
Abstract
Urinary incontinence (UI) is a common symptom affecting almost one-third of adult women. UI can occur because of hypermobility or intrinsic sphincter deficiency of the urethra. Regardless its etiology, it is associated with poor quality of life and most of the incontinent women develop symptoms such as anxiety, depression, and social isolation over time. The synthetic midurethral sling (MUS) was first introduced in 1995 and quickly became the gold standard treatment for women with stress UI because of intrinsic sphincter deficiency and/or urethral hypermobility. This session addresses the indications, preoperative preparation, surgical steps, postoperative care, and complications related to synthetic MUSs. Owing to the exponential increase in the prevalence of mesh-related complications, we also developed a rational evidence-based algorithm that will help urologists to diagnose and manage this specific subset of patients.
Indications
Midurethral Slings (MUSs) are indicated for women with stress urinary incontinence (SUI), mixed urinary incontinence (UI), and predominant SUI component, or pelvic organ prolapse and occult SUI. 1
Preoperative preparation
Preoperative urinalysis and culture must demonstrate no evidence of urinary tract infection. Topic estrogen can be prescribed 4 to 6 weeks preoperatively in postmenopausal women with vaginal atrophy and no contraindications. Patients taking low-dose aspirin do not need to stop taking medication. All patients should be advised about UI recurrence, postoperative urinary retention, and mesh-related complications. A special consent for mesh use is advised after an informed consent to the patient regarding the FDA notification.
