
Abstract
Objectives:
To compare the outcomes of retroperitoneal vs transperitoneal approach for robot-assisted partial nephrectomy (RAPN).
Materials and Methods:
A systematic review of the literature was performed through January 2018 using PubMed, Scopus, and Ovid databases. Article selection proceeded according to the search strategy based on PRISMA criteria. Only studies comparing retroperitoneal to transperitoneal approach for RAPN were deemed eligible for inclusion.
Results:
Seven retrospective case–control studies were identified and included in the analysis, with a total number of 1379 patients (866 for transperitoneal group; 513 for retroperitoneal group). In the retroperitoneal group, tumors were slightly larger [weighted mean difference (WMD): 0.29 cm; 95% confidence interval (CI): 0.04–0.54; p = 0.02], and more frequently located posterior/lateral (odds ratio: 0.61; 95% CI: 0.41–0.90; p = 0.01). In two of the studies only posterior tumors had been included. Both operating time (WMD 20.17 min; 95% CI 6.46–33.88; p = 0.004) and estimated blood loss (WMD 54.57 mL; 95% CI 6.73–102.4; p = 0.03) were significantly lower in the retroperitoneal group. In addition, length of stay was significantly shorter in the retroperitoneal group (WMD 0.46 days; CI 95% 0.15–0.76; p = 0.003). No differences were found regarding overall (p = 0.67) and major (p = 0.82) postoperative complications, warm ischemia time (p = 0.96), and positive surgical margins (p = 0.95).
Conclusions:
Retroperitoneal RAPN can offer in select patients similar outcomes to those of the most common transperitoneal RAPN. Furthermore, it may be particularly advantageous for posterior upper pole and perihilar tumors and associated with reduction in operative time and hospital stay. Robotic surgeons should be ideally familiar with both approaches to adapt their surgical strategy to confront renal neoplasms from a position of technical advantage and ultimately optimize outcomes.
Introduction
P
Both transperitoneal 7,8 and retroperitoneal 9 approaches have been described and standardized for robot-assisted PN (RAPN). Debate is ongoing to define their role, as advantages and disadvantages of each of these two approaches are being scrutinized. Only a limited number of comparative studies have been reported, and therefore, a gap exists in the literature. 10
Aim of this study is to provide the most up to date systematic review and cumulative analysis of reported comparative outcomes of retroperitoneal RAPN (R-RAPN) vs transperitoneal RAPN (T-RAPN).
Material and Methods
Search strategies
A systematic revision of literature was performed up to January 2018 using different search engines (Pubmed, Ovid, and Scopus) to identify studies comparing R-RAPN to T-RAPN. A review protocol was established before conducting the study. The PICO model was as follows: population consisted of patients with renal mass (P) who underwent RAPN with retroperitoneal approach (I) or standard transperitoneal approach (C). Outcomes of interest were perioperative outcomes (O), as detailed later. Identification and selection of the studies were conducted according to Preferred Reporting Items for Systematic Reviews and Meta-analysis criteria (

PRISMA flow for study selection and inclusion.
Selection criteria
Two of the authors (N.P. and R.A.) performed the article selection, which was limited to English language only and with adult patients. Only original studies comparing the outcomes of retroperitoneal and T-RAPN for renal tumors were included. Title and abstracts were first reviewed to ascertain whether they would potentially follow the inclusion criteria. For those passing the first screening, a full text analysis was performed to confirm inclusion. Studies without primary data (letters to the editor/authors, case reports, and commentaries), as well as conference abstracts, were not considered. References of collected studies were manually reviewed to find additional studies of interest.
Assessment of study quality and publication bias
We classified each study according to the level of evidence (
Data extraction and analysis
Data were extracted from each selected study consisting of baseline demographics [age, gender, body mass index (BMI), preoperative estimated glomerular filtration rate (eGFR), tumor size, RENAL nephrometry score, 11 side, and location], intraoperative data [(operative time (OT), estimated blood loss (EBL), and warm ischemia time (WIT)], and postoperative outcomes [complications (minor and major, according to Clavien-Dindo 12 ), hospital stay, and positive surgical margin (PSM) rate].
