
Abstract
Objective:
The increasing number of flexible ureterorenoscopy (fURS) procedures, the fragility of devices, and their growing repair costs represent a substantial burden for urological departments worldwide. No risk factors of flexible ureteroscope damage have been identified so far. The objective of this study was to investigate the impact of infundibulopelvic angle (IPA) on device damage and on other intraoperative and postoperative factors such as length of hospital stay, surgical complications, stone-free rate (SFR), operation, and fluoroscopy time.
Materials and Methods:
In a retrospective monocentric study, IPA was measured based on intraoperative retrograde pyelography images taken during fURS. All procedures were conducted with modern reusable flexible ureteroscopes: Karl Storz Flex-X2 or Olympus URF-V. Statistical analysis was performed in RStudio (version 1.0.136) with the unpaired t-test and Mann–Whitney U test. Pearson correlation coefficient (Pearson's r) was measured whenever applicable.
Results:
In total, 381 fURS performed between September 2013 and March 2017 were analyzed: 260 (68.24%) for kidney stone operation and 121 (31.76%) for diagnostic purposes; of these, 38 (9.97%) devices were postoperatively deemed defective. IPA values were significantly steeper in cases with flexible ureteroscope damage compared to cases without damage (median 42.5 degrees vs 56.0, p < 0.001). Steeper IPA was significantly associated with the occurrence of Clavien-Dindo ≥2 complications (median 51.0 degrees vs 55.0, p = 0.005) as well as prolonged hospital stay (median 51.0 degrees vs 55.0, p = 0.014). No influence on SFR was observed (p > 0.05). IPA did not correlate with operation or fluoroscopy time.
Conclusions:
Steep IPA can be considered the first risk factor predicting both flexible ureteroscope damage and an unfavorable postoperative course. A better understanding of damage mechanisms is the key for the proper indications to use costly single-use devices.
Introduction
M
The fragility of flexible ureteroscopes, a growing number of procedures worldwide, as well as the associated maintenance and repair costs, are important economic and logistic challenges for endourologic centers performing fURS procedures. 6 –8 Despite many improvements over the past years, such as miniaturization, passive and active flexion, and digital imaging, the susceptibility to intraoperative damage is still high and has become a major point of scientific interest over recent years.
The identification of risk factors of reusable flexible ureteroscope damage would be beneficial in terms of identifying indications for disposable fURS, to decrease the rates of reusable fURS device damage. Our own data and experience suggest that extreme flexion of the tip of fURS devices to overcome a steep infundibulopelvic angle (IPA) and reach the lower kidney pole could play a role in fURS damage mechanism. 9
The substantial influence of IPA on radiologically confirmed stone-free rate (SFR) as well as stone clearance after fURS and shockwave lithotripsy (SWL) procedures was already confirmed in retrospective 10 –13 as well as prospective studies. 14 Based on those findings, the steep IPA was recognized in the Guidelines of the European Association of Urology as a factor that negatively influences stone clearance from the lower kidney pole after SWL procedures. 3
The aim of this study was to investigate whether the IPA would play a role as a risk factor of fURS device damage. The relationship of IPA to other intraoperative and postoperative factors such as complication rate, fluoroscopy time, and length of hospital stay (LOS) has also been studied.
Materials and Methods
Our retrospective monocentric study was based on 381 fURS cases performed between September 2013 and March 2017 at the Department of Urology, University Hospital Schleswig-Holstein (Luebeck, Germany). Written patient consent was obtained. Preoperative antibiotic therapy was applied only in patients with positive preoperative urine culture. Patients were operated under general anesthesia in supine lithotomy position. All procedures were conducted with modern reusable flexible ureteroscopes: Karl Storz Flex-X2 and Olympus URF-V.
In the majority of cases, fURS was preceded by semirigid ureterorenoscopy (URS).
The IPA was measured based on intraoperative retrograde pyelography (RPG) images. Contrast (Urolux Retro®; CS Diagnostics GmbH) was usually injected into the proximal ureter through the semirigid ureteroscope, before the application of fURS devices. Stone lithotripsy was conducted with SlimLine 200 μm Fiber (Boston Scientific) and Holmium Laser (Lumenis VersaPulse® PowerSuite™ 100 W). Uromed Stonizer® tipless (1.9F) or NGage® (2.2F) nitinol baskets were used for kidney stone extraction. Tissue biopsies were performed with Olympus FB 56D-1 (1.2 mm) or Karl Storz (3.0F) biopsy forceps. Inspection of all calices, including lower kidney pole, belongs to the state of the art of every fURS procedure performed in our department. Ureteral stent reinsertion was dependent on the complexity level of the given operation and the extent of postoperative ureteral trauma; thus, it was not performed routinely.
