
Abstract
Introduction:
A ball-tip holmium laser fiber (TracTip; Boston Scientific) has been developed to theoretically reduce damaging friction forces generated within a ureteroscope working channel. We compared the insertional forces and damage with a ureteroscope inner lining when inserting standard flat-tip and ball-tip laser fibers.
Materials and Methods:
A standard ureteroscope channel liner was placed in a 3D-printed plastic mold. Molds were created at four angles of deflection (30°, 45°, 90°, and 180°) with a 1 cm radius of curvature. New 200 μm ball-tip (TracTip; Boston Scientific) and 200 μm flat-tip (Flexiva; Boston Scientific) laser fibers were advanced through the liner using a stage controller. A strain gauge was used to measure force required for insertion. Each fiber was passed 600 times at each angle of deflection. The ureteroscope liner was changed every 150 passes. Leak testing was performed every 50 passes or when the insertional force increased significantly to assess damage to the liner.
Results:
At all deflection angles, the average insertional force was significantly lower with the ball-tip laser fibers compared with flat-tip laser fibers (p < 0.001). All trials with the ball-tip lasers were completed at each angle without any leaks. Two of four trials using flat-tip fibers at 45° deflection caused liner leaks (at 91 and 114 passes). At 90° deflection, all flat-tip trials caused liner leaks on first pass. The 180° trials could not physically be completed with the flat-tip laser fiber. Within the flat- and ball-tip groups, an increasing amount of force was needed to pass the fiber as the degree of deflection increased (p < 0.001).
Conclusions:
The ball-tip holmium laser fiber can be safely passed through a deflected ureteroscope without causing liner perforation. The standard flat-tip fiber requires greater insertion force at all angles and can cause the ureteroscope liner to leak if it is deflected 45° or more.
Introduction
T
Damage to the working channel has been documented during instrument introduction into a deflected ureteroscope. This damage can be due to friction from the instrument tip, as well as photothermal exposure from an activated laser. 9 To address working channel damage, ball-tip laser fibers such as the Flexiva TracTip (Boston Scientific, MA) were developed to reduce insertional forces, thereby reducing the likelihood of ureteroscope damage.
In this study, we compare the insertional forces and ureteroscope liner damage that occurs when a standard polished flat-tip or ball-tip laser fiber is introduced into a model mimicking ureteroscope deflection.
Materials and Methods
Two laser fibers were tested and compared: the 200 μm ball-tip (TracTip) laser fiber and the 200 μm polished flat-tip Flexiva fiber (Boston Scientific).
A ureteroscope working channel model was developed by placing a standard polytetrafluoroethylene (PTFE) ureteroscope working channel liner in a plastic mold created using a 3D printer. Molds were created at four different angles of deflection (30°, 45°, 90°, and 180°) using a radius of curvature of 1 cm, which is consistent with that of a flexible ureteroscope positioned within the upper, interpolar, and lower pole renal calices 10 –12 (Fig. 1).

In vitro experimental setup.
Unused ball-tip laser fibers and uncleaved, new polished flat-tip laser fibers were advanced through the models using a stage controller to maintain a constant velocity of 0.6 cm/second, which allowed for accurate force measurements and visual determination of effective fiber passage. Force generated from laser fiber insertion was measured using a strain gauge. Each fiber was passed 600 times through each deflection angle model with the liner exchanged every 150 passes to allow for four separate runs per fiber angle pair. Each individual angle was tested with a new laser fiber. No working channel liners or laser fibers were reused during the study period.
Leak testing was performed every 50 passes or when a significant increase in force was noticed to assess damage to the ureteroscope liner. An air-filled syringe was attached to both ends of the liner submerged in water. When passing air from one syringe to another, a leak was noted when air escaped from the lining wall. If a leak was noted, all remaining passes for that liner were aborted.
Statistical evaluation included calculation of means and 95% confidence intervals, which have been graphically represented. t-Tests were performed to compare flat-tip vs ball-tip insertion forces at each respective angle of deflection. One-way analysis of variance was used to compare multiple groups, and post hoc Tukey's Honest Significance Difference was utilized to make comparisons between pairs with p < 0.05 as the threshold for significance. Statistical analyses were performed with SPSS v25 (IBM, NY).