For continuous outcomes, the weighted mean difference (WMD) was used as a summary measure, whereas the odds ratio (OR) or risk ratio (RR) with 95% confidence interval (CI) was calculated for binary variables. RR was preferred in cases of a high number of events to avoid overestimation. As only means and standard deviations are permitted for the computational portion of meta-analyses, a validated mathematical model was used to convert median (range) to mean (standard deviation) for studies reporting medians and ranges.
13
Pooled estimates were calculated using the random-effect model to account for study heterogeneity. Evaluation of potential publication bias was done by funnel plot analysis for each outcome. All statistical analyses were performed using Review manager 5 (Cochrane Collaboration, Oxford, United Kingdom). The study was prospectively registered and approved by the PROSPERO website (
Results
Description of included studies and quality assessment
Seven studies were identified and included for the analysis 14 –20 (Table 1), which were published between 2013 and 2018. None of them was a randomized clinical trial. Three studies were observational retrospective case–control studies, three of them were retrospective matched cohort studies, and one was a prospective nonrandomized study. Study quality was high for all studies. Due to small number of studies, visual assessment was unlikely to be accurate, but no obvious publication bias was observed.
Level of evidence for all studies: IIIb (according to Oxford Centre for Evidence-based Medicine).
According to Newcastle–Ottawa scale
R-RAPN = Retroperitoneal RAPN; T-RAPN = Transperitoneal RAPN.
Demographics and clinical characteristics