Patient Positioning
MUSs are performed with the patient in the dorsal lithotomy position. Cushion-leg support is advisable to minimize calf compression and prevent postoperative deep vein thrombosis (Fig. 1).

Dorsal lithotomy position.
Retropubic MUS: Surgical Steps
Step 1
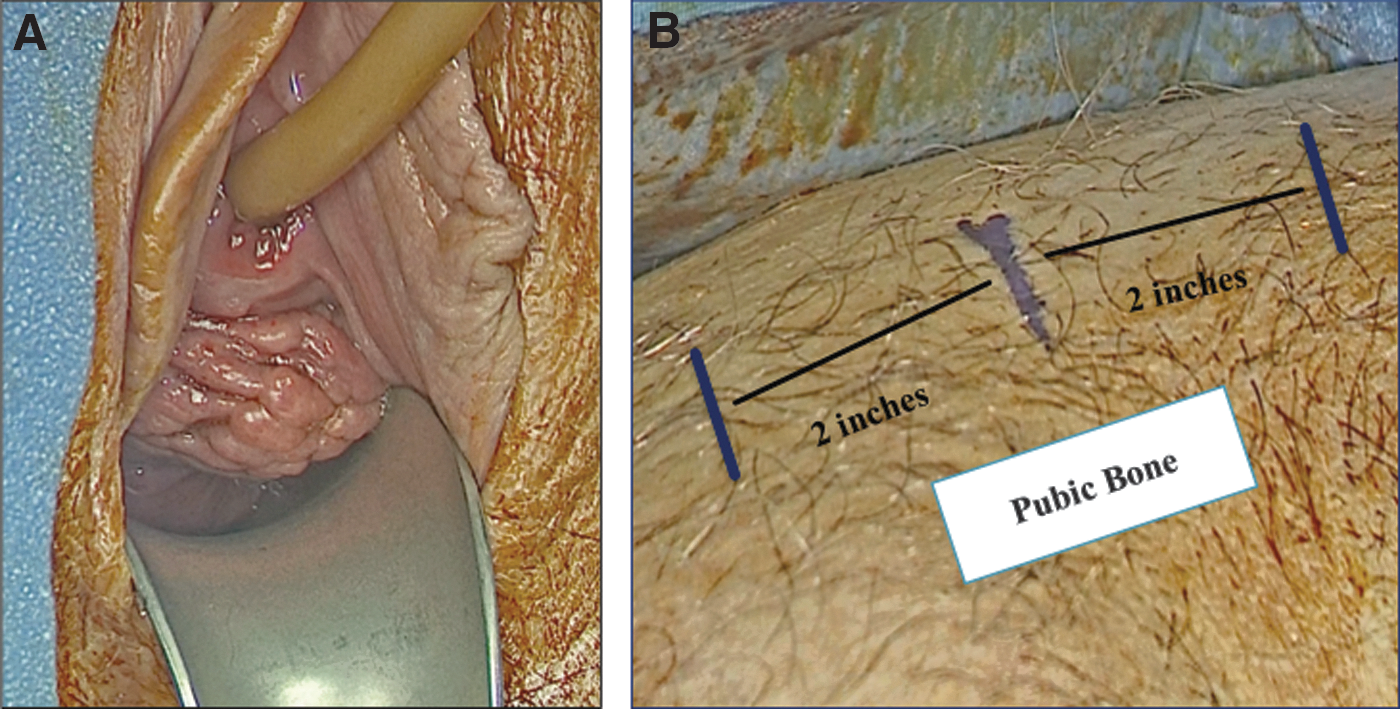
A weighed speculum is lubricated and inserted into the vagina. Then, an 18F Foley catheter is placed into the urethra and bladder is emptied. Three incision marks are done in the suprapubic area: one in the midline and two located 2 inches from the midline on each side (see Supplementary Video S1; Supplementary Data are available online at
Step 2
To minimize the risk of bladder perforation during the passage of the trocar sheath, a retropubic hydrodissection is advisable. A 20-gauge spinal needle is inserted along the posterior surface of the pubic symphysis until the needle touches the endopelvic fascia. Then, the needle is pushed 12 inches back and 20 mL of local anesthesia is injected on each side (see Supplementary Video S2; Fig. 3).
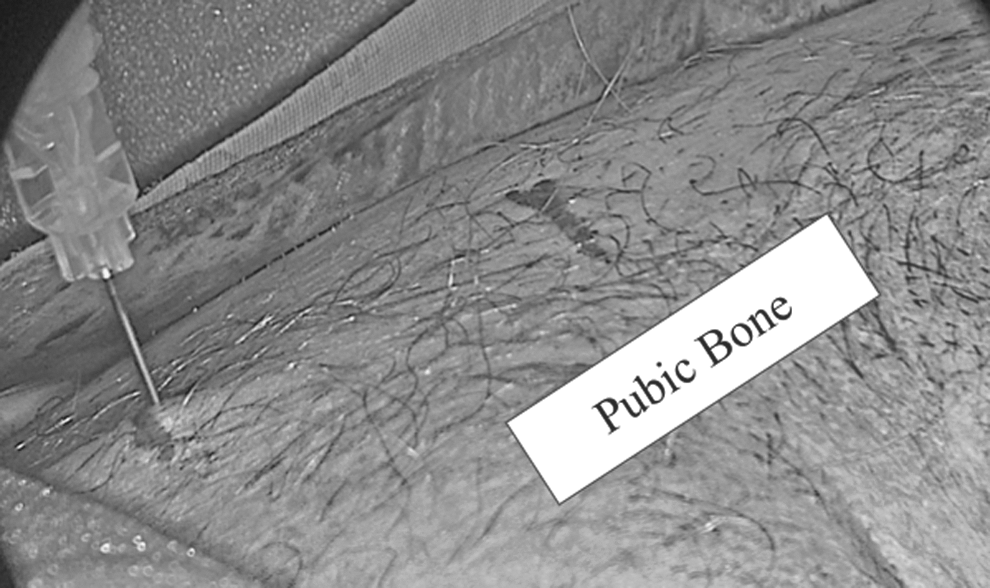
Retropubic hydrodissection.
Step 3
Saline is injected into the submucosa at the level of midurethra to create a space between the vaginal wall and the periurethral fascia to facilitate the dissection (see Supplementary Video S3; Fig. 4).
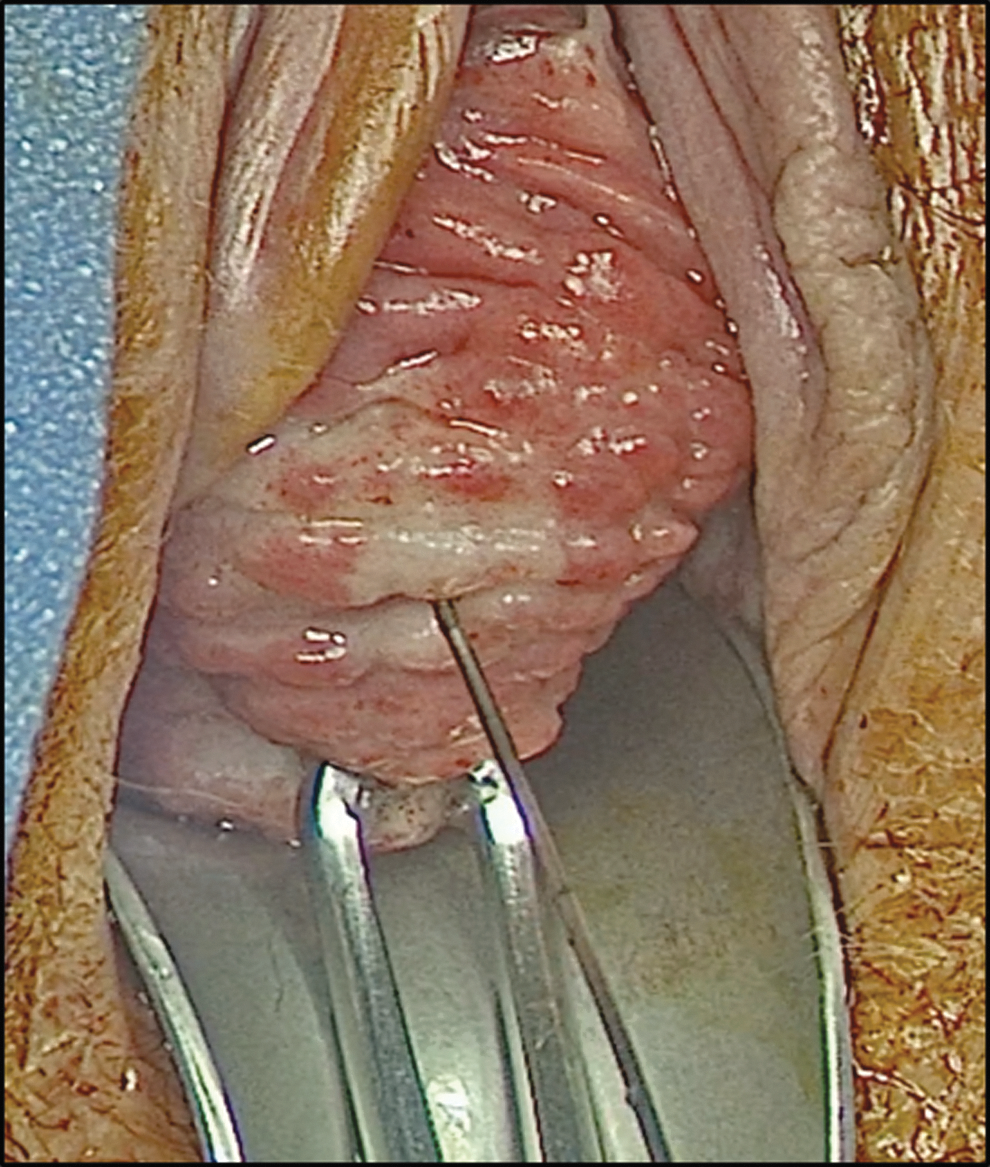
Vaginal submucosa injection.
Step 4
A 2-cm longitudinal midline incision is performed at the level of midurethra, ∼1 cm above the urethra meatus. Two Allis clamps are placed on each side of the incision for traction and better exposure. Using Metzenbaum scissors, we dissected the vaginal mucosa laterally along the periurethral fascia toward the patient's ipsilateral shoulder. This procedure is repeated on the contralateral side (see Supplementary Video S4; Fig. 5).