Results
Insertional forces
The ball-tip laser fibers generated significantly less insertional force on the ureteroscope liner than standard flat-tip laser fibers in all tested deflection angles (p < 0.001) (Fig. 2). In both 30° and 45° models, the average insertional force for the flat-tip laser fiber was more than twofold greater than for the ball-tip laser fiber (113.17 mN vs 59.28 mN and 319.75 mN vs 135.62 mN, respectively). In the 90° model, the force required for inserting the flat-tip laser fibers was 9264 mN compared with 200 mN for ball-tip laser fibers (Fig. 2). The stage controller was physically unable to pass the flat-tip fiber at 180° as the fiber would repeatedly catch at the point of deflection and recoil out of the model; for this reason, these trials were aborted.
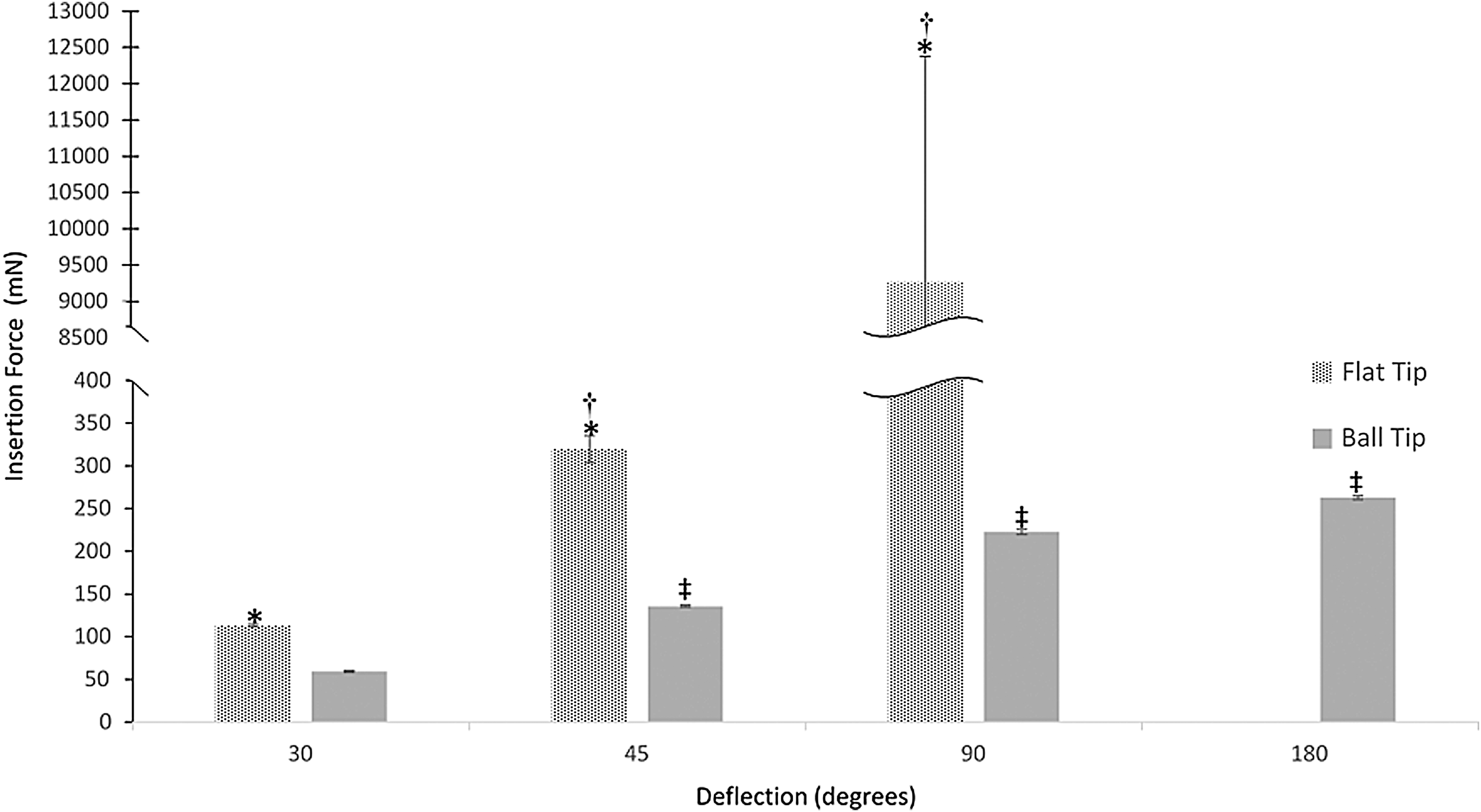
Mean insertion forces in mN between ball-tip and flat-tip fibers at 30°, 45°, 90°, 180° of deflection. Bars indicate 95% confidence interval. *Indicates greater flat-tip insertional forces than ball-tip to p < 0.001. †Flat-tip fibers—significantly greater insertional force needed than prior level of deflection. ‡Ball-tip fibers—significantly greater insertional force needed than prior level of deflection.
