
Abstract
Objective:
The objective of this meta-analysis was to compare the efficacy and safety of externalized ureteral catheter (EUC) and Double-J stent (DJS) in tubeless percutaneous nephrolithotomy (PCNL) for patients with upper urinary stones based on published literature.
Materials and Methods:
A comprehensive literature search using Pubmed, Embase, and Cochrane Library was performed to find studies comparing outcomes of EUC and DJS for treating patients with upper urinary stones up to December 2017. Seven studies, which included 863 patients from 5 randomized controlled trials (RCTs) and 2 non-RCTs published between 2009 and 2017, met our inclusion criteria and were included in this systematic review and meta-analysis. Between-studies heterogeneity was assessed and sensitivity analysis was conducted based on RCTs.
Results:
The stent-related symptoms were higher for DJS compared with EUC (odds ratio [OR]: 0.09; confidence interval [95% CI]: 0.01–0.61; p = 0.01). No significant differences were found in minor (Clavien I–II) complications (OR: 1.37; 95% CI: 0.93–2.01; p = 0.11), major (Clavien III–V) complications (OR: 1.38; 95% CI: 0.73–2.60; p = 0.32), hemoglobin drop (weighted mean difference [WMD]: −1.43 g/L; 95% CI: −3.65 to 0.78; p = 0.2), pain score (VAS) (WMD: 0.01; 95% CI: −0.28 to 0.29; p = 0.95), analgesic required (OR: 1.02; 95% CI: 0.77–1.34; p = 0.91), stone-free rate (risk ratio: 0.98; 95% CI: 0.9–1.07; p = 0.67), duration of hospitalization (WMD: −0.21 days; 95% CI: −0.86 to 0.44; p = 0.53), and operative times (WMD: −7.59 minutes; 95% CI: −18.81 to 3.64; p = 0.19).
Conclusion:
We concluded that compared with DJS, EUC is also an effective alternative for patients with upper urinary stones in tubeless PCNL and could help patients by reducing stent-related discomfort and avoiding cystoscopy for DJS removal. However, the inherent limitations of the included studies should be considered, and well-designed RCTs with further large sample size should be performed to validate our findings.
Introduction
O
In the past, some recent studies 3 –9 aimed to compare differences of DJS and EUC in tubeless PCNL for surgical treatment of patients with upper urinary stones. Gonen and colleagues 6 showed that tubeless PCNL with EUC is as feasible and safe as DJS. More importantly, compared to DJS, EUC could help patients by reducing stent-related discomfort and avoiding cystoscopy for DJS removal. Although Telha and colleagues 5 reported that tubeless PCNL with DJS was the optimal minimally invasive procedure to decrease the complications and duration of hospitalization compared to EUC, the small samples in each study were limiting and unable to make a strong conclusion. So far, no meta-analysis has investigated the outcomes of these two procedures. Therefore, whether EUC in tubeless PCNL is safer or more effective when compared to the DJS remains unsettled.
We aim to provide systematic information on the comparison of outcomes of EUC vs DJS, to summarize the existing evidence in our meta-analyses, and to provide higher level of evidence (LOE) about this topic for guidelines. We hope it may guide urologists and patients to decide on the treatment modality, and to select the optimal invasive surgical treatment technique.
Materials and Methods
A comprehensive prospective protocol, including objectives, search strategy, inclusion and exclusion criteria, study selection, data extraction, quality assessment, and statistical analysis, was preconditioned according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis. 10
Search strategy
A comprehensive literature strategy search was performed by two members (Wu and Zhang) independently in December 2017. The PubMed, Embase, and the Cochrane Library databases were used to obtain relevant studies up to December 2017. The search terms used were “externalized ureteral catheter” and “‘Double-J stent’ or ‘ureteral stent’” in combination with “‘tubeless percutaneous nephrolithotomy’ or ‘tubeless PCNL’ or ‘tubeless PNL’.”
Inclusion and exclusion criteria
The relevant studies were included according to the following criteria: (1) comparative studies reported comparison between EUC and DJS in patients with upper urinary stones; (2) the outcome measures consisted of at least two of the following things: complications, hemoglobin drop, pain score (VAS), analgesic required, stone-free rate (SFR), duration of hospitalization, and operative times. Exclusion criteria are as follows: (1) repeated publications or conference proceedings; (2) nonpublished materials, editorials, or reviews; (3) studies containing patients with partial or complete staghorn calculi, serious urinary infection, renal insufficiency, musculoskeletal deformities, or congenital abnormalities. Eligible study content and quality assessment, and data extractions were performed by two investigators (Feng and Yue) independently, and disagreements were resolved by open discussion.
Study selection and data extraction
We screened eligible studies based on above-mentioned inclusion and exclusion criteria. We contacted the corresponding authors of relevant studies through email to supplement missing or unavailable data. The extracted data included baseline characteristics (first author, year of publication, study period and design, cases, gender, age, weight/body mass index, and mean stone size), perioperative outcomes (interventions, operative times, and complications), and postoperative outcomes (minor/major complications, hemoglobin drop, pain score (VAS), analgesic required, SFR, and duration of hospitalization).
Quality assessment and statistical analysis
Criteria provided by the Oxford Centre for Evidence-based Medicine 11 was applied to assess the LOE for all included studies. Also, the quality of nonrandomized controlled trials (non-RCTs) was assessed by Newcastle-Ottawa Scale (NOS). 12 In addition, the Cochrane risk of bias tool was applied to assess the methodological quality of RCTs. 13 All statistical analyses were performed using software RevMan (version 5.3; Cochrane Collaboration, Oxford, United Kingdom). For continuous and dichotomous variables, weighted mean difference (WMD) and odds ratio (OR)/risk ratio (RR) were calculated with associated 95% confidence intervals (CIs), respectively. The I 2 statistics with associated 95% CI and χ 2 p-values were used to assess between-studies heterogeneity. A fixed-effect model was adopted if heterogeneity was not significant (p > 0.10, I 2 < 50%); otherwise, random effect will be applied. 13 Forest graphs were applied to express the results of the meta-analysis. The Z-test determined the pooled effects, and only p < 0.05 was taken into account as a statistically significant difference. The potential publication biases were expressed using Funnel plots. Sensitivity analysis was conducted based on RCTs. Only outcomes with three or more than three eligible studies were included in the sensitivity analysis.
Results
Of 108 available studies obtained by the literature search strategy, 7 studies, 3 –9 which included 863 patients from 5 RCTs and 2 non-RCTs (429 cases for EUC and 434 cases for DJS), fulfilled the above-mentioned inclusion criteria and were included in the final analysis (Fig. 1). A flowchart of the study selection process is presented as Figure 1, whereas Table 1 summarizes the baseline characteristics and quality assessment of all included studies. Among seven included studies available for meta-analysis, two 4,7 were non-RCTs (LE: 3b) and another five 3,5,6,8,9 were RCTs (LE: 2b). The methodological quality of included studies was relatively high for all the non-RCTs (NOS: 6 of 9 points), and the RCTs were high quality for 5 points (the Cochrane risk of bias tools: score from 0 to 7).