Postoperatively, the devices were cleaned, tested for leakproofness, disinfected with 30 mL of 1% GIGASEPT PAA (Schülke & Mayr GmbH), dried, and prepared for transport for external sterilization. The fURS devices that were deemed defective during routine postoperative processing were sent to external repair (Drägerwerk AG & Co. KGaA) and exchanged for new devices by the manufacturer.
Stone-free status was usually determined intraoperatively by the surgeon. Radiological reevaluation with CT or kidney, ureter, and bladder radiograph (KUB) was conducted only in cases of uncertainty regarding postoperative stone-free status or before second-look procedures.
The IPA was retrospectively digitally measured (Agfa HealthCare IMPAX Software) in accordance with the El-Bahnasy definition. 15 The angle was measured between the ureteropelvic axis and central axis of the lower pole infundibulum based on recorded intraoperative RPG images (Fig. 1).
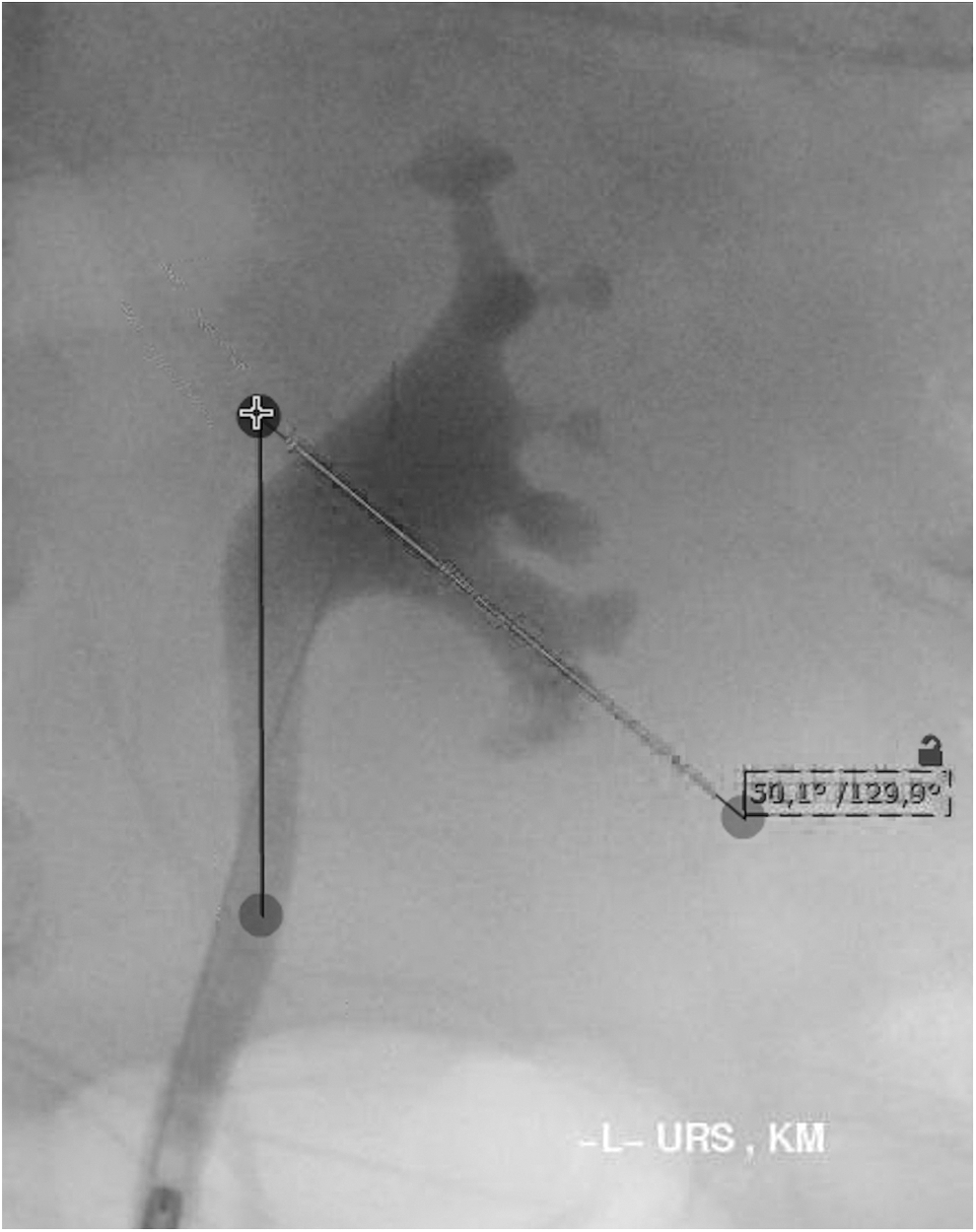
Infundibulopelvic angle of 50 degrees. URS = ureterorenoscopy.
