
Abstract
Objective:
To present our technique and initial results of dual combined retroperitoneal and transperitoneal laparoscopic approach for the treatment of renal-cell carcinoma (RCC) with level 0–II venous tumor thrombus.
Patients and Methods:
We included nine consecutive patients with RCC and level 0–II inferior vena cava (IVC) thrombus who underwent laparoscopic radical nephrectomy and IVC thrombectomy using dual combined laparoscopic approach in our department between January 2016 and June 2017.
Results:
The mean operative time was 150 minutes when cavotomy was not performed and 240 minutes when cavotomy with thrombectomy was required. The mean IVC clamping time was 24 minutes and the mean blood loss was 300 mL. We encountered no major intraoperative or postoperative complications (Clavien III–IV). The patients were discharged a mean of 7 days after the procedure. At the 6-month follow-up, all patients were alive. One patient presented a retroperitoneal enlarged lymph node and started systemic treatment.
Conclusions:
The dual combined laparoscopic approach for kidney tumors with level 0–II IVC thrombus is feasible, reproducible, and especially useful in patients with complex renal pedicle. The technique provides early arterial control by retroperitoneal approach, which reduces the blood flow through the renal vein and has the advantage of minimal mobilization of the thrombus-bearing renal vein; it therefore lowers the risk of tumor embolism and intraoperative hemorrhage.
Introduction
A
The open approach has previously been considered the standard when performing radical nephrectomy with IVC thrombectomy. More recently, the focus has shifted toward the minimally invasive techniques (laparoscopy and robotics), which have proven their feasibility for performing high complexity surgeries. 5 The current challenge for the surgical treatment of RCC with IVC thrombus is to ensure maximal oncologic control, with minimal morbidity for the patient.
The preferred approach for minimally invasive techniques is transperitoneal, but some authors have described as feasible a full retroperitoneal laparoscopic approach for level II tumor thrombus. 6 The transperitoneal approach offers a larger working space, but it is hampered by an increased mobilization of the thrombus-bearing renal vein, which may increase embolism risk. On the contrary, the retroperitoneal approach is of interest because it ensures a fast and direct access to the renal artery before kidney mobilization, and also an easier access to the lumbar veins, 7 but the smaller working space, the limited access to an extended lymph node dissection, and longer learning curve limit its use. 8
The aim of the current report is to present our technique and initial results of the dual combined retroperitoneal and transperitoneal laparoscopic approach for the treatment of RCC with level 0–II venous tumor thrombus.
Patients and Methods
Patient selection
We included nine consecutive patients with RCC and level 0–II thrombus who underwent laparoscopic radical nephrectomy and IVC thrombectomy using the dual combined laparoscopic approach in our department between January 2016 and June 2017. The study was approved by the local hospital ethics committee and all patients signed the written informed consent. All procedures were performed by the same surgeon.
Complete laboratory serum evaluation was performed in all patients, including full blood count, kidney and liver function, and electrolyte tests.
The preoperative imaging assessment included thoracoabdominal contrast-enhanced CT, abdominal contrast-enhanced MRI, and echocardiography.
We staged the patients according to the 2010 TNM criteria of the American Joint Committee on Cancer. 9
The anticoagulation therapy used in these patients was 1 mg/kg enoxaparin subcutaneously twice a day, from the moment of diagnosis and paused 12 hours before surgery. Twelve hours after the procedure, the anticoagulation therapy was resumed and continued up to 21 days.
Surgical technique
We describe the technique used for right-sided tumors. The patient was positioned in 90° left lateral decubitus position, with the surgical table flexed. The retroperitoneal space was developed by finger and balloon dissection and four trocars were placed in the right lumbar area, according to the method developed in our department 10 (Fig. 1).
