
Abstract
Objectives:
Literature regarding experience with three-dimensional (3D) laparoscopy in urology has remained scanty, and this might be also related to the parallel explosion of robot-assisted laparoscopic surgery. The study aim was to compare 3D vs two-dimensional (2D) laparoscopic approaches for urological procedures in perioperative outcomes in a subgroups analysis of studies reporting procedures requiring intracorporeal suturing.
Materials and Methods:
We searched EMBASE and Medline from database inception to September 22, 2017 for studies comparing patients undergoing 2D vs 3D laparoscopic approach for urological procedures. Two investigators independently selected studies for inclusion. Studies identification and selection was performed according to PRISMA criteria. Quality of the studies was assessed by the Newcastle-Ottawa and the Jadad scales for nonrandomized controlled trials (RCTs) and RCTs, respectively. For continuous variables, weighted mean difference was used for quantitative synthesis; for categorical variables, the odds ratio with confidence interval (95% CI) was used instead. A random-effect model was used for pooled estimates to account for heterogeneity. Statistical analyses were performed using RevMan 5.3 (Cochrane Collaboration, Oxford, United Kingdom).
Results:
Eight comparative studies of interest published in English were found and considered for the quantitative synthesis. Among them, four were RCTs. Six studies regarded procedures requiring intracorporeal suturing and were considered for cumulative-analysis. Meta-analysis did not show any significant difference in operative time. Quantitative synthesis showed advantages for 3D laparoscopy in terms of operative time, blood losses, and length of stay. When limited to studies regarding radical prostatectomy, operative time significantly favored 3D approach (mean difference −35.00, 95% CI −41.34 to −28.67 minutes).
Conclusions:
The present systematic review and cumulative-analysis indicated that 3D laparoscopy could offer some advantages in terms of operative time for more challenging procedures requiring intracorporeal suture.
Introduction
L
In this context, three-dimensional (3D) imaging technology was introduced. In the early 1990s Wenzl et al. 5 first described a gynecological laparoscopic procedure using 3D technology. Initially, the 3D display was based on “Shutter Glass” technique, providing poor-definition images. Moreover, it was harmful to the eyes of the surgeon. Thanks to technological improvements, Film-type Patterned Retarder 3D laparoscopes were subsequently introduced. Such new-generation 3D laparoscopy had high-definition stable images, reducing the visional stress for the surgeon. In 2012, Buchs and co-workers first reported a smooth operation by Film-type Patterned Retarder glasses. 6 From then on, 3D laparoscopy knew a worldwide diffusion. 7 A recently published meta-analysis on general surgery procedures concluded that 3D laparoscopy should be the preferred over 2D laparoscopy for the superior surgical efficacy. 8
On the other hand, literature regarding experience with 3D laparoscopic procedures in urology has remained scanty, and this might be also related to the parallel explosion of robot-assisted laparoscopic surgery. 9 –11
Aim of this systematic review was to explore the current status of 3D laparoscopy in urology, and to determine the advantages and the outcomes of 3D laparoscopy for urologic procedures requiring intracorporeal suturing.
Evidence Acquisition
Search strategy and article selection
A systematic review limited to articles in English language published until September 2017 was performed. A specific search on PubMed and Embase databases included dedicated search strings. All studies reporting data of interest were collected. Only studies reporting on the use of 3D laparoscopy in the field of Urology (as determined by type of procedure, journal where study was published, or authors' affiliation) were considered for inclusion. Editorials, commentaries, abstracts, reviews, book chapters, and studies reporting experimental studies on animal or cadaver were excluded from the review. Articles reporting the use of 3D laparoscopy in training were also excluded. Two of the authors (E.C. and D.A.) independently reviewed the literature according to the inclusion and exclusion criteria. Title and abstracts were reviewed accounting for the inclusion criteria. After the screening, full text analysis was performed to confirm the selected articles inclusion. References from the pooled articles were reviewed to identify additional studies of interest. Disagreements about eligibility were resolved by a third party (R.B.) until consensus was reached. Guidelines set out by (Preferred Reporting Items for Systematic Reviews and meta-analysis statement) PRISMA were followed. 12
Assessment of quality of the studies and publication bias
Extracted studies were distinguished according to the 2011 Oxford Centre for Evidence-based Medicine level of evidence for therapy studies. Retrieved data were recorded in a dedicated data extraction form. Protocol was submitted to Prospero (
The study quality was assessed by the Newcastle-Ottawa scale (NOS) for nonrandomized controlled trials (RCT), 13 considering a total score of 5 or less low quality, 6 to 7 considered intermediate quality, and 8 to 9 considered high quality. The Jadad scale was used for RCT. 14 Studies were scored between 0 (very poor quality) and 5 (rigorous quality). Funnel plots were used to assess the risk of publication.