Analyzed parameters included SFR, fURS device defects, intraoperative and postoperative complications, LOS, operation and fluoroscopy time, recurrent stone former status, and presence of lower pole kidney stones.
Recurrent stone former was defined as a patient with at least one stone event in the past. The fURS devices were deemed defective during routine postoperative processing. Intraoperative and postoperative complications were classified based on the Clavien-Dindo scale. 16 Routine hospital stay in our department is dependent on current reimbursement system and limited to 48 postoperative hours.
Statistical analysis was performed by RStudio (version 1.0.136). Mean value with standard deviation for normally distributed variables, median value with minimum and maximum values for variables without normal distribution, as well as percent values for categorical variables were used for descriptive statistics. Normal distribution was tested with the Shapiro–Wilk test. Depending on its results, the unpaired t-test or Mann–Whitney U, or Pearson correlation test was applied for univariate analysis. The level of significance was defined as p < 0.05.
Results
In total, 381 fURS performed between September 2013 and March 2017 were analyzed: 260 (68.24%) for kidney stone operation and 121 (31.76%) for diagnostic purposes. Preoperative characteristics are presented in Table 1. The majority of therapeutic fURS involved lower pole stones (194/260, 74.62%) and stones <2 cm (254/260, 97.69%). In 38 (9.97%) cases, devices were postoperatively deemed defective. Presence of lower pole kidney stones was observed in 23 out of 38 fURS (60.53%) cases with device damage.
Percentages and SDs for mean values in brackets.
fURS = flexible ureterorenoscopy; SD = standard deviation.
Device leakage (23/38, 60.53%) and defects of Bowden cable system (7/38, 18.42%) were two major recorded causes of device defect.
Median IPA in the analyzed cohort was 54.0 degrees. Extended postoperative hospital stay (>2 days) was noted in 56 (14.93%) cases. Detailed intraoperative and postoperative characteristics are presented in Table 2.
Percentages, SDs for mean values and minimum/maximum for median values in brackets.
Six cases excluded—consecutive procedure (e.g., nephrectomy) during the same hospital stay.
IPA = infundibulopelvic angle; RPG = retrograde pyelography; SFR = stone-free rate.
Significant complications requiring at least an additional pharmacological treatment (Clavien-Dindo ≥2) occurred in 39 (10.24%) patients. The majority of recorded complications (Table 3) were associated with postoperative urinary tract infection (27/39 cases, 69.23%), requiring antibiotic therapy (Clavien-Dindo grade 2). In one case, Double-J stent reinsertion (Clavien-Dindo grade 3b), and in two cases, intensive therapy (Clavien-Dindo grade 4) were necessary because of postoperative sepsis. Mortality was limited to one case of postoperative pneumonia.
In univariate analysis, significantly steeper IPA values correlated with damaged fURS devices (median 42.5 degrees vs 56.0, p < 0.001). A steep IPA was also significantly associated with the occurrence of Clavien-Dindo ≥2 complications (median 51.0 degrees vs 55.0, p = 0.005), as well as a prolonged hospital stay (median 51.0 degrees vs 55.0, p = 0.014). Figure 2 presents in detail boxplots of these significant parameters. No influence on SFR or operation time was observed (p > 0.05, Table 4).
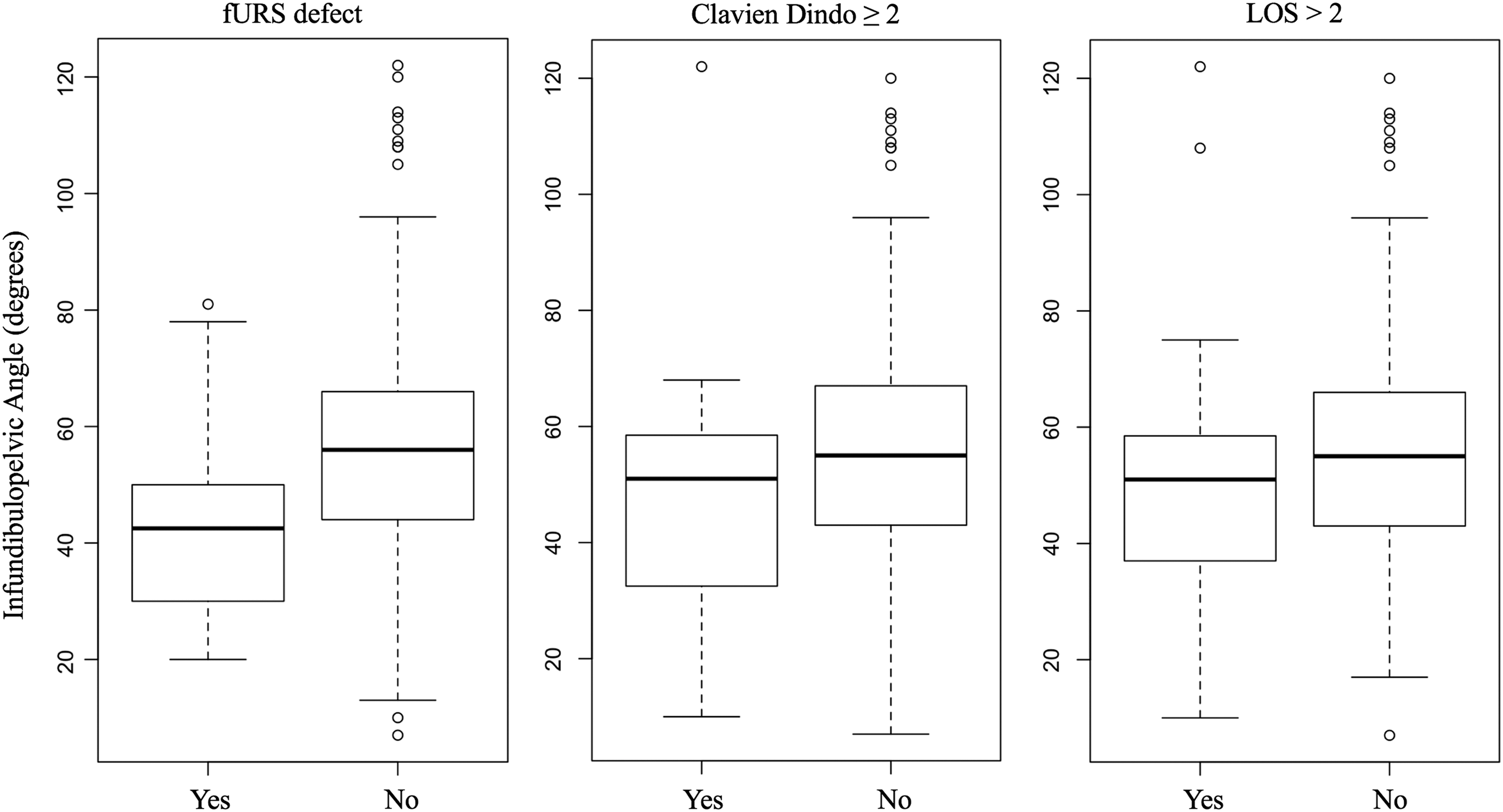
Box plots of statistically significant parameters (p < 0.05). fURS = flexible ureterorenoscopy; LOS = length of hospital stay.
Minimal and maximal values in brackets. Italic values characterize statistically significant parameters.
Mean value.
LOS = length of hospital stay; MWU = Mann–Whitney U test.
The linear model did not reveal any significant correlation between IPA and operating time (Pearson's r = 0.036, p = 0.486), or between IPA and fluoroscopy time (Pearson's r = 0.022, p = 0.672).
Discussion
To our knowledge, we present the first analysis of data revealing significant relationships between the anatomy of the collecting renal system and the damage rate of reusable fURS devices.
Our results suggest that a steep IPA, regardless of the complexity of the stone retrieval, influences the durability of reusable devices. Moreover, we noticed that relatively many defects occurred in diagnostic procedures (9/121; 7.44%). Therefore, it is possible that the IPA plays a role in device damage not only in typical cases with lower pole kidney stones. This hypothesis should be confirmed in further studies.
The vast majority of fURS defects occurred when the measured IPA reached 60 degrees or less (33/38 cases, 86.84%). One out of four cases with an IPA ≤35 degrees resulted in a postoperative flexible device defect (17/61, 27.87%). Based on these results, the IPA may be implemented in routine clinical practice for the identification of appropriate surgical measures to preserve reusable fURS devices by using costly single-use fURS devices instead.
A steep IPA was additionally associated with a prolonged hospital stay and the prevalence of intraoperative and postoperative complications (Clavien-Dindo ≥2). Thus, this group of patients demands not only careful performance by the surgeon but also additional attention during the postoperative period.
The cost-effectiveness with regard to fURS may be improved through some advancements in surgical techniques and resident training, to increase the longevity of already established reusable instruments. 17,18 On the other hand, already mentioned disposable fURS devices have been recently introduced as an alternative to traditional reusable flexible ureteroscopes. 19 –21 Among the different devices, the LithoVue™ (Boston Scientific) has the highest level of clinical evidence of clinical utility. 22
In terms of efficacy and safety, the LithoVue has been shown to not be inferior in comparison to reusable devices based on prospective trials. 23 –25 However, recently published cost analyses demonstrated higher costs in the routine use of single-use fURS devices over reusable flexible ureteroscopes for high-volume stone therapy centers. 9,26
Current data regarding risk factors for fURS device damage are scarce. The available literature focuses mostly on economic aspects of the usage of reusable flexible ureteroscopes, usually in comparison to single-use devices. 9,26,27
Martin et al. 26 prospectively summarized the annual costs of 160 reusable fURS procedures, including repair costs. Eleven cases with proven reusable fURS device damage were recognized in the same period. Based on this study, reusable fURS was determined to be a more cost-effective alternative for high-volume endourologic centers in the United States compared to disposable fURS, such as LithoVue. The average cost of reusable fURS revealed amortized costs of ∼$850 per use. However, the authors did not propose any specific risk factor of fURS device damage in their study. 26
Our working group also showed an economic superiority of reusable fURS in a retrospective cost simulation of an fURS program in a German setting. 9 The average cost of reusable fURS was ∼€500 per procedure. Moreover, it was observed that the fURS defects occurred usually in complex cases of kidney stone disease characterized by multiple, large dense stones, located particularly in the lower kidney pole that required laser disintegration with the necessary application of a laser fiber through the fURS working channel.
Based on the results of this study, we assume that not only preoperative stone status but also the anatomy of the renal collecting system, especially IPA, may be an important factor, which should be considered in future prospective trials that are designed to identify risk factors of reusable device damage and indications for disposable fURS.
Our Olympus devices are being used since 2016 and constitute minority of our equipment (3 Olympus URF-V vs 7 Karl Storz Flex-X2). Unfortunately, we possess the information regarding ureteroscope type only for the cases with reported device damage. To sum up, gathered data are not sufficient to determine which device type provides better performance and durability.
The absence of influence of overall IPA on the operation time and on the SFR based on intraoperative evaluation corresponds with the already published data of Jessen et al. 11
This supports the conclusion that modern fURS devices provide good performance regardless of the renal anatomy. It seems that the excellent flexion of modern flexible ureteroscopes guarantees good performance regardless of the stone position. Taking our study into consideration, it should be recommended that different endourologic tools as baskets, laser fibers, and biopsy forceps should be introduced only when the tip of flexible ureteroscope is straight positioned. Based on our experience, which stands in line with described results, the direct insertion of mentioned tools in deflected tip of ureteroscope to directly reach lower calix may result in ureteroscope leakage.
As already mentioned, stone-free status was determined intraoperatively by the surgeon. A more objective evaluation could be achieved by postoperative CT or KUB. Clinical practice in our department, however, supports the reduction of radiologic exposure to the patients in cases where intraoperative stone freedom is not questionable.
The IPA was measured retrospectively on RPG images taken intraoperatively. Contrast was usually applied through a semirigid URS device. The force generated by the insertion of a semirigid URS could cause ureter dislocation, thereby influencing measured IPA values.
The retrospective nature of our study is considered a limitation. Thus, the history of each reusable device was not tracked; we were unable to determine if the number of previous procedures or the type of ureteroscope had an impact on the risk of damage. Further case–control and prospective studies focused on finding other intraoperative and postoperative risk factors of flexible ureteroscope damage are needed. Assessment of other known radiological parameters regarding renal collecting system (e.g., infundibular length and width) was not possible because of retrospective character of the study. The accurate measurement of these parameters requires a defined distance between the patient's kidney and X-ray source. In retrospective setting, it was impossible to reproduce this value. Similar prospective analysis of overmentioned anatomical factors would be surely interesting for the future.
Conclusions
A steep IPA can be considered the first risk factor predicting both reusable fURS device damage and a complicated postoperative course. Special intraoperative and postoperative attention in cases with a steep IPA of 60 degrees or less are advised. A better understanding of damage mechanisms is key for the proper indication to use costly single-use devices. The significance of IPA as a risk factor has to be validated in prospective trials.
Acknowledgments
The authors express their gratitude to the coworkers from the University Hospital Schleswig-Holstein in Luebeck, spe- specifically Petra Schwarz and Lothar Lasarzewski, for providing technical data and expertise regarding the processing of fURS devices, and to Stefan Pilz for their help in study group selection.
Footnotes
Author Disclosure Statement
No competing financial interests exist.