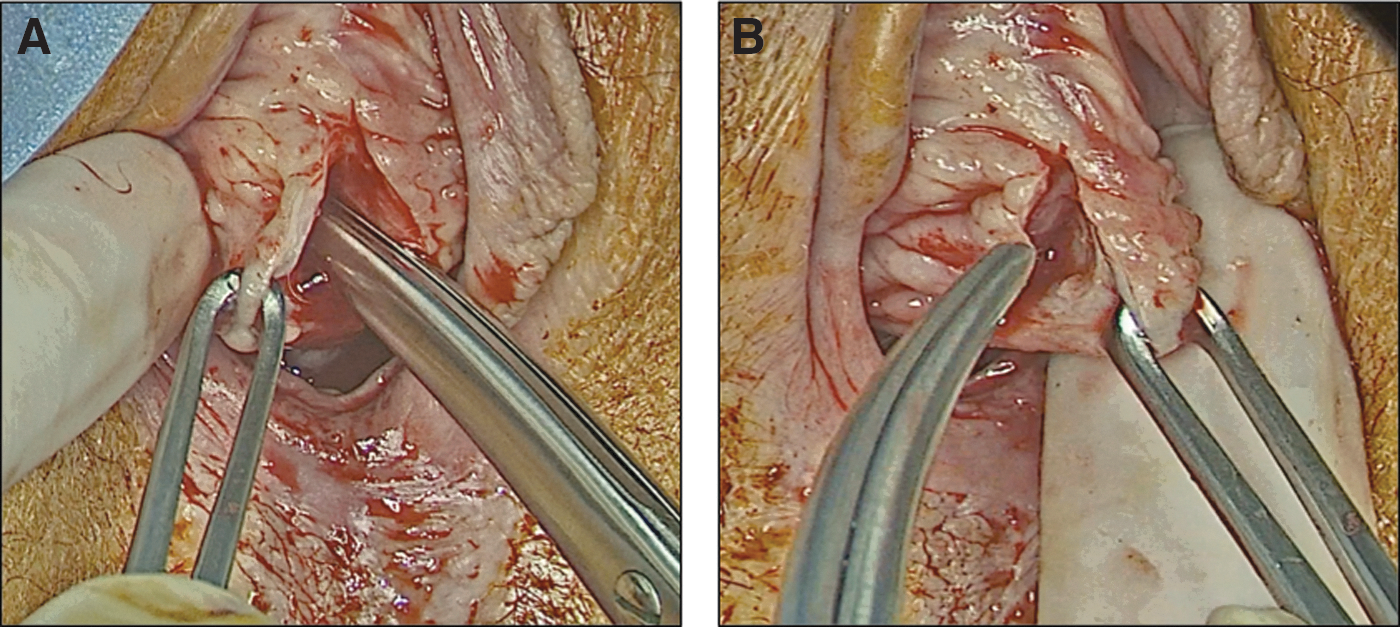
Midline incision at the level of midurethra and dissection of vaginal mucosa on the right side
Step 5
To control the insertion of the trocar sheath, an index finger is placed in the vagina under the anterior vaginal wall laterally to the suburethral incision. The tip of the trocar sheath is oriented horizontally toward the patient's ipsilateral shoulder. Before perforating the endopelvic fascia, the trocar sheath tip should stay in close contact with the posterior surface of the pubic symphysis. Then, the sheath is advanced through the endopelvic fascia, retropubic space, rectus fascia, and skin (see Supplementary Video S5; Fig. 6).

Step 6
With the trocar sheath in place, cystoscopy is performed to assure that both trocars do not cause any inadvertent injury to the bladder or urethra. During cystoscopy, both trocars are mobilized to confirm their position (see Supplementary Video S6; Fig. 7).