Data extraction and analysis
A dedicated data extraction form was used to collect the data of interest. Baseline demographics (age, BMI) and perioperative variables (operative time, blood losses, complications, and length of stay) were recorded whenever available. The weighted mean difference was used as a summary measure for continuous outcomes, whereas the odds ratio (OR) with confidence interval (95% CI) was used for categorical variables. A validated mathematical formula was used to convert medians and ranges to means and standard deviations, when needed. 15 A random-effect model was used to account for heterogeneity in pooled estimates. RevMan 5.3 software was used for statistical analysis (Cochrane Collaboration, Oxford, United Kingdom).
Evidence Synthesis
The electronic search identified a total of 1.653 articles in PubMed and Embase. Of these, 241 publications were identified for detailed review after exclusions for wrong subject, which yielded a total of 8 articles included in the present systematic review (PRISMA flow diagram was reported in Fig. 1).
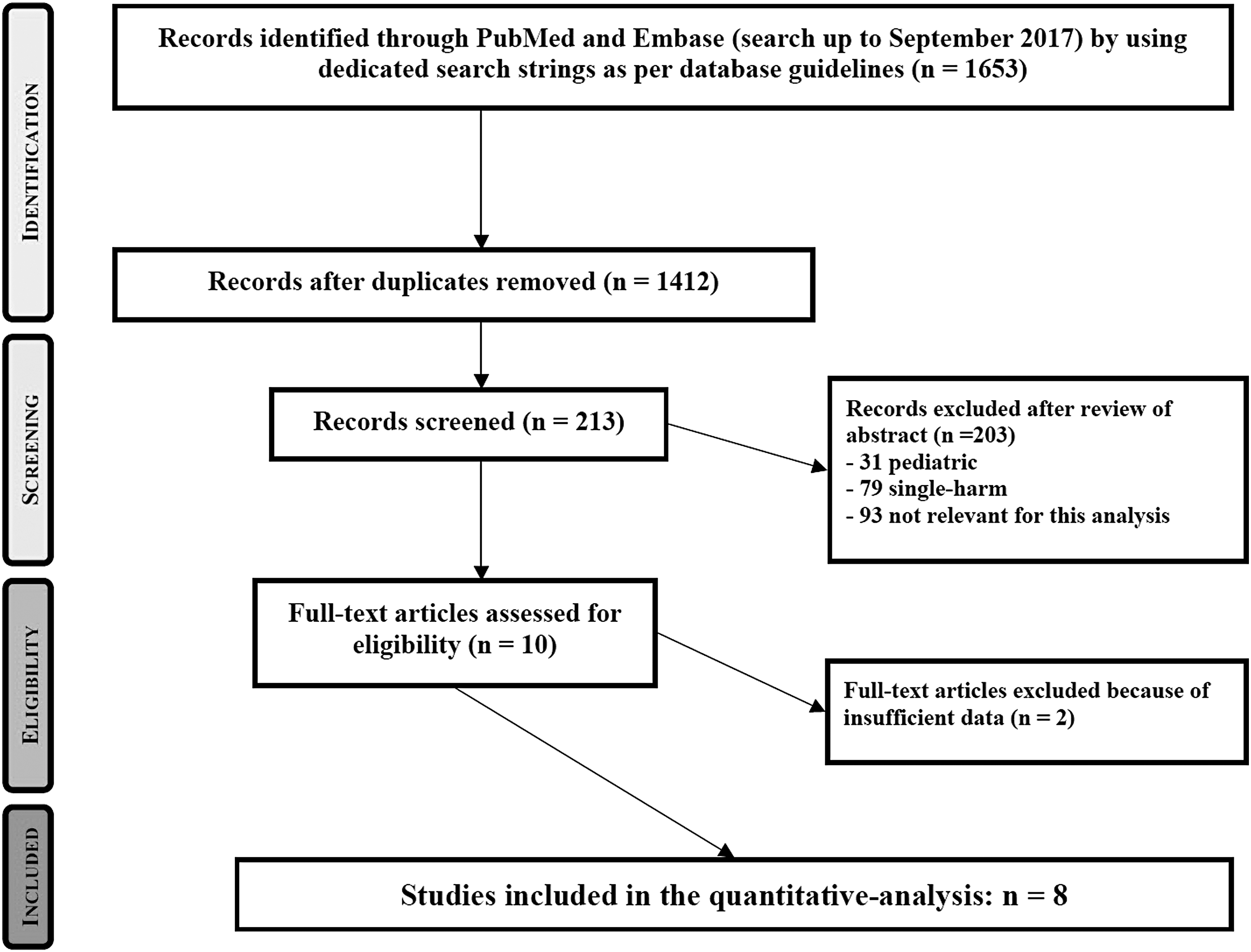
PRISMA flow for study selection and inclusion PubMed search string: (“Imaging, Three-Dimensional”[Mesh] OR 3D OR 3-D OR three-dimension* OR 3-dimension*) AND (“Laparoscopy”[Mesh] OR “Laparoscopes”[Mesh] OR laparosc* OR laparoendosc* OR celioscop* OR “Minimally Invasive Surgical Procedures”[Mesh:NoExp] OR minimally-invasive-surg*) AND (“Urinary Tract”[Mesh] OR “Genitalia, Male”[Mesh] OR “Male Urogenital Diseases”[Mesh] OR “Urologic Diseases”[Mesh] OR “Urologic Surgical Procedures”[Mesh] OR urol* OR kidney* OR renal OR nephrect* OR nephropex* OR nephroureter* OR ureter OR ureteral* OR ureterect* OR bladder* OR prostate* OR cystectom* OR varicocele* OR cryptorchid* OR retroperitoneal-lymph-node* OR pelvic-lymph-node*). Embase search string: ((‘three dimensional imaging’/exp OR 3d OR ‘3 d’ OR ‘three dimension*’ OR ‘3 dimension*’) AND (‘laparoscopy’/exp OR ‘laparoscope’/exp OR laparosc* OR laparoendosc* OR celioscop* OR ‘minimally invasive surgery’/de OR ‘minimally invasive surg*’) AND (‘urinary tract’/exp OR ‘male genital