
Abstract
Background:
Laparoscopy is widely used in the urological field. This systematic review and a meta-analysis were conducted to assess the clinical and surgical efficacy of the three-dimensional (3D) laparoscopic system in comparison with two-dimensional (2D) laparoscopy for treