
Abstract
Objectives:
To compare functional outcomes of warm ischemia RPN (wRPN) to cold ischemia RPN (cRPN) in “at risk” patients.
Materials and Methods:
Retrospective review of institutional database queried for all patients who underwent cRPN/wRPN (January 2007–December 2016). For the study purpose, patients with solitary kidney and/or history of partial nephrectomy and/or multiple tumors and/or preoperative estimated Glomerular Filtration Rate (eGFR) <60 mL/minute were extracted. To reduce inherent biases, groups were matched on key variables related to renal function through a greedy matching algorithm with no replacement. Renal functional outcomes were evaluated by eGFR drops at 1–3 days and at 1, 3, 6, and 12 months postoperatively. A linear mixed effects model was used to assess eGFR at each follow-up who received either cRPN or wRPN. Follow-up was treated as a factor variable to account for nonlinear time trends. Contrast analysis was used to compare cRPN vs wRPN groups at each follow-up, using Sidak–Holm p-value adjustments for multiple comparisons.
Results:
Out of 19 cRPN patients and 279 wRPN patients, 14 cRPN patients were finally matched 1:1 with no replacement to 14 wRPN. There was no significant difference in preoperative eGFR for matched patients undergoing cRPN vs wRPN. Since the first postoperative day, cRPN patients had higher eGFR. The difference was statistically significant since the third month postoperatively (mean difference = 18.201, 95% confidence interval [CI]: 1.930–34.472) and remained at both the sixth month (mean difference = 18.839, 95% CI: 2.568–35.109) and the 12th month (mean difference = 21.277, 95% CI: 5.006–37.547) follow-up.
Conclusions:
Accounting for unmodifiable and modifiable factors, in a cohort of highly selected patients “at risk” for postoperative significant decline in renal function after RPN, renal functional outcomes appear to be superior with cold ischemia technique.
Introduction
P
Most surgeons prefer the use of vascular clamping to improve the visualization of the tumor's borders, facilitating tumor resection and minimizing the risk of positive surgical margins. Moreover, a bloodless field allows for more precise renorrhaphy. 11 The most common method used to perform ischemia is clamping of the renal artery with or without the renal vein (the so-called “warm ischemia technique”). There is general literature consensus that limiting warm ischemia to less than 20–25 minutes is a reliable cutoff for preventing renal functional deterioration. 10,12 When longer ischemia time is expected due to patient and tumor characteristics, “cold ischemia technique” is recommended, as it has been reported to be able to increase the kidney's tolerance to ischemia time up to 45 minutes, 10,13 thanks to decreased intracellular metabolism and thus decreased oxidative injury associated with hypoxia and renal reperfusion. 14 –16 During open approach, ice slush for cooling the kidney is feasible and routinely used. Reproducing renal cooling during minimally-invasive approach, however, is more challenging. Indeed, multiple techniques have been described, including arterial infusion, 17 endoscopic retrograde ureteral cooling, 18 and cooling through renal surface irrigation. 19 The use of intracorporeal ice slush to obtain renal hypothermia during robotic PN (RPN) was first described by Rogers and colleagues with direct instillation of ice slush onto the surface of the kidney. 20 Our group then described a simplified modification of that technique. 21
Nevertheless, available experiences in the literature have remained anecdotal as cold ischemia technique is challenging to apply during robotic surgery. Trying to fill the gap, we designed the present study to evaluate, after adjusting for factors potentially influencing renal function by a rigorous propensity score matching, the impact of ischemia technique during RPN on postoperative renal function in a selected cohort of patients.
The aim of the study was to compare the renal functional outcomes and trend of cold-ischemia and warm-ischemia technique RPN in patients “at risk” for postoperative functional deterioration after RPN.
Materials and Methods
Data acquisition
Our prospectively maintained PN database approved by the institutional review board (IRB 5065) was reviewed, and all patients who underwent RPN with cold and warm ischemia techniques between January 2007 and December 2016 were extracted.