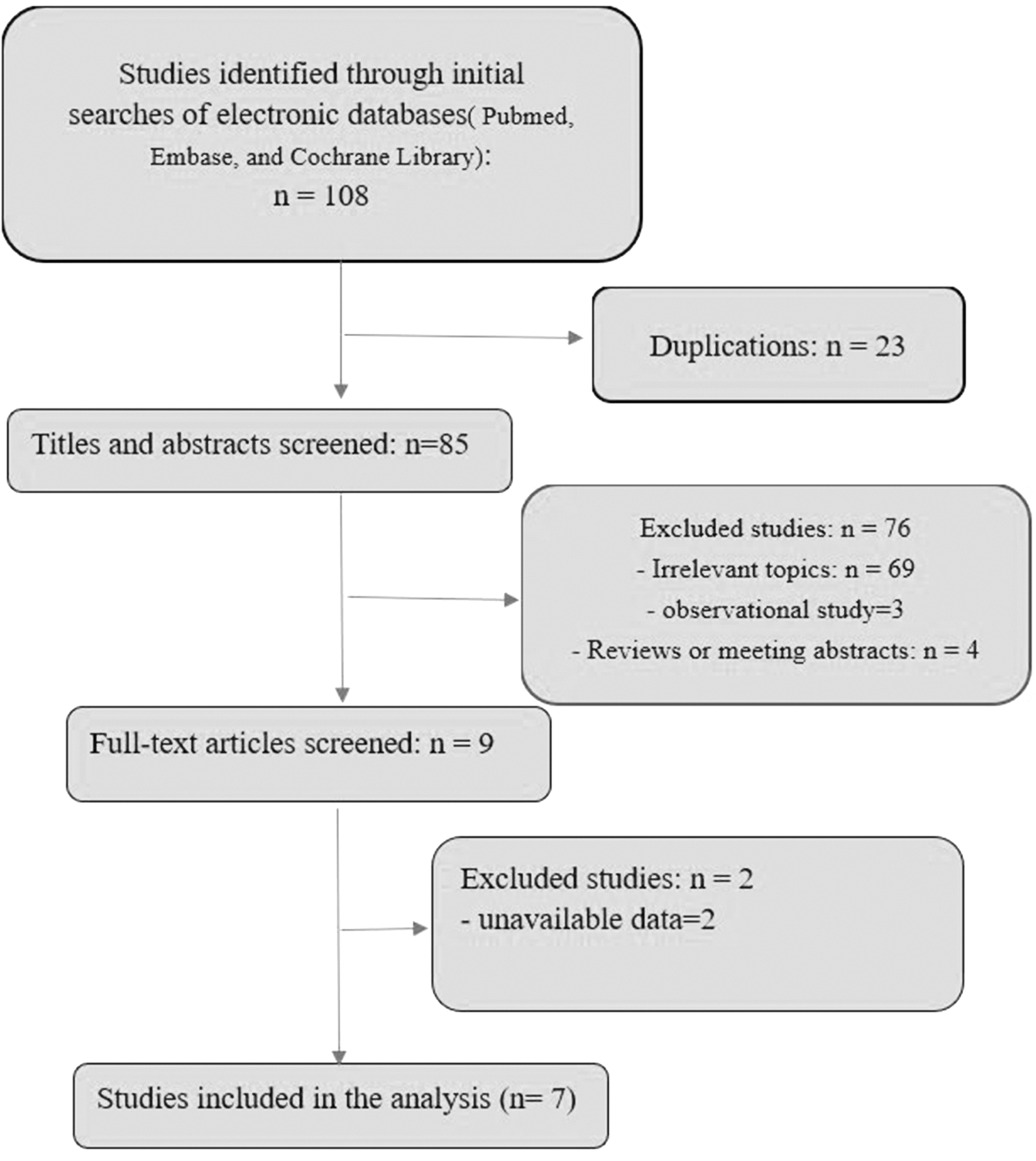
Flow diagram of studies identified, included, and excluded.
Using The Cochrane collaboration's tool (score from 0 to 7).
Using Newcastle-Ottawa Scale (score from 0 to 9).
BMI = body mass index; DJS = Double-J stent; EUC = externalized ureteral catheter; LOE = level of evidence; RCCS = retrospective case–control study; RCT = randomized controlled trial.
Outcome
Data on minor (Clavien I–II) complications were available in seven studies, 3 –9 which evaluated 868 patients (Fig. 2a). Meta-analysis of the seven studies indicated that no significant difference was found in minor complications between groups with EUC and DJS (OR: 1.37; 95% CI: 0.93–2.01; p = 0.11, p heterogeneity = 0.4, I 2 = 3%). Five studies 3 –6,9 reported major (Clavien III–V) complications (Fig. 2b). No significant difference was found in major complications between groups with EUC and DJS (OR: 1.38; 95% CI: 0.73–2.60; p = 0.32, p heterogeneity = 0.26, I 2 = 24%).