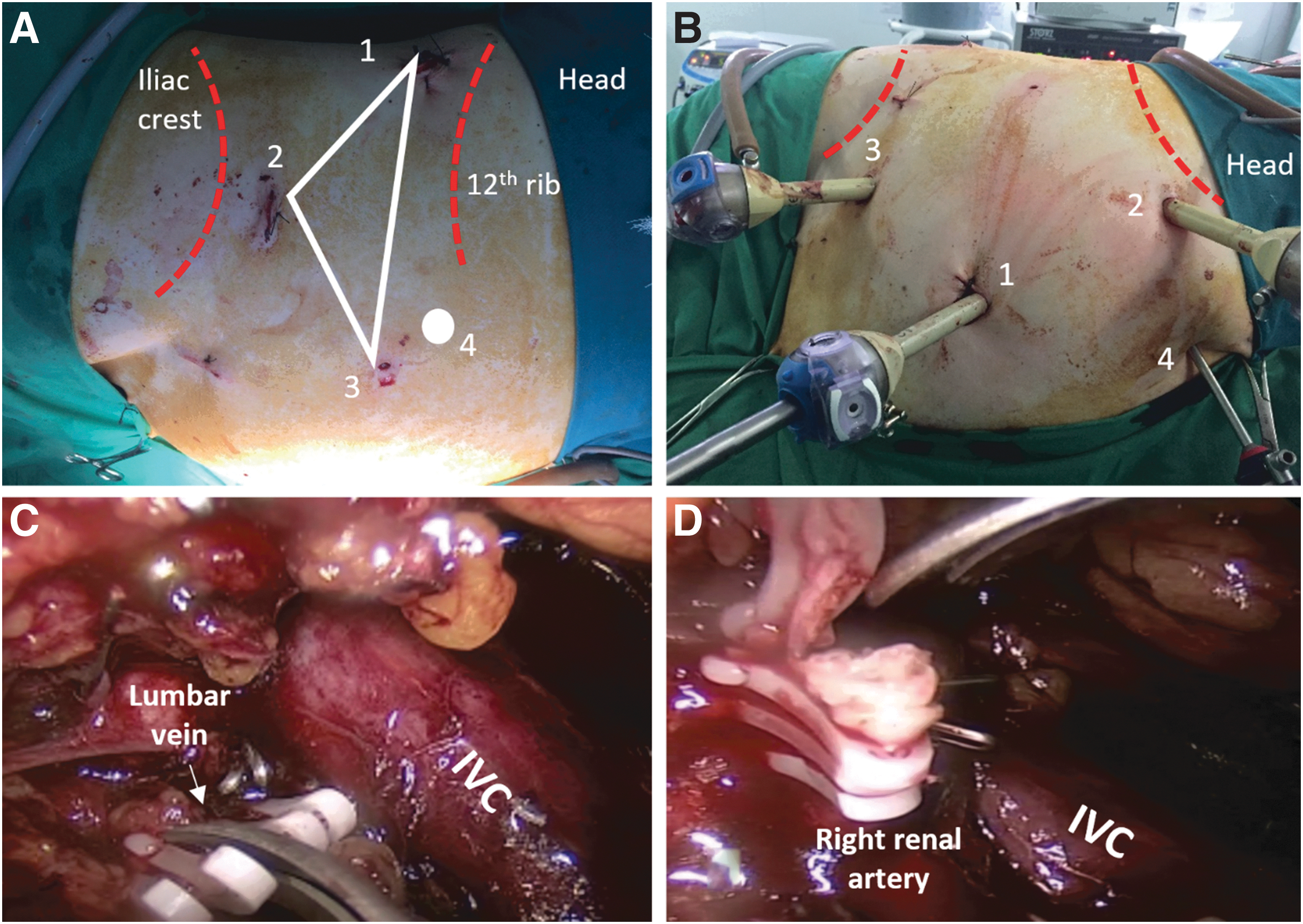
The renal artery was identified and dissected after medial incision of Gerota's fascia. The clipping of the renal artery (arteries) was performed using L size Hem-o-lok clips and the vessel was sectioned. We continued with the mobilization of IVC cranially and caudally to the renal hilum. All identified lumbar veins were clipped and divided.
After the renal artery (ies) was clipped and mobilization of IVC was completed, surgery continued in the transperitoneal approach, with the placement of four trocars in the abdomen. Only one 5 mm port site from the retroperitoneum for the assistant was left open until the end of the surgery in case another trocar was needed during transperitoneal approach. We began the dissection by incising the line of Toldt and reflecting the ascending colon and the duodenum medially. We identified the right ureter and right gonadal vein, and the latter was clipped and transected. The renal vein was identified and isolated, with minimal mobilization. The dissection continued cranially up to the hepatic veins. The adrenal vein was identified, clipped, and divided, and the adrenal gland was dissected on the medial side to isolate the infrahepatic IVC.
In case of level 0 thrombus, we performed the milking of the thrombus and clipped the renal vein with XL size Hem-o-lok clips immediately close to its junction with IVC. In two cases with level I thrombus, we observed a significant retraction of the tumor thrombus after ligation of the renal artery, which allowed us to milk it and safely ligate the renal vein with Hem-o-lok clips, without the need of cavotomy.