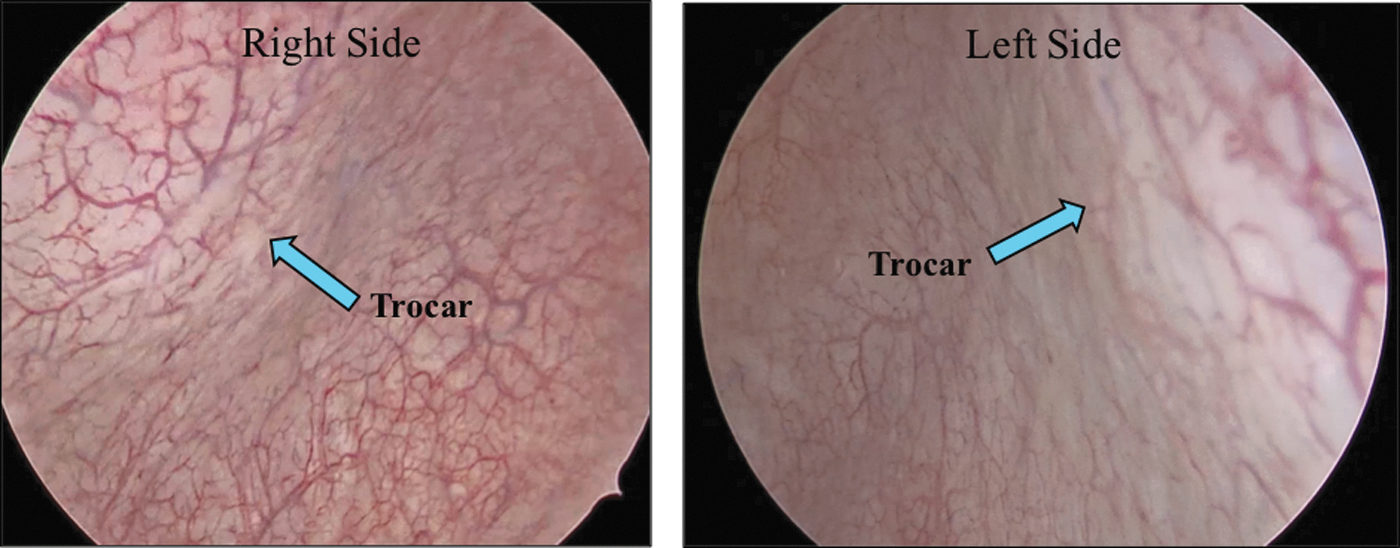
Cystoscopy demonstrating trocar sheath position on both sides and no evidence of bladder injury.
Step 7
Before advancing the mesh, it is imperative to empty the bladder to avoid shearing a full bladder with the mesh. In the absence of inadvertent injury, both trocar sheaths are pulled upward to bring the sling loosely without twisting it under the midurethra. Once the sling is on the right place, the blue tag is cut off. To adjust the sling tensioning, a right-angle clamp is placed between the sling and urethra to stabilize the sling during sheath removal. Ultimately, both plastic sheaths surrounding the Prolene mesh are removed (see Supplementary Video S7; Fig. 8).

Step 8
The vaginal wall is closed with running absorbable suture. Suprapubic skin is closed with skin glue and vaginal packing soaked in antibiotic ointment is inserted into the vagina (see Supplementary Video S8; Fig. 9).
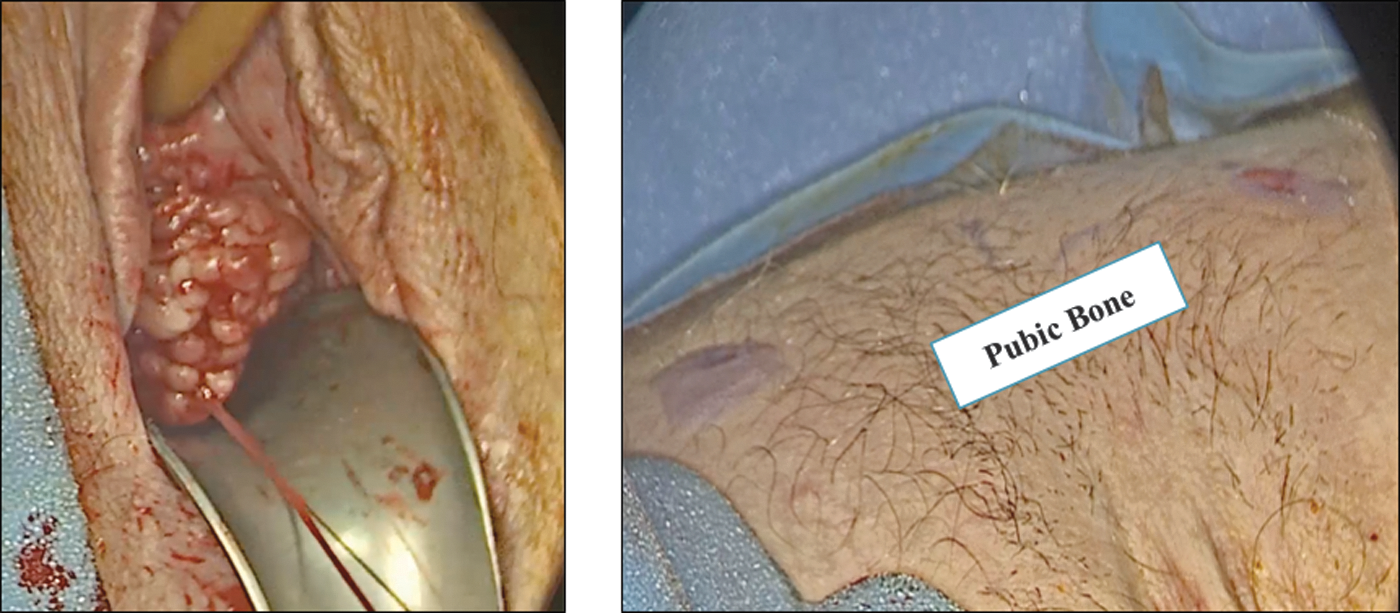
Vaginal wall closure and skin glue.