For the study purpose, only patients with solitary kidney and/or history of ipsilateral previous PN and/or multiple tumors and/or preoperative estimated Glomerular Filtration Rate (eGFR) <60 mL/minute were extracted.
In addition, patients who experienced complications potentially affecting postoperative kidney function, such as urinary fistulas and kidney infections, were excluded.
RPNs with warm ischemia technique were performed by expert institutional robotic surgeons according to a standardized previously described technique. 22 RPNs with cold ischemia technique were performed by a single surgeon (J.K.) as previously reported. 21 In patients who underwent cold ischemia RPN (cRPN), the indication was an expected warm ischemia time >20 minutes at preoperative planning.
Outcome measurements
Patients' demographics and preoperative variables were reported, including age, gender, race, body mass index (BMI), Charlson's comorbidity index (CCI), 23 smoker status (active vs former vs nonsmoker), diabetes, hypertension, hyperlipidemia, American Society of Anesthesiology (ASA) score, and preoperative hemoglobin.
As for the tumors' characteristics, side, clinical size, clinical stage according to TNM (Tumor-Node-Metastasis), 24 and RENAL nephrometry score 25 were reported. To evaluate the renal functional outcomes, Serum Creatinine (SCr) and eGFR (as calculated by the Modification of Diet in Renal Disease formula 26 ) were used. Chronic kidney disease (CKD) was staged accordingly.
Perioperative variables included operative time, estimated blood loss, ischemia type and duration, use of sealants, intraoperative complications, and percentage kidney volume preservation, as assessed by the surgeon. 27
Postoperative data included postoperative complications as reported according to the Clavien classification 28 (with grade 3 or higher complications considered as major complications) and length of hospital stay. Regarding pathologic data, tumor size at final pathology, percentage of malignant lesions, and positive surgical margins were reported. Concerning the renal functional outcomes, SCr and eGFR were reported at 1–3 days and at 1, 3, 6, and 12 months postoperatively.
Statistical analysis
To reduce selection bias and potential confounding by the differences in general and clinical properties by groups, we performed a matched analysis. Matching was based on unmodifiable (age, sex, race, BMI, CCI, smoker status, diabetes, hypertension, hyperlipidemia, ASA score, baseline renal function assessed by eGFR, tumor size, tumor stage, and RENAL nephrometry score) and modifiable (ischemia time and percentage kidney volume preservation) variables. Three of the 19 patients who underwent cRPN (15.8%) and 53 of the 279 who underwent warm ischemia RPN (wRPN) (19%) were missing the aforementioned variables and, thus, were excluded. Sixteen cRPN patients (84.2%) and 210 (81%) wRPN patients were analyzed. We used a logistic regression model to calculate the propensity score (PS) for cold ischemia based on the variables among 226 patients. After exclusion of two unmatchable cRPN patients, using greedy matching algorithm with the PS, 14 cRPN patients were finally matched 1:1 with no replacement to 14 wRPN patients. The balance of the baseline variables was checked for the matched cohorts.
General characteristics of the groups at baseline were summarized with mean and standard deviation for continuous variables and frequency counts and percentages for the categorical variables. Student's t-test was conducted to compare means of continuous variables by groups, and Chi-square test was used to compare the frequency of categorical variables by groups.
Analysis of functional outcomes
A linear mixed effects model was used to assess eGFR at each follow-up for matched patients who received either cRPN or wRPN. Follow-up was treated as a factor variable to account for nonlinear time trends.
After modeling, contrast analysis was used to compare cRPN vs wRPN groups at each follow-up point, using Sidak–Holm p-value adjustments for multiple comparisons.
Time points considered included baseline (within 30 days of surgery) and at 1 and 3 days and at 1, 3, 6, and 12 months after surgery. The minimum follow-up was 12 months. eGFR measurements >12 months post-RPN were not included to limit confounding variables on renal function. Statistical analyses were performed in R (R Project for Statistical Computing, Vienna, Austria) and JMP (SAS Institute, Cary, NC).
Results
After 1:1 matching, the balance of the key variables was checked, and the results showed that a good balance between the matched groups was achieved for all matched variables.