system’/exp OR ‘urinary tract disease’/exp OR ‘male genital system disease’/exp OR ‘urologic surgery’/exp OR urol* OR kidney* OR renal OR nephrect* OR nephropex* OR nephroureter* OR ureter OR ureteral* OR ureterect* OR bladder* OR prostate* OR cystectom* OR varicocele* OR cryptorchid* OR ‘retroperitoneal lymph node*’ OR ‘pelvic lymph node*’)) NOT ‘gynecologic surgery’/exp.
Characteristics of the included studies were reported in Table 1. Among them, four articles were RCTs: one article reported about laparoscopic partial nephrectomy, 16 one about laparoscopic radical prostatectomy, 17 one about living donor nephrectomy, 18 one about laparoscopic radical and simple nephrectomy and pyeloplasty. 19
2D = two-dimensional; 3D = three-dimensional; LA = laparoscopic adrenalectomy; LDN = laparoscopic living donor nephrectomy; LN = laparoscopic simple nephrectomy; LP = laparoscopic pyeloplasty; LPN = laparoscopic partial nephrectomy; LRN = laparoscopic radical nephrectomy; LRP = laparoscopic radical prostatectomy; RCT = randomized controlled trial.
Overall, the total sample-size was 704 (2D laparoscopy: 408; 3D laparoscopy: 296).
For RCTs, the total cohort was 436 (2D laparoscopy: 236; 3D laparoscopy: 200). As concerning the number of patients who underwent procedures requiring intracorporeal suturing available for pooled analysis, 256 and 205 were in 2D and 3D, respectively. Analyzed studies were confirmed to be comparable after accounting for patients' demographics (age, gender, p > 0.05).
Methodological quality
All non-RCT studies were assessed as good quality trials in methodology, with NOS ≥7.
At Jadad's scaling, the majority of RCT were found of acceptable quality (≥3 points), except for the study by Wahba and colleagues 18 (Table 1).
Study endpoints
Operative time
The cumulative analysis of procedures requiring intracorporeal suture (radical prostatectomy, pyeloplasty, and partial nephrectomy), found a mean difference in operative time of 10.90 minutes in favor of 3D laparoscopy (95% CI −14.82 to −6.98 minutes, Fig. 2A), while no difference was found by meta-analysis (mean difference 3.32, 95% CI −2.12 to 8.76 minutes, Fig. 2B).