Troubleshooting during surgery
The retropubic space (space of Retzius) contains connective and adipose tissue. The obturator vessels, which are the closest major vascular structure, are located ∼3 cm laterally to the midline on each side. The left and right dorsal nerves of the clitoris run along the inferior surface of the ischiopubic rami and cross under the pubic bone 1 to 2 cm from the midline. Anteriorly, this space is bounded by rectus abdominis muscles, pubic symphysis, and ischiopubic rami. The lateral borders are the bony pelvis and the obturator internus muscle. The inferolateral boundary of the space of Retzius is the endopelvic fascia, which separates the prevesical space from the vesicovaginal space. Medially, the endopelvic fascia is attached to the levator ani muscles and laterally is attached to the arcus tendineous and the ischiopubic rami. The proximal urethra and bladder lie posterior to this space.
Overall, the rate of intraoperative complications associated with MUS ranges from 2% to 3%. The most common reported complications are (1) bladder perforation, (2) vascular injury (bleeding and/or hematoma), and (3) urethral injury.
To minimize the risk of intraoperative bladder perforation, the bladder must be completely emptied before trocar placement. Most cases of bladder perforation occur at 2 and/or 10 o'clock positions. Cystoscopy with both trocar sheaths in place is highly recommended to confirm the integrity of the bladder. If bladder perforation is noted, the trocar must be withdrawn and carefully passed again to avoid further perforation. In these cases, patients should be discharged with the urethral catheter, which will be withdrawn 7 to 10 days postoperatively.
Intraoperative bleeding is less common than bladder perforation. Most cases can be managed with observation and local compression. It is advisable to certify patient anticoagulation status before intervention.
Intraoperative urethral injury occurs more frequently with transobturator slings. In all cases of urethral injury, urethra must be repaired and Foley catheter maintained for 7 to 10 days postoperatively. In these cases, synthetic MUS should be postponed because of the risk of mesh-related complications. 2,3
Postoperative Care
MUS is an outpatient surgery (23 hours stay). The urethral catheter, vaginal packing, and intravenous line are all taken out in the morning after surgery. Oral antibiotics, stool softener, and pain medication are given as required. Normal activities such as walking and driving are allowed after hospital discharge. Impact exercises and sexual intercourse should be avoided for 1 month postoperatively.
Management of Postoperative Complications
Failure to void after urethral catheter removal
The urethral catheter is removed before hospital discharge and patients are instructed to void. Those who are not able to void are discharged to home with the catheter in place and followed in the outpatient clinic 48 hours later. Before coming to the clinic, they are instructed to take the urethral catheter out at home. If urinary retention persists, they are instructed to perform clean intermittent catheterization or can be referred to the operating room for sling tensioning readjustment. 4
Voiding dysfunction after MUS
Overall, persistent voiding dysfunction after sling placement is the result of bladder outlet obstruction. Clinically, patients can present with urgency/frequency, incomplete bladder emptying, and high postvoid residual urine, or urinary retention. Cystoscopy is recommended in all patients to rule out bladder pathologies, hypersuspended bladder neck, and mesh-related complications. Urodynamic study is a useful examination that should be performed at the physician's discretion. 5
Cutting the sling in the midline through a single vertical incision is the recommended approach to manage voiding dysfunction associated with tight sling within the first 3 months after surgery. After 3 months, the sling is fixed along its entire course, hindering its removal through a midline incision. In these cases, urethrolysis and sling excision are indicated.