In the rest of the cases with IVC level I–II thrombus, we continued with the skeletonization of IVC also on the medial side, with subsequent identification and isolation of the left renal vein. We encircled with vessel loops the left renal vein, the IVC caudally to the renal hilum, and the IVC cranially to the renal hilum, above the thrombus, but below the hepatic veins (Fig. 2). We performed the occlusion of the veins using Rummel tourniquets in the following order: IVC below the renal hilum, left renal vein, and IVC above renal hilum. We performed the incision of the IVC with complete removal of tumor thrombus. The IVC was closed after heparinization using double-layered Prolene 5/0 continuous suture and the blood flow was restored by releasing the tourniquets in reverse order. The suture line was inspected for leakage (Fig. 3). The kidney was placed into the endobag as soon as cavorraphy was performed. The extraction of the kidney was performed through an incision in the right inguinal region. Two drains were placed: near the IVC suture line and Douglas space.


For the left side, we used a similar approach, but the dissection was performed at the lateral border of the aorta. After clamping the left renal artery, the tumor thrombus retracted and was safely milked in a retrograde manner, so there was no need to dissect the renal vein closer to its junction with IVC.
Results
The baseline characteristics of the patients are summarized in Table 1. Three patients had mild anemia and impaired liver function, both being considered paraneoplastic.
According to the 2010 TNM criteria of the American Joint Committee on Cancer.
IQR = interquartile range; n = number of patients.
All the patients with left kidney tumor had level 0 thrombus, as well as one patient with right-sided tumor. None of the patients showed evidence of distant metastasis. The contralateral kidney was normal in all cases.
Table 2 displays operative and perioperative data. Adrenalectomy was performed in three cases of suspicion of tumor invasion on the preoperative imaging assessment, which was not confirmed by the pathologic analysis. Hilar lymph nodes were removed and were negative in all patients, whereas interaortocaval lymphadenectomy was not performed.
IVC = inferior vena cava.
The patients started mobilization on postoperative day 2 and were discharged a mean of 7 (5–9) days after the procedure. None of the patients experienced significant complications (Clavien–Dindo 11 III–V). We encountered seven minor postoperative complications in six patients: one patient received transfusion, two patients developed port-site hematoma, and three patients presented postoperative elevated estimated glomerular filtration rate (eGFR), of whom one was discharged with a creatinine of 2 mg/dL. One patient with port-site hematoma also presented prolonged lymphatic drainage up to 6 days.
The pathologic examination identified negative surgical margins in all cases (Table 3). From the three cT4 patients, one was downstaged to pT3b and two to pT3a after pathologic analysis of the adrenal gland.
RCC = renal-cell carcinoma.
At the 6-month follow-up, all patients were alive. One of the pT3b patients presented a retroperitoneal enlarged lymph node and started targeted systemic treatment with sunitinib, the other eight having no evidence of recurrence at this point.
Discussion
The most important principles of minimally invasive radical nephrectomy with IVC thrombectomy are 12 early arterial control as well as control of the lumbar veins to reduce hemorrhagic complications during vessel loop placement and cavotomy, minimal IVC mobilization to reduce the risk of tumor embolism, occlusion of the major blood vessels in a specific order, immediate placement of the specimen into an endobag to reduce local seeding, and an experienced and dedicated surgical and anesthesiologic team.
Our dual technique combines the two approaches for laparoscopic nephrectomy. The retroperitoneal approach is preferred for faster identification and ligation of the renal artery and also for allowing the identification and sectioning of lumbar veins that drain into IVC in the proximity of the renal hilum. The early occlusion of renal artery leads to decreased blood flow through the renal vein, decreased intraoperative bleeding, retraction of the tumor thrombus, and a lower risk of tumor embolism. The transperitoneal approach offers improved access to the interaortocaval space (to perform extended lymphadenectomy), to the contralateral renal vein and intrahepatic IVC, and also a larger working space for performing cavotomy, excision of the thrombus, and suturing of IVC. The data hereby presented confirm the feasibility and safety of this dual combined laparoscopic approach.
The literature regarding the surgical treatment of RCC with venous thrombus is rather scarce: the majority of the published articles reported limited case series or clinical cases.
A similar combined laparoscopic approach was also described by Sanli et al. 13 (two cases), Tang et al. 14 (one case), and Shao et al. 15 (six cases), but with a few differences from our approach, which is described next.
Sanli and colleagues 13 placed three trocars for retroperitoneal and also for transperitoneal approach and liver retraction was performed using the retroperitoneal access ports. In both cases, the surgeon performed the milking of the thrombus with the Hem-o-lok clip applier and transected the renal vein after placing a Satinsky clamp, followed by suture—in the first case, or applied Hem-o-lok clips on the renal vein—for the second case. Shao and coworkers 15 described the occlusion of IVC and left renal vein with bulldog clamps in all six patients, with complete removal of the thrombus after incision of IVC.