Among the 1379 patients included in the meta-analysis, 866 (62.8%) were T-RAPN and 513 (37.2%) R-RAPN. Table 2 summarizes patient and tumor characteristics. There was no difference between groups in terms of gender (p = 0.50), age (p = 0.40), BMI (p = 0.09), RENAL score (p = 0.74), and tumor side (p = 0.97). In the R-RAPN group, tumors were slightly larger (WMD 0.29 cm; p = 0.02) and more frequently posterior/lateral (RR 0.61; p = 0.01). To note, in two studies only posterior tumors were considered. 16,17 The baseline eGFR was lower in R-RAPN group (WMD −3.63 mL/min; p < 0.001).
BMI = body mass index; CI = confidence interval; eGFR = estimated glomerular filtration rate.
Surgical outcomes
Forest plots for main intraoperative outcomes are illustrated in Figure 2. Both OT (WMD 20.17 min; 95% CI 6.46–33.88; p = 0.004) and EBL (WMD 54.57 mL; 95% CI 6.73–102.4; p = 0.03) were significantly lower in the R-RAPN group, whereas no significant differences were found in terms of WIT (WMD −0.04 min; 95% CI −1.76–1.68; p = 0.96).
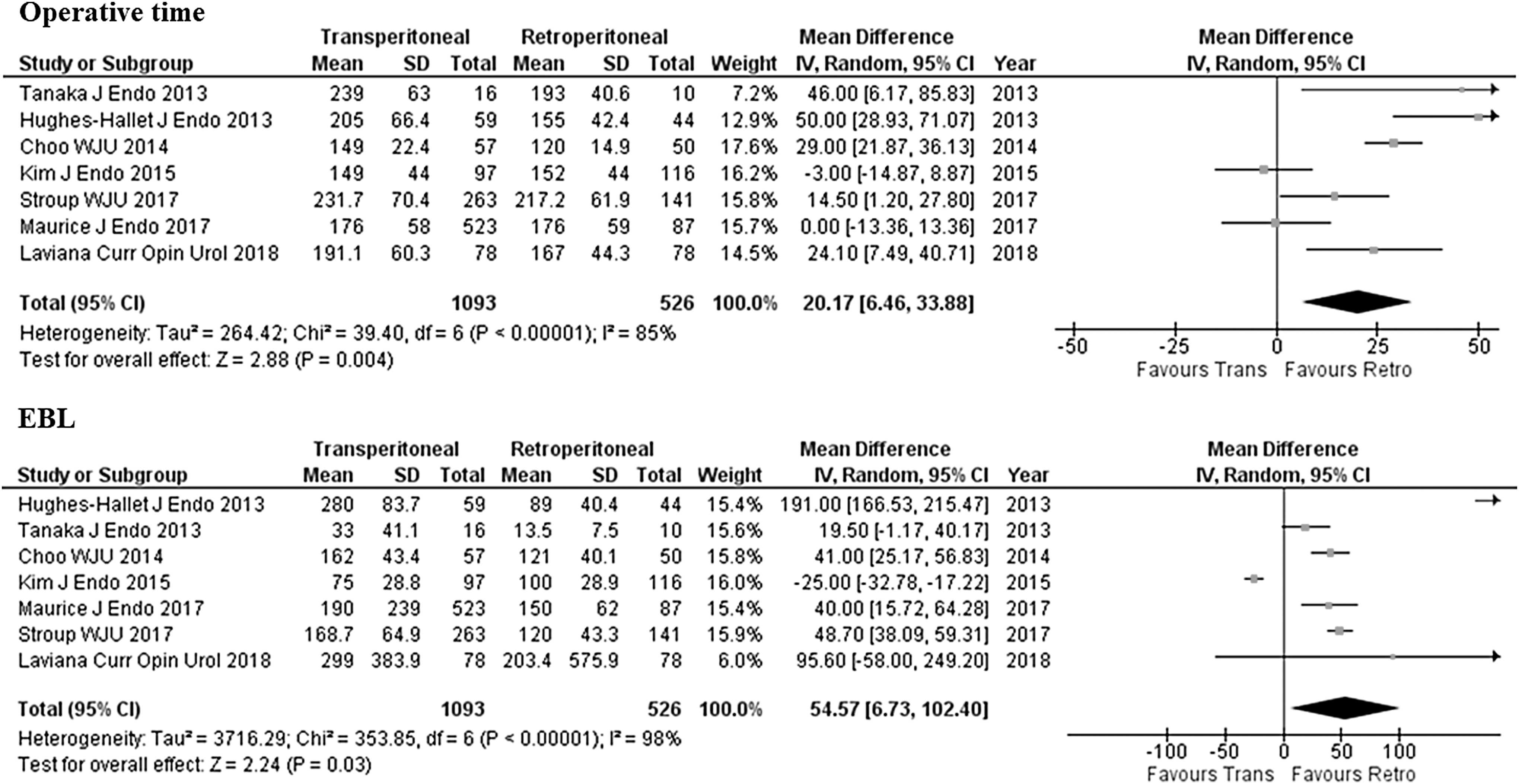
Forest plots for operative time and estimated blood loss.
Overall complication rate was 12.8% and 13.3% for T-RAPN and R-RAPN, respectively, and no difference was found between groups (OR 1.08; 95% CI 0.77–1.52; p = 0.67). Major complication rates were 2.7% and 3.4% for T-RAPN and R-RAPN, respectively, and similarly no difference was found between groups (OR 0.94; 95% CI 0.52–1.69; p = 0.82). PSM rates were 2.2% and 2.9% for the T-RAPN and R-RAPN, respectively (OR 0.98; 95% CI 0.47–2.06; p = 0.95). Finally, the hospital stay was significantly shorter in the R-RAPN group (WMD 0.46 days; CI 95% 0.15–0.76; p = 0.003) (Fig. 3).