With respect to the prepropensity-score matched comparison (Table 1), after matching there was no significant difference between the groups (Table 2). In terms of perioperative outcomes, no differences were found between the matched cohorts (Table 3). Regarding pathologic data, groups were comparable in mean tumor size (4.0 ± 1.5 vs 3.7 ± 1.8 cm, p = 0.63), rate of malignant lesions (13/14, 93% vs 12/14, 86%, p = 0.55), and rate of positive surgical margins (1/14, 7% vs 0/14, 0%, p = 0.32, cRPN vs wRPN, respectively).
SD = Standard Deviation; ASA = American Society of Anesthesiology; CCI = Charlson's Comorbidity Index; eGFR = estimated Glomerular Filtration Rate.
Reported even if already mentioned among the covariates included in the propensity-score matching.
Hb = hemoglobin.
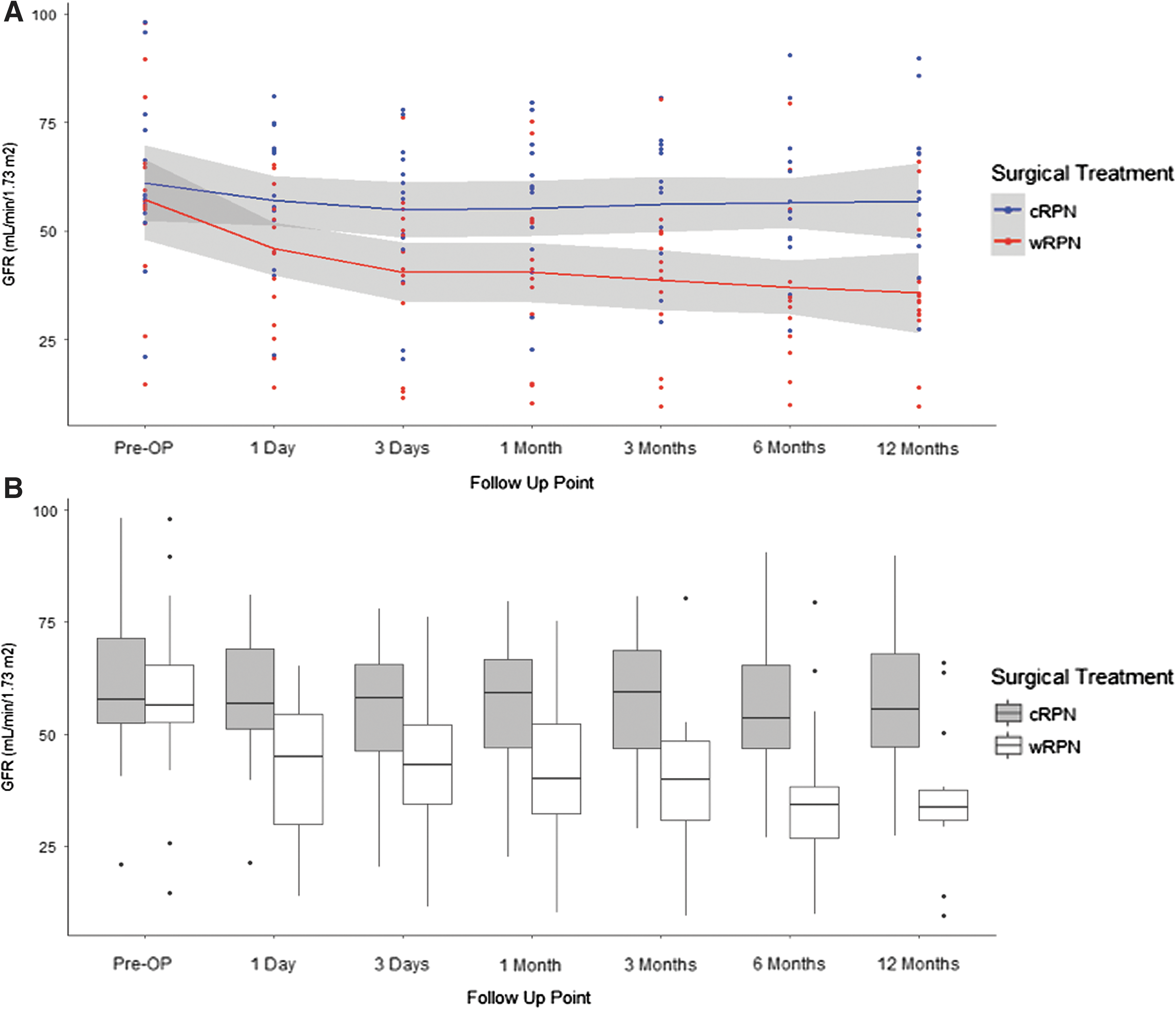
Concerning the functional data, there was no significant difference in preoperative eGFR for the matched patients undergoing cRPN vs wRPN. However, since the first postoperative day, a drop in renal function was observed in patients who underwent wRPN. The difference between cRPN and wRPN was statistically significant since the third month postoperatively, with patients treated with cRPN having significantly higher eGFR (mean difference = 18.201 [95% confidence interval (CI) = 1.930–34.472]). This difference remained at both the sixth month (mean difference = 18.839 [95% CI = 2.568–35.109]) and 12th month (mean difference = 21.277 [95% CI = 5.006–37.547]) follow-up points (Fig. 1, Supplementary Table S1; Supplementary Data are available online at
Discussion
In the present article, we analyzed a selected cohort of patients that can be considered at higher risk of renal functional deterioration after PN and are thought to benefit from a cold ischemia approach. After rigorous propensity score matching based on several factors potentially impacting renal functional outcomes after RPN, we found a significant difference in postoperative GFR favoring cold ischemia technique. Such difference was observed since the first day postoperatively, being statistically significant since the third month postoperatively and then at 6- and 12-month assessments.
We believe that our results are of note. Indeed, several prior studies have shown equivalency in functional outcomes when comparing cold vs warm ischemia technique PN. In 2011 Lane and colleagues published a multicentric study comparing 300 cold ischemia vs 360 warm ischemia PN performed for tumor in a solitary functioning kidney. At 3 months after PN they found that median eGFR decreased by equivalent amounts with cold or warm ischemia (21% vs 22%, respectively, p = 0.7), although the median cold ischemia time was longer (45 vs 22 minutes, respectively, p < 0.001). 29
In 2013, Kawahara and colleagues retrospectively compared 18 patients who underwent open PN with cold ischemia to 22 patients who underwent laparoscopic PN with warm ischemia. There was no significant difference between the groups in the reduction of eGFR. Paradoxically, eGFR loss in the open group was higher in patients experiencing >20 minutes of cold ischemia, whereas in laparoscopic group eGFR loss was higher when warm ischemia time was >30 minutes. 30