Forest plot and meta-analysis of minor complications
Two studies 6,9 assessed 155 patients and reported on stent-related symptoms (Fig. 2c) between the two groups favoring the EUC (OR: 0.09; 95% CI: 0.01–0.61; p = 0.01, p heterogeneity = 0.16, I 2 = 50%).
Four studies 3,6 –8 that assessed 343 patients reported on hemoglobin drop (Fig. 2d). There was no significant difference between groups with EUC and DJS (WMD: −1.43 g/L; 95% CI: −3.65 to 0.78; p = 0.2, p heterogeneity <0.00001, I 2 = 90%).
Data on pain score (VAS) were available in 5 studies, 3,4,6,8,9 which evaluated 551 patients (Fig. 3e). Meta-analysis of the five studies indicated that no significant difference was found in postoperative pain score between groups with EUC and DJS (OR: 0.01; 95% CI: −0.28 to 0.29; p = 0.95, p heterogeneity = 0.97, I 2 = 0%). Data on analgesic required were available in 5 studies, 3,4,7 –9 which evaluated 873 patients (Fig. 3f). Meta-analysis of the five studies indicated that there was no significant difference between groups with EUC and DJS (OR: 1.02; 95% CI: 0.77–1.34; p = 0.91, p heterogeneity = 0.49, I2 = 0%).
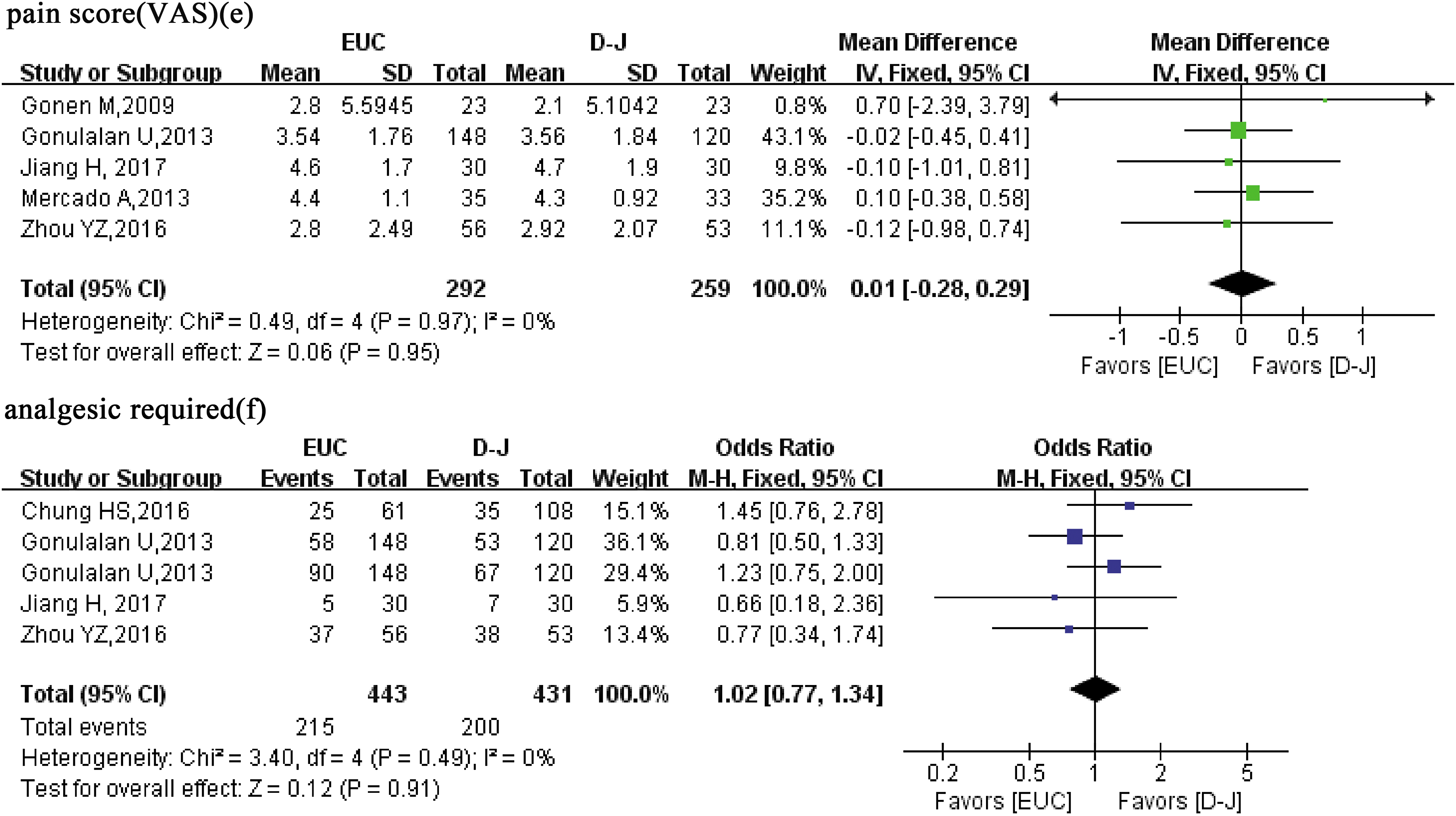
Forest plot and meta-analysis of postoperative pain score (VAS)
Five studies 4,5,7 –9 that assessed 652 patients reported on operative times (Fig. 4g). There was no significant difference between groups with EUC and DJS (WMD: −7.59 minutes; 95% CI: −18.81 to 3.64; p = 0.19, p heterogeneity <0.00001, I 2 = 86%). Data on duration of hospitalization were available in 6 studies, 3,4,6 –9 which evaluated 720 patients (Fig. 4h). Meta-analysis of the six studies indicated that no significant difference was found in hospitalization times between groups with EUC and DJS (WMD: −0.21 days; 95% CI: −0.86 to 0.44; p = 0.53, p heterogeneity <0.00001, I 2 = 87%).

Forest plot and meta-analysis of operative times
Five studies 3,4,6 –8 that assessed 611 patients reported on SFR and no significant difference was found between groups with EUC and DJS (RR: 0.98; 95% CI: 0.9–1.07; p = 0.67, p heterogeneity = 0.009, I 2 = 50%) (Fig. 4i).
When RCTs 3,5,6,8,9 were assessed, no change in terms of the significance difference of each of outcomes except for hemoglobin drop. Meta-analysis of three RCTs 3,6,8 revealed that EUC in tubeless PCNL for surgical treatment of patients with upper urinary stones provided a significantly lower hemoglobin drop compared with DJS. Between-study heterogeneity was significantly reduced for major (Clavien III–V) complications, hemoglobin drop, operative times, and SFR, whereas heterogeneity remained statistically significant in hospitalization times (Table 2).