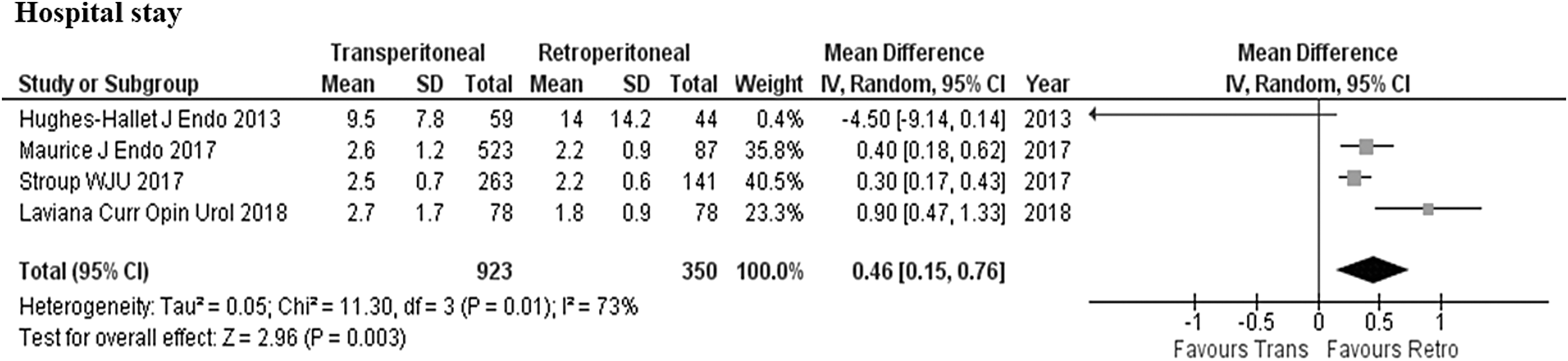
Forest plots for hospital stay.
Discussion
Herein we present the largest cumulative analysis to date of studies comparing the retroperitoneal vs transperitoneal approach for RAPN. Overall, our findings suggest that both approaches may offer equivalent and optimal surgical quality and short-term oncologic and functional outcomes for both anterior and posterior masses. Not surprisingly, the retroperitoneal approach is preferred for posteriorly located tumors, and it might offer an advantage in terms of shorter OT, lower EBL, and shorter hospital stay. The clinical impact of these differences, however, seems to be negligible with respect to functional recovery and oncologic efficacy, and it remains to be determined with respect to quality of life indices.
In the only other similar analysis, reported by Xia et al., only 4 studies were included for a total of 449 patients, and no significant difference was found in any of the only outcome of interest, except for a marginally shorter OT for the R-RAPN group (WMD: 28.03; 95% CI 0.41–55.65; p = 0.05). 10 This difference has become statistically more significant in our analysis (WMD 20.17 min; 95% CI 6.46–33.88; p = 0.004), likely due to the larger sample. The shorter OT was reported in four of the studies included in our analysis. 14 –16,19,20 Intuitively, Hughes-Hallet et al. explained this result by considering that a retroperitoneal approach allows to access the renal hilum without colon mobilization. 14 In this regard, it should be acknowledged how patient selection impacts cumulative findings. Most surgeons preferring a transperitoneal approach would still use this approach for posterior tumor and spend more time doing so. In that regard, they could consider a retroperitoneal approach. In contrast, approaching some tumors, such as large (clinical T2+) or highly complex tumors, or lower pole tumors, using a retroperitoneal approach might be more challenging.
Another significant difference found in our analysis was the lower EBL for the R-RAPN group, which, however, despite reaching the statistical significance (p = 0.03) might not be clinically significant (about 55 mL). A reduction in EBL in the retroperitoneal group was also reported in a previous comparative study, including laparoscopic and robotic PN cases reported by Gin et al. 21 Hughes-Hallet et al. reported a significantly lower EBL in the R-RAPN group compared to the T-RAPN group (88 vs 395 mL, p < 0.01), and the authors explained this difference by the larger use of an early unclamping technique in the T-RAPN and also by the reduced surgical dissection needed in the retroperitoneal access. 14
Regarding other relevant intraoperative outcomes, it is worth mentioning that no difference was found for the WIT between the two approaches. In all the studies, mean WIT for both groups were under the 25–30 min cutoff, which has been traditionally considered as a benchmark to reach for functional preservation. 22,23 This might be explained by the fact that Centers and surgeons reporting these studies had become proficient with both RAPN techniques.