In 2014, Eggener and colleagues performed a multi-institutional analysis comparing 522 vs 874 patients who underwent open or laparoscopic PN with warm and cold ischemia technique, respectively. In their study, patients undergoing cold and warm ischemia demonstrated 12.3% and 10.1% reductions in renal function from baseline, respectively (p = 0.067). Increasing age, the female gender, and the increasing tumor size were strongly (all p-values <0.001) associated with reduction in renal function, but neither renal hypothermia nor surgical approach were predictive of renal function reduction. 31
In 2014, Jabaji and colleagues retrospectively evaluated a multicenter database, where 241 vs 31 patients underwent warm ischemia and cold ischemia PN, respectively. Authors did not find any significant differences in the proportion of patients developing de novo CKD between the groups (14.9% vs 15%, warm vs cold ischemia, respectively). 32
Zhang and colleagues retrospectively compared 112 cold ischemia PN vs 165 warm ischemia PN and found that the acute kidney injury, defined as a ≥1.5-fold increase in SCr above the preoperative level, strongly correlated with duration (p < 0.001) but not type of ischemia (p = 0.049). 33
In contrast, some reports found an advantage with cold ischemia technique. In 2014, Funahashi and colleagues retrospectively compared 59 patients who underwent open PN with warm ischemia to 64 patients who underwent open PN with cold ischemia. Notably, the authors used 99mTc-MAG3 renal scintigraphy to measure renal function. In addition, the regional 99mTc-MAG3 uptake was analyzed in the surgically unaffected parts to evaluate the ischemic damage. Authors concluded that 20–25 minutes of warm ischemia induced temporary renal injury recovered within 6 months, whereas warm ischemia >25 minutes caused irreversible damage. Conversely, cold ischemia up to 58 minutes was found to prevent ischemic injury. 34
In 2015, Abdeldaeim and colleagues published a prospective randomized study comparing 60 cold vs 60 warm ischemia patients with T1 renal tumors and CKD who underwent open PN. The authors found that patients undergoing warm ischemia were more prone to a postoperative decrease in eGFR, with a relative risk of 1.34 and 2 times at 3- and 24-month follow-up, respectively. 35 In 2015, Ramirez published a matched comparison based on preoperative eGFR, ischemia time, and RENAL score. cRPN was found to be associated with a 12.9% improvement in preservation of postoperative eGFR but no difference was seen at 6-month assessment. 36
Finally, in 2016 Yoo and coworkers published a propensity-score matched comparison of 30 patients who underwent wRPN vs 30 patients who underwent cold ischemia open PN. Cold ischemia open PN was superior to wRPN when ischemia time was ≥25 minutes. Conversely, wRPN offered comparable functional outcomes to those of cold ischemia open PN when ischemia time was <25 minutes. 37