Damage to ureteroscope inner lining
Ball-tip laser fibers caused less damage to the ureteroscope liner than flat-tip laser fibers. At all tested deflection angles, ball-tip laser fibers completed all the trials and passed through each ureteroscope working channel model without causing a leak. In the 45° model, flat-tip fibers caused liner leaks in two of four trials at pass 91 and 114 (Fig. 3). Of note, the perforations occurred with 1710 and 1990 mN of force, respectively. The respective mean force applied per pass before the perforations was 300 and 290 mN, representing a 5.5- and 6.9-fold acute increase in insertion force at the time of perforation. On a separate 45° liner, multiple passes between 1000 and 1421 mN did not result in perforation. In the 90° model, flat-tip fibers caused liner leaks after the first pass in all four sheaths. As stated above, the stage controller was unable to pass the flat-tip fiber at 180°.
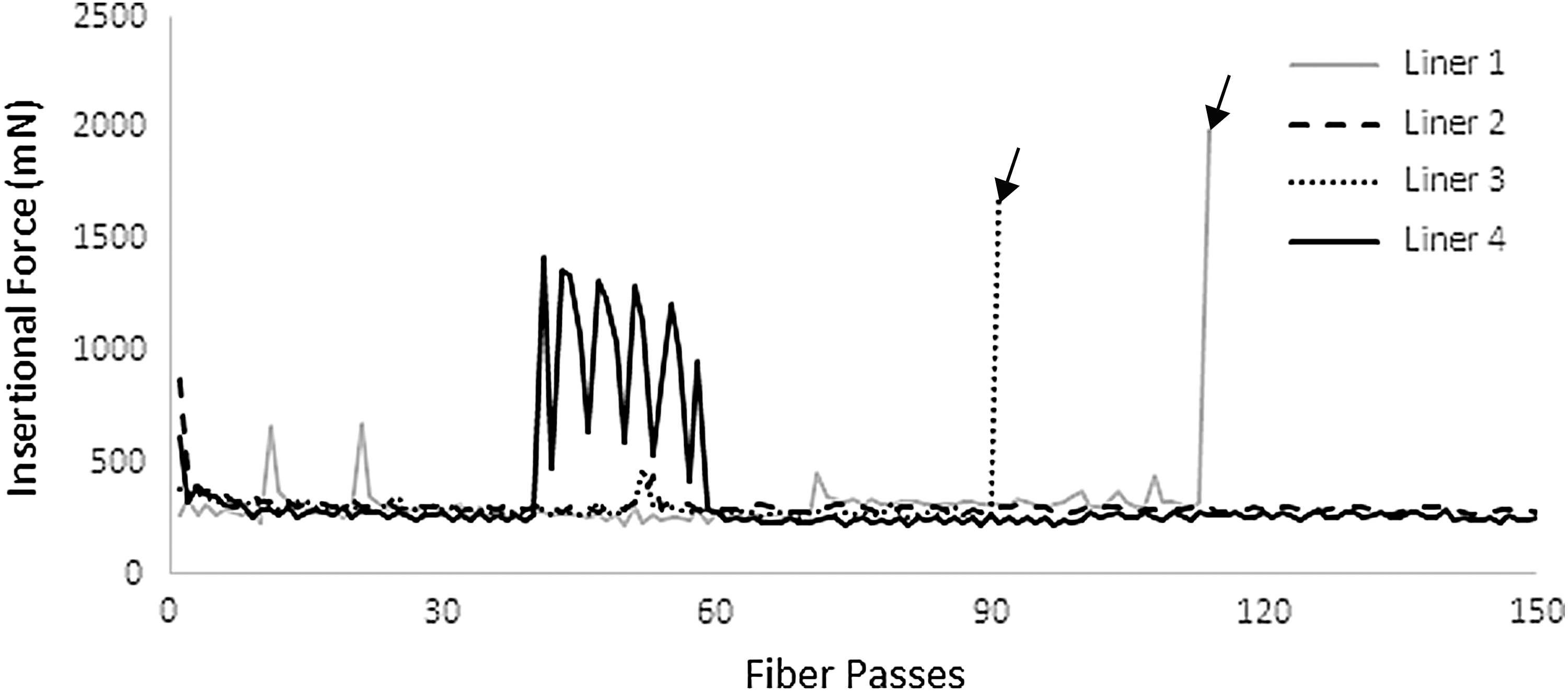
Flat-tip fiber passes at 45°. Perforations noted with arrows at passes 114 and 91 for liners 1 and 3, respectively.