CIs = confidence intervals; OR = odds ratio; WMD = weighted mean difference.
Publication bias outcomes
Funnel plots were conducted to assess the publication bias in this meta-analysis that reported minor complications (Fig. 5). All studies lie inside the 95% CIs and distribute around the vertical, indicating no obvious publication bias.

Funnel plot for assessing publication bias.
Discussion
This meta-analysis of 5 RCTs and 2 non-RCTs, including 863 patients, comparing outcomes of DJS and EUC in tubeless PCNL showed that no significant differences were found in minor (Clavien I–II) complications, major (Clavien III–V) complications, hemoglobin drop, pain score (VAS), analgesic required, SFR, hospitalization times, and operative times. However, the stent-related symptoms were higher for DJS in tubeless PCNL compared with EUC.
The safety of the patients is an important parameter for the application of any new procedure. Gonen and colleagues 6 reported that using an EUC instead of a DJS for postoperative drainage did not increase postoperative complications of the tubeless PCNL. Similarly, Zhou et al. 9 reported the results from 109 patients with upper urinary stones, who underwent tubeless PCNL, to analyze and compare the outcomes of using EUC vs DJS in tubeless PCNL. They found no statistically significant differences between the two groups regarding morbidity. However, Telha et al. performed an RCT, including 148 cases with kidney stones, and found that tubeless PCNL with DJS was the optimal minimally invasive procedure with less postoperative complications compared to EUC. In the DJS group, the complications were postoperative hematuria (8.3%), urine leakage (5.6%), and postoperative fever (2.8%), whereas the complications of EUC group were leakage of urine (17.1%), postoperative hematuria (11.8%), fluid collections (10.5%), postoperative fever (6.6%), and postoperative colonic injury (1.3%). Our meta-analysis of seven studies revealed that no significant difference in minor (Clavien I or II) and major (Clavien III–V) complications was found between EUC and DJS in tubeless PCNL. On sensitivity analysis of RCTs, outcomes were consistent with overall results.