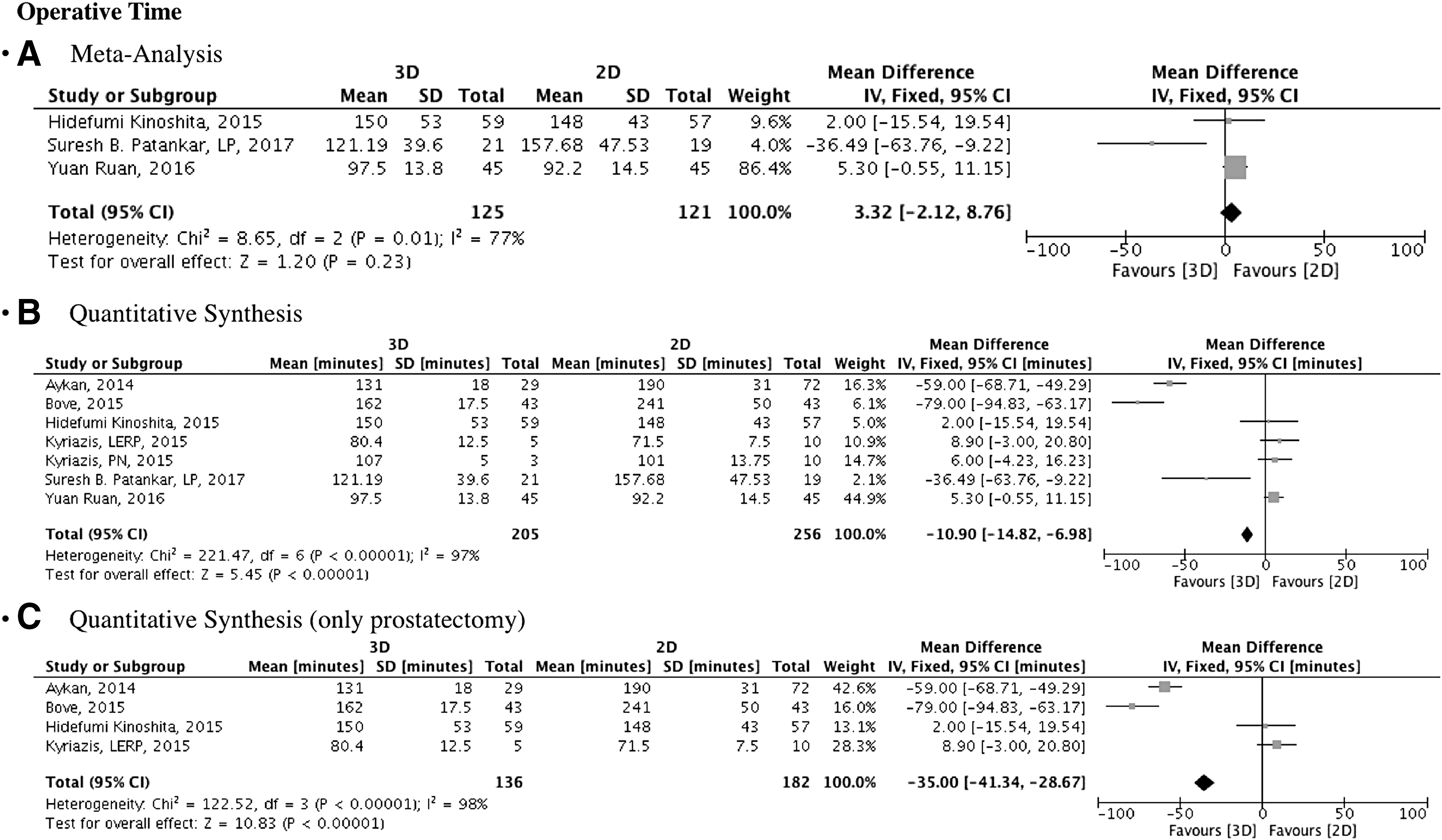
Forest plots of operative time:
A specific analysis was performed on this outcome for studies regarding radical prostatectomy: 136 and 182 patients were considered at quantitative synthesis for 3D and 2D laparoscopy, respectively. The analysis significantly favored 3D approach (mean difference −35.00, 95% CI −41.34 to −28.67 minutes, Fig. 2C).