Discussion
Modern flexible ureteroscopes are smaller with powerful optics and have improved flexion capabilities. These advances have increased the breadth of endoscopic interventions for both benign and malignant urologic diseases. 13 However, this technical improvement comes with a price; flexible ureteroscopes are fragile. In an effort to decrease the risk of scope damage and its financial ramifications, the ball-tip laser fiber was developed to reduce friction-induced working channel liner damage.
Our study suggests that at clinically applicable angles of deflection, the ball-tip fiber required significantly less insertional force when compared with the flat-tip fiber. In addition, high-volume ball-tip fiber passage never resulted in liner perforation. While the flat-tip fiber's increased insertional forces did not result in liner damage at 30°, two of four liners were perforated at 45° of deflection and all four liners were compromised at 90° with just a single pass. As such, there seems to be a gradient in which a scope liner is more prone to perforate with increased scope deflection. Perforations started to occur at 45°, a relatively small angle of deflection that is commonly used, and exceeded to reach caliceal stones during flexible ureteroscopy.
The transition point of this gradient appears to be at 45° of deflection in which not all liners were discernably damaged and those with perforations had them well into the 150 passes allotted to each. After 114 and 91 passes, liners 1 and 3 perforated with 1992.3 and 1705.7 mN of force, respectively. At the same time, liner 4 required ∼1000 to 1421.3 mN of force for passes 41 to 55, but did not perforate. These findings suggest that the liner's perforation threshold could be as little as ∼1700 mN, which amounts to the force a large apple applies to the table it rests on. This relatively small amount of force required to damage a ureteroscope at just 45° of deflection is disproportionate to the high costs associated with scope repair. This 45° may seem like a relatively safe angle of deflection to insert a flat-tip laser fiber; however, our results suggest otherwise. No perforations occurred at 30°. To avoid liner perforation when advancing a flat-tip laser fiber ureteroscopes should remain at zero flexion as much as possible, and ideally should not exceed 30°. However, there are clinical scenarios where repositioning a stone out of the lower pole or reducing ureteroscope deflection to pass a laser fiber is not feasible. As such, it is our practice to use ball-tip fibers routinely during flexible ureteroscopy.
Others have evaluated the TracTip laser fiber and compared it with a standard flat-tip fiber, however, our study is the first to evaluate the potential for each to damage a ureteroscope's working channel lining at increasing levels of deflection. Shin and colleagues showed that ball-tip fibers required less insertional force than the flat-tip fibers within a sheath deflected to 270°. 14 While this information was helpful, there are not many clinical scenarios that require laser fiber passage with the scope deflected to 270°. In an effort to produce a more clinically relevant in vitro environment, we tested laser fiber passage at ureteroscope deflections of 30°, 45°, 90°, and 180°.
There has been disagreement regarding the durability of the ball-tip. Shin and colleagues found that tip degradation was comparable between ball- and flat-tip fibers at both high-energy low-frequency and high-frequency low-energy settings. 14 However, another study noticed robust ball-tip degradation after short-term use at low-frequency high-energy settings and comparable tip degradation between ball-tip and flat-tip fibers at high-frequency low-energy settings. 15 Differences in experimental design could explain the differing results. Nevertheless, at 90° of deflection, we noted perforations with the flat-tip fiber on the first pass on each of the four liners. While there exists conflicting evidence for the ball-tip's durability, even in the worst-case scenario in which the ball-tip does quickly degrade, it would protect against perforations on initial passage when the scope is deflected ≥90°.
At 45° of deflection, we noted liner perforations after 91 and 114 passes. Some may question the ball-tip's protective utility in a single flexible ureteroscopy case when a fiber may be inserted and extracted only a handful of times. However, 90+ fiber passes through a single ureteroscope working channel may occur over a number of weeks or months in typical urologic practice. During that time, the channel liner is not just subjected to laser fibers but also to the passage of other endoscopic instruments such as stone baskets, biopsy forceps, brushes, graspers, as well as rigorous sterile processing that can further weaken the lining. Considering these factors, consistently using a ball-tip fiber could be a simple way to reduce further mechanical wear on the working channel lining.