DJS is the most common form of internal drainage in the urinary surgery. 14 Several studies 15,16 have confirmed the safety and efficacy of tubeless PCNL with DJS. However, stent-related discomfort should not be ignored. In a recent study, 17 30% of the patients who underwent tubeless PCNL had stent-related discomfort, and 60% of them needed antispasmodics and/or analgesics for symptom relief. DJS placement also has a disadvantage as requirement of additional cystoscopy for removal, increasing the cost of treatment and psychologic stress for the patient. These shortcomings led to modifications of tubeless PCNL, including indwelling EUC instead of DJS. In 2001, a 6F EUC was first used for 48 hours in PCNL and demonstrated that this technique in selected patients could reduce postoperative discomfort without increasing complications. 18 In 2009, Gonen and colleagues 6 explored differences between EUC and DJS in tubeless PCNL in 46 patients. The only statistically significant difference between two groups was found in postoperative stent-related symptoms. Therefore, they concluded that tubeless PCNL with EUC is an effective alternative for patients with upper urinary stones and could g by reducing stent-related discomfort and avoiding cystoscopy for DJS removal. Our meta-analysis also revealed that the EUC group presented fewer postoperative stent-related symptoms compared with the DJS group. Those differences are likely to translate into clinical significance.
SFR represents an important parameter when evaluating the efficacy of minimally invasive procedure in the treatment of patients with upper urinary stones. Five studies 3,4,6 –8 reported data on SFR. Also, the SFR in EUC groups ranged from 80% to 93.3%. Meta-analysis of the five studies indicated that no significantly difference was found in SFR between EUC and DJS.
There were five studies that provided the data of pain score (VAS); the pooled data revealed that no significant difference was found between groups with EUC and DJS. Our pooled data also demonstrated that no significant difference between EUC and DJS was found in analgesic required. Pooled analysis of these studies revealed that no significant difference in operative times and hospitalization times was found between EUC and DJS. In fact, even nuances in the surgical technique and surgical experience could affect related operative times. Percutaneous methods showed variations in image guidance, access, type of dilator, type of lithotripsy, and postoperative stent. Therefore, our cumulative data demonstrated that EUC turns out to be a safe and feasible alternative to DJS for patients with upper urinary stones in selected cases.
Our meta-analysis has several limitations, which should be taken into consideration when interpreting the results. First of all, two studies were retrospective studies. These results should be interpreted with caution, given the potential for selection and treatment bias attributable to the inherent limitations of retrospective study. Between-studies heterogeneity was found to be high for several outcomes, including hemoglobin drop, operative times, duration of hospitalization, and SFR. Although heterogeneity was significantly reduced by the sensitivity analysis for hemoglobin drop, operative times, and SFR, it still remained statistically significant in the duration of hospitalization. The heterogeneity can be explained by the difference in surgical technique and surgical experience, and outcome definitions. The surgical technique for EUC and DJS, the diameters and location of stones, and stent implantation were not similar across the different studies. Overall, only seven studies could be included into final analysis. Also, such a small number of studies were unable to make a strong conclusion. Thus, well-designed RCTs with further large sample size should be performed to validate our findings.
Conclusion
In conclusion, compared with DJS, EUC in tubeless PCNL is also an effective alternative for patients with upper urinary stones in selected cases, with the following benefits: reduced stent-related discomfort and avoided cystoscopy for DJS removal. Also, well-designed RCTs with further large sample size are awaited to validate and update the findings of our analysis.
Footnotes
Author Disclosure Statement
No competing financial interests exist.