Notably, the patients considered in the present analysis were selected to be at higher risk of functional deterioration after PN. They are questioned to be suitable candidates to benefit from a cold ischemia approach.
To account for inherent bias from a retrospective study, the cohorts of patients analyzed in the present study were matched in a rigorous method, accounting for a high number of factors influencing the renal functional outcomes after PN. Our findings showed a statistically and clinically significant difference between cold ischemia and warm ischemia technique during RPN, starting from the first month postoperatively and then remaining stable over time until the 1-year follow-up. Notably, we were able to match the patients according to the ischemia time duration too. The topic of renal ischemia has been one of the more controversial in the field of PN literature for decades. Ischemia intervals of 25–30 minutes have traditionally been accepted as preventing renal damage and long-term functional decline. 10,38 The results of our study show a benefit from cold ischemia technique even if some of the matched patients had ischemia time intervals within this threshold, confirming the protective role of cold ischemia.
There are several limitations to be mentioned. First, as with any retrospective design, some unmeasured and residual confounders that can account for differences in outcomes may exist. To reduce any measurable bias, a rigorous propensity score matching technique was applied, with a consistent number of variables considered, including the ischemia time duration and the percentage parenchymal volume preserved. Optimal matching was attained, with groups highly comparable in baseline characteristics and surgical factors of interest. As concerning the parenchymal volume preservation data, even if the surgeon assessment was proved to be valuable, 27 we acknowledge that more accurate methods are now available. 26 Finally, we acknowledge the low sample size, while underlining the selected population that could be of interest in the daily practice.
Conclusions
After controlling for measurable factors potentially influencing renal functional outcomes after RPN, in a cohort of patients “at risk” for postoperative significant decline in renal function, renal functional outcomes appear to be superior with cold ischemia technique.
Footnotes
Acknowledgment
The authors thank Cecelia Hanline for the language revision.
Author Disclosure Statement
J.H.K. certifies that all conflicts of interest, including specific financial interests and relationships and affiliations relevant to the subject matter or materials discussed in the article (e.g., employment/affiliation, grants or funding, consultancies, honoraria, stock ownership or options, expert testimony, royalties, or patents filed, received, or pending), are the following: Endocare, Inc., Intuitive—J.H.K. (consultant). The remaining authors (R.B., J.G., J.D., J.A., S.A., and M.L.) have no industrial relationship to disclose.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.