Previous studies suggest that expensive major repair of a flexible ureteroscope is needed after 5 to 40 cases. 2 –5 In addition, more frequent maintenance is required when the scope is deflected to access the lower pole. 5 Common causes for ureteroscope repair include damage to the working channel, loss of active tip deflection, poor optics, and shaft damage. 16,17 In one study, damage to the working channel accounted for 52% of all causes for ureteroscope repairs, and 50% of working channel damage was related to repeated passage of instruments. 18 Previously described measures to mitigate scope liner damage include introducing working channel elements when the ureteroscope is not deflected, using a ureteral access sheath and relocating a lower pole stone to a more accessible position. 19,20 Unfortunately, such maneuvers are not always feasible and our data suggest that ureteroscope inner lining can be perforated by passing instruments even when the ureteroscope is just deflected 45°. In addition, some factors of ureteroscope longevity are out of the surgeon's direct control, such as damage during pre- and postoperative room turnover and sterile processing. At our institution, a ball-tip fiber costs approximately $70 more than a standard flat-tip. In the dynamic operating room environment, consistently using a ball-tip fiber for flexible ureteroscopy may be a reliable and relatively low-cost method to reduce flexible ureteroscope wear.
Our study does have a few notable limitations. First, our model does not account for ball-tip degradation as all laser fibers tested were unused. Given this limitation, our results may not be translatable to a fiber that no longer has a discernable ball on its tip after burnback from laser use. To avoid tip burnback low-power, high-frequency energy settings, as used to dust a stone, can be used to minimize ball-tip degradation. 21 Based on our present study, it is unclear whether it is safe to insert the ball-tip fiber repeatedly through the working channel once it has already been used for lithotripsy. Also, while we did use an actual flexible ureteroscope working channel sheath, this is an in vitro study and does not represent a true clinical scenario.
Another potential limitation is that the 3D mold which housed the working channel sheath at a prescribed angle is potentially more rigid than a flexible ureteroscope. This may explain why the flat-tip fiber perforated the ureteroscope liner on the first pass of each run at 90° deflection. However, despite constitutional differences in our 3D mold, the laser fiber insertional forces we collected from our model are similar to forces reported when a laser fiber is advanced within a real flexible ureteroscope. 21,22 One of these studies evaluated a flat-tip 200 μm laser fiber within a FlexGuard fiber sheath and recorded mean fiber insertional forces of 200 at 300 mN when two different ureteroscopes were deflected to 150°. 21 In our study, at 45° of deflection, aside from episodes of perforation, the flat-tip fiber passes averaged 320 mN of force. Our mean forces for the ball-tip fiber were similar as well, particularly at the angles of deflection most similar to 150° (90° and 180°): 30°–60 mN, 45°–140 mN, 90°–220 mN, 180°–260 mN. These results are further corroborated by another study which showed that an average of 320 mN of force was required to advance a 200 μm flat-tip ScopeSafe laser fiber (with a Scope Guardian fiber sheath) through a flexible ureteroscope angled at 270°. 22 In the end, our model yielded insertional forces consistent with prior studies that measured forces through a real flexible ureteroscope. This similarity suggests that the insertional forces and perforation thresholds we collected from our 3D model are clinically applicable.
Finally, we did not cleave the flat-tip laser fiber before sheath passage. Flexiva flat-tip fibers are polished and cleaving their end would obviate the polished coating designed to facilitate the passage through a ureteroscope. 15,24 Others have suggested that cleaving of the flat-tip fibers may reduce scope damage during fiber passage, but we aimed to compare the fiber types as per manufacturer's specifications as we currently use them in clinical practice. 25
Conclusions
A ball-tip holmium laser fiber can be safely passed through a deflected ureteroscope liner without causing identifiable damage at deflection angles up to 180°. The standard flat-tip fiber requires up to five- to sevenfold greater insertion forces at all angles and causes the ureteroscope liner to leak if deflected 45° or more. Consistent use of a ball-tip fiber may decrease liner damage and reduce flexible ureteroscope repair requirements.
Footnotes
Author Disclosure Statement
Both M.E.L. and G.M.P. serve as consultants for Boston Scientific.