Blood losses
The cumulative analysis of the procedures requiring intracorporeal suture found a significant difference in blood losses favoring 3D laparoscopy (mean difference −21.55 mL, 95% CI −28.51 to −14.59 mL). Neither meta-analysis nor specific analysis per procedure was possible due to lacking data (Fig. 3A).

Forest plots of
Postoperative complications
Specifically regarding procedures requiring intracorporeal suturing, postoperative complications were found to be comparable between 3D and 2D laparoscopy at cumulative analysis (OR 0.61, 95% CI 0.24–1.57 and OR 0.60, 95% CI 0.22–1.61, respectively) No meta-analysis was possible due to low cases available (Fig. 3B).
Length of stay
At quantitative synthesis, length of stay was found to be significantly shorter for 3D laparoscopy (−0.55 days, 95% CI −0.82 to −0.29 days). No meta-analysis was possible due to low cases available (Fig. 3C).
Discussion
The present systematic review and cumulative-analysis was able to generate some important considerations about the role of 3D and 2D laparoscopy in urology.
Limited to the pooled procedures requiring intracorporeal suturing (namely radical prostatectomy, pyeloplasty, and partial nephrectomy), meta-analysis did not show any significant difference in operative time between the two approaches. Unfortunately, other perioperative outcomes were not meta-analyzed due to lacking data.
It is known that such procedures are challenging if performed by laparoscopic approach, as requiring advanced laparoscopic skills such as needle control and driving and intracorporeal suturing. We acknowledge that it would have been expected a preponderance of 3D laparoscopy against 2D laparoscopy in such more challenging procedures, mainly attributed to the more stereoscopic surgical view. Indeed, as previously reported by one of the first studies in the field performed by the European Institute of Telesurgery, Strasbourg, stereoscopic vision appears to be able to significantly enhance the performance of laparoscopy. 20 Moreover, this advantage persists beyond the surgeon's learning curve and it is accentuated as the laparoscopic tasks become more complex. The tridimensional reconstruction of target region is able to facilitate the estimate of anatomic depth, thus increasing the accuracy of surgical manipulation. 21
In the Kinoshita RCT, although superiority of 3D laparoscopy of over 2D was not demonstrated in perioperative outcomes, the authors concluded that 3D imaging systems might have a substantial role in laparoscopic surgery. Notably, a subjective evaluation by surgeons was performed by validated questionnaire showing that 3D imaging was better and did not increase fatigue. 17 3D imaging has been questioned to be more likely to cause visual strain and headache by reports from general surgery. 22 Moreover, dizziness and eye fatigue have been observed at a higher rate in beginner laparoscopic surgeons. 23 As such, Kinoshita and co-workers warned that although in their study no surgeons complained about significant symptoms caused by the use of the 3D, there is the potential that some surgeons may not adapt to 3D imaging given the prevalence of the described adverse effects in spectators of 3D stereoscopic movies, such as fatigue, feeling of sickness, headache, and nausea. 17,24
In Patankar and Padasalagi RCT, the State-Trait Anxiety Inventory score was used to quantify emotional, physical, and cognitive aspects of stress experienced during the surgical procedure. 19 Results significantly favored 3D laparoscopy, confirming previous reports stating that surgeons can work faster and safer under 3D vision, especially during crucial and complicated surgical maneuvers. 25 Due to the disagreement between the results of the present meta-analysis and the surgeon's perception reported by available studies we then performed a quantitative synthesis on all the outcomes available.
Interestingly, as concerning the operative time, we were able to perform a quantitative synthesis of the outcome limited to radical prostatectomy only, on a total number of 318 patients (136 vs 182, 3D vs 2D, respectively). Results strongly favored 3D laparoscopy, with a mean difference of 35 minutes less (95% CI −41 to −29). Undoubtedly, the anastomosis step during laparoscopic prostatectomy increases the difficulty of the procedure over other urological procedures not requiring intracorporeal suture, and this is the possible explanation of the finding. Confirming our finding, at multivariate logistic regression analysis, the RCT by Kinoshita et al. found the 3D imaging system as significant predictor of shorter time spent for urethrovesical anastomosis, with an OR of 3.5 vs 2D (p = 0.014). 17
Unfortunately, meta-analysis of the outcome was not possible, but we underline that the evidence is based on one RCT, 17 one prospective study, 26 one prospective study with historical comparative cohort, 27 and one retrospective study. 28
As concerning the blood losses, a mean difference of 20 mL favoring 3D laparoscopy was found at quantitative synthesis. Specifically regarding the blood losses outcome, we point out that the method used for reporting the blood losses is not rigorous in all the cases. Indeed, they are often mentioned as “estimated” blood losses. As previously reported, the visual estimation of intraoperative blood losses can be unreliable and inaccurate. Moreover, no provider specialty, level of experience, or self-assessment of ability is associated with an improved estimation. This is why the blood loss estimation is not considered as a reliable metric to judge the surgical performance. 29 Moreover, some studies just reported that no significant differences in terms of intraoperative blood losses were found, without reporting the data or stating they were “negligible.” 27,30 Last, we sincerely believe that 20 mL of increased blood loss is clinically relevant.