In cases with renal vein thrombus and in two cases of level I IVC thrombus, we also performed the milking of the thrombus, but we used Rummel tourniquets to occlude IVC (distal and proximal to the renal vein) and the left renal vein to avoid thrombus migration during thrombectomy. We believe that the use of bulldog clamps for the occlusion of the vessels during IVC thrombectomy may be preferable to the tourniquets, as we experienced a slow retrograde bleeding up to the end of the IVC suturing.
The reported operative time when performing IVC thrombectomy ranged between 150 and 210 minutes, 13,15 the IVC clamping time was 16 minutes, 13 and mean blood loss ranged between 150 and 1100 mL, 15 similar to our figures.
None of the authors reported significant intraoperative or postoperative complications or conversions to open surgery, and the patients were discharged 4 to 9 days after the procedure, which was similar with our experience. 13 –15
The high complexity and morbidity of the procedure, especially in case of left-sided tumors, lead other surgeons to develop new techniques. Ghareeb and coworkers 16 reported a hand-assisted approach to milk the thrombus before the division of the left renal vein using a vascular stapler, thus proving the feasibility of a hybrid minimally invasive approach for left-sided tumors.
Furthermore, Liss and associates 17 showed the feasibility of laparoendoscopic single-site transperitoneal approach for such cases, with similar perioperative outcomes (operative time and blood loss) and significant advantages in terms of pain score at discharge, major analgesic requirement, and hospital stay in comparison with multiport laparoscopy, but this technique is still in its infancy.
Although currently the laparoscopic approach is considered feasible, in selected cases, for completely intracorporeal nephrectomy with IVC thrombectomy, the technique gained popularity only after the advent of robotic surgery. The advantages of the robotic systems facilitate the high-complexity surgical gestures. 18 Gill and colleagues 12 reported one of the largest experiences in robot-assisted level II–III IVC thrombectomy (24 patients) and concluded that the robotic approach can offer reproducible vascular, reconstructive, oncologic, and clinical outcomes. The authors report a mean operative time of 4.5 hours (range 3–8 hours), mean blood loss of 240 mL (100–7000 mL), and 16.7% rate of complications (Clavien–Dindo II–IIIb) during the first postoperative year.
An alternative to the use of the retroperitoneal approach for primary clamping of renal artery is preoperative renal embolization, but this technique has raised controversies as some authors reported an association of preoperative embolization with increased transfusion requirements, operative time, and postoperative complications and mortality rate. 19 On the contrary, Gill and colleagues 12 observed that preoperative embolization leads to decompression of venous collaterals and decreased blood loss. Nonetheless, according to oncologic surgery, the primary approach of the right renal artery should be in the interaortocaval space, as described by Ramirez and associates. 20 The retroperitoneal clamping of the renal artery or embolization represents alternatives to this technique to limit the mobilization of the thrombus-bearing renal vein or IVC. Still, one of the most important advantages of performing the dual approach is the possibility of identification, clamping, and sectioning of the lumbar veins, which is of utmost importance in reducing hemorrhagic incidents during IVC vessel loop placement and IVC thrombectomy.
A further question about the surgical management of RCC with venous thrombus is related to the moment of endobag insertion. We insert the kidney into the endobag after IVC suture and continue with full mobilization. At the end of this step, the kidney falls into the endobag entirely by itself. The fact that the kidney is fixed to the abdominal wall during cavotomy maintains the renal hilum elevated and avoids excessive mobilization of the renal vein. We consider that the risk of tumor spillage is minimal when this procedure is used. None of the included patients presented with local recurrence, although our follow-up is limited. Another possible technique is to clamp the IVC, staple the thrombus-bearing renal vein, and perform cavotomy and resection of the remaining thrombus as described by Gill and colleagues 12 Using the latter technique, the authors reported a 46% new-onset metastatic disease after surgery at a mean follow-up of 16 months, but they included patients with level III thrombus and higher percentage of Fuhrman grade III–IV tumors. Because the exact location of the recurrences was not detailed, a possible link with the surgical approach remained elusive.
Conclusions
In conclusion, we hereby present our technique of dual combined laparoscopic approach for kidney tumors with renal vein and IVC level I–II thrombus. We consider that this approach is feasible, reproducible, and especially useful in patients with complex renal pedicle. The technique provides early arterial control due to the retroperitoneal approach and offers advantages by minimizing the mobilization of the thrombus-bearing renal vein, reducing the blood flow through the renal vein and therefore the risk of tumor embolism and intraoperative hemorrhage.
Footnotes
Author Disclosure Statement
No competing financial interests exist.