Slings placed in the wrong location, more specifically, at the level of proximal urethra should be removed regardless the surgery timeframe. The best time to perform a “new” MUS should be at physician's discretion. 6,7
Mesh-related complications
Extensive data exist in the literature supporting the use of synthetic mesh slings for the treatment of SUI in women. The main advantages are shorter operative time and hospital stay, minimal postoperative pain, and less urinary retention when compared with fascial slings. Mesh-related complications such as mesh exposure and mesh perforation can occur after synthetic sling placement, but the rate is acceptably low (2%).
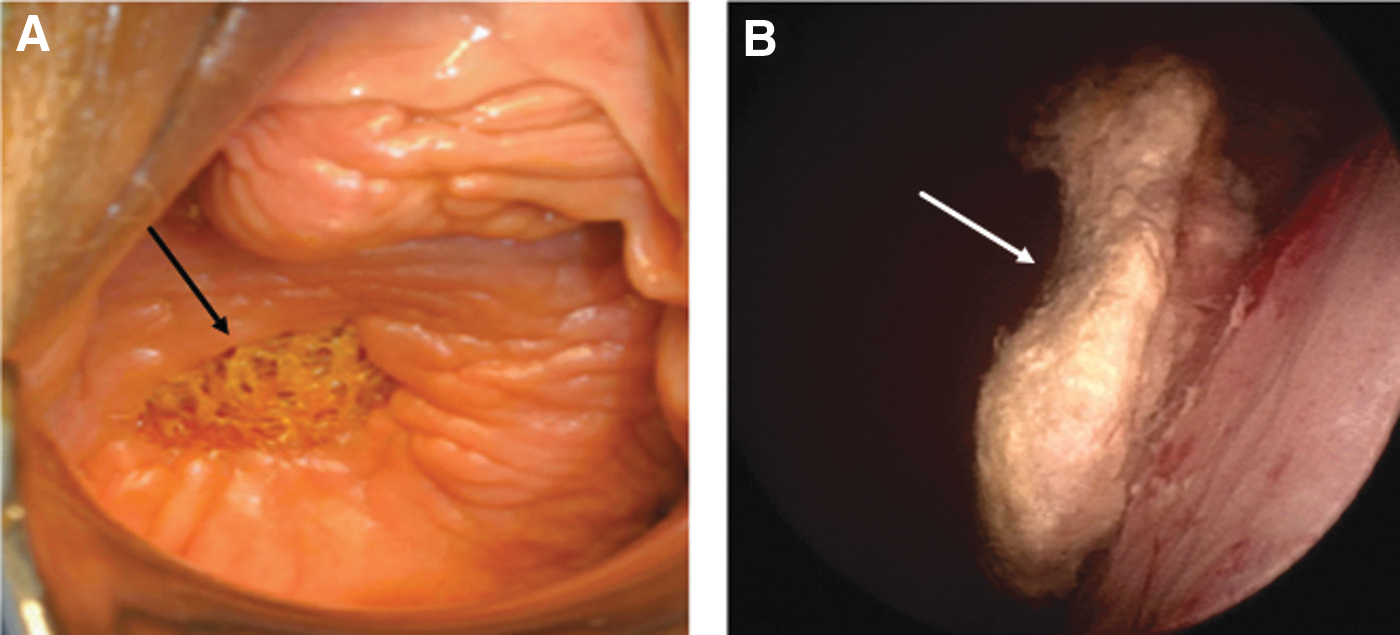
The American Urological Association (AUA), European Association of Urology (EAU), as well as Society of Urodynamics, Female Pelvic Medicine, and Urogenital Reconstruction (SUFU) support the use of synthetic MUS for the treatment of women with SUI. However, before the procedure, they recommend that all patients should be advised about the risks and benefits of mesh slings as well as other therapeutic approaches. A rational algorithm to address mesh-related complications is depicted hereunder (Fig. 10). Figure 11 shows an example of vaginal exposure and intravesical mesh calcification.