As concerning the postoperative complications outcome, 3D and 2D laparoscopy were found to be comparable at quantitative synthesis, with an average rate around 5%. We acknowledge that the quality of the report of complications was generally low in the extracted studies. Moreover, procedures considered were heterogeneous, thus preventing to draw consistent conclusions specifically regarding the outcome.
Finally, we were able to perform quantitative synthesis of the length of stay. We found it was significantly shorter for 3D laparoscopy in procedures requiring intracorporeal suture. Having said this, the average advantage of 3D over 2D laparoscopy was 0.5 day, preventing us again to draw definitive conclusions.
The available 3D systems are attractive but more expensive than 2D systems. The goal of 3D laparoscopy is to try to fill the enormous gap between 2D laparoscopy and robotic surgery, by providing some advantages of robotics at cheaper costs. 31
Bhayani and Andriole questioned whether robotic surgery is able to offer any advantages over a smaller, less expensive 3D system. 32 With a comparable quality in the 3D vision, it is possible that the learning curve of laparoscopy becomes similar to that of robotic surgery. In such scenario, the costs would favor the acquisition of a 3D laparoscopy tower, that roughly is one-tenth the price of the robotic system. Moreover, a 3D laparoscopy tower is versatile, and could be adopted for any kind of laparoscopic intervention in different surgical specialties.
Park and colleagues published a comparative study among 2D laparoscopy, 3D laparoscopy, and robotic surgery. Beginners and expert laparoscopic surgeons were involved. The authors concluded that robotic surgery is particularly helpful in the naïve laparoscopic surgeons. Conversely, expert surgeons are equally good in surgical tasks whatever the technology. 33 This finding was confirmed by Andras and co-workers, reporting that prior experience in robotic surgery ensures a fast transition to 3D laparoscopic approach for radical prostatectomy, with comparable oncologic and functional outcomes, but with a shorter operative time and reduced costs. 34,35
Notwithstanding the possible economic advantages of 3D laparoscopy over robotics, we have to acknowledge that patients are attracted by the robotic technology and will continue to be attracted by robotic technology, regardless the surgeon's experience. 36
On the other side, there are several open surgeons who are embracing the robotic technology to remain competitive, and several residents or young urologists who are being trained mainly for robotic surgery.
These considerations together with the level 1 evidence finding of the present systematic review and meta-analysis of operative time are a possible explanation of the limited role of 3D laparoscopy in the urological field (reflected by the few available studies).
Although the methodology of the present systematic review with meta-analysis and quantitative synthesis was attempted to be rigorous, we acknowledge some limitations. First, despite a subgroup analysis focused on the procedures including intracorporeal suturing was performed, we are unable to state that heterogeneity among the procedures was eliminated. Second, the number of included studies was low and limited the sample size in the pooled analysis.
Third, the available literature reports perioperative outcomes in a heterogeneous fashion that were sometimes hard to be pooled. In addition, one can argue that the differences in the surgical technique and in the surgeon experience in each of the considered interventions might represent another source of bias.
Notwithstanding these limitations, our systematic review and cumulative-analysis indicated that 3D laparoscopic approach for urological procedures requiring intracorporeal suturing is able to offer some advantages in terms of perioperative outcomes over the standard 2D laparoscopy. Having said this, operative time is not significantly longer at meta-analysis of data.
Conclusions
Based on our results, 3D laparoscopy is able to offer some advantages over 2D laparoscopy in terms of operative time, blood losses, and length of stay. It could be considered as a viable alternative approach to facilitate more complex surgical gestures if robotic system is not available. Available subjective evaluations by surgeons showed the surgical vision superior with 3D, without increasing eye fatigue, but there is the potential that some surgeons may not adapt given the prevalence adverse effects in the general population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.