Our cumulative analysis confirmed an overall shorter hospital stay for the R-RAPN group of about half day (WMD 0.46 days; CI 95% 0.15–0.76; p = 0.003). According to Maurice et al., a faster recovery of bowel function represents a potential advantage of R-RAPN, which can translate into an earlier discharge and, therefore, shorter hospital stay. This group reported a mean of 2.2 days in the R-RAPN group vs 2.6 days in the T-RAPN group (p = 0.01). 18 A significant reduction in the hospitalization time was also recorded by Hughes-Hallet et al. (4.6 days for the T-RAPN vs 2.5 days for the R-RAPN group; p < 0.01). 14 Moreover, Kim et al. reported transperitoneal approach for RAPN to be a significant predictor of hospital stay greater than 1 day (OR = 7.4, p < 0.01) on a multivariate analysis when controlling for age, sex, BMI, patient comorbidity, previous abdominal surgery, baseline kidney function, nephrometry score, and tumor size. 17 More recently, Laviana et al. found R-RAPN to be associated with a 76% lower probability of hospital stay of at least 2 days (p < 0.001). 20 These authors also performed a cost analysis and found that the shorter hospital stay and OT were the main driving costs, which resulted in an overall reduced cost for the R-RAPN group (−2337 USD). Of course, these findings might not be generalizable to other hospital settings. Moreover, one can argue that postoperative hospital stay is not only depending on the surgical technique, and it can be influenced by factors other than preoperative parameters. In this regard, it has been shown that outpatient transperitoneal laparoscopic nephrectomy can be safely implemented in well informed and selected patient, given appropriate hospital setup. 24
In the field of laparoscopic kidney surgery, Fan et al. reported a meta-analysis, including six studies, comparing transperitoneal vs retroperitoneoscopic PN and found shorter OT (WMD: 48.85 min; p < 0.001) and shorter length of stay (WMD 1.01 days; p = 0.001) for the retroperitoneoscopic group. 25 Therefore, similar differences in the case of standard laparoscopy were detected for these two parameters and even at larger extent than for robot-assisted laparoscopy. It might be speculated that the use of a robotic platform might attenuate these differences by facilitating surgeons to become proficient in both transperitoneal and retroperitoneal approach. Certainly, the adoption of robotic technology for minimally invasive PN seems to offer better outcomes, 5,26 likely allowing a larger adoption of nephron-sparing surgery. 6
The positive margin rate for both groups/approaches in our analysis was below 3%, which is a desirable figure, in line with literature from high volume institutions for PN. 27,28 As the oncologic significance of this surrogate oncologic parameter remains to be defined, surgeons should thrive to leave “no tumor behind”. 27
Some limitations of our study need to be acknowledged. The major limitation is related to the design of included studies. Despite representing a robust statistical tool, meta-analyses certainly carry intrinsic biases, and randomized controlled trials should ideally be included. In our analysis, most of the studies were either retrospective or prospective nonrandomized, however of good quality. Moreover, our cumulative analysis was necessarily limited to certain parameters that were extractable and available. For example, it was not possible to perform any functional outcome analysis. 29 Moreover, more robust oncologic outcomes, other than the PSM rate, were also not available for analysis. To note, it was not possible to account for existing differences among institutions and surgeons in terms of surgical technique and expertise, as well as protocols of perioperative management and follow-up. Furthermore, it would be interesting to assess how the introduction of the Xi system might facilitate a retroperitoneal approach on larger or lower pole masses, due to less clashing compared to Si system. Despite these limitations, we can provide the best available evidence in the field, and therefore, our findings can be used as reference for further clinical investigation. In the future, further comparative prospective ideally randomized multicenter studies are needed to better clarify the role of one vs the other access for RAPN.
Conclusions
Notwithstanding the intrinsic limitations of this type of cumulative analysis, our findings show that R-RAPN offers similar outcomes to those of the T-RAPN in select patients. Furthermore, it may be particularly advantageous for posterior upper pole and perihilar tumors, and it might translate into shorter OT and hospital stay. While further clinical investigation is warranted to confirm these findings and ultimately provide a higher level of evidence, it is likely that T-RAPN will remain the preferred approach in the hands of many. However, robotic surgeons should be ideally familiar with both approaches to adapt their surgical strategy to confront renal neoplasms from a position of technical advantage and ultimately optimize outcomes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.