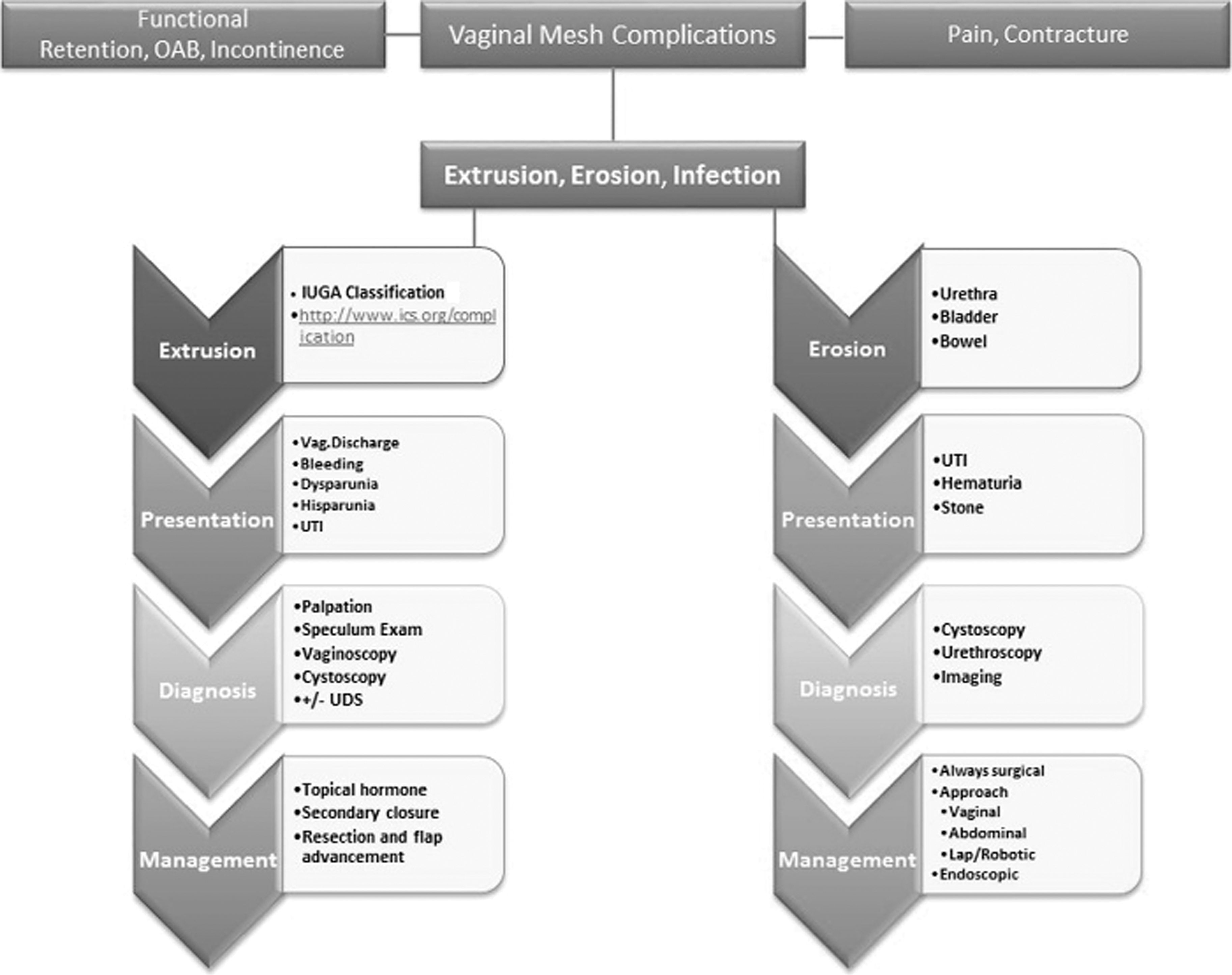
Algorithm for mesh-related complications.
The AUA position statement is available at
(
(
There is also an FAQ available through
(
To view full video, “MUS AtlasofMinimallyInvasive Urologic Surgery.mp4,” click here.
Footnotes
Author Disclosure Statement
No competing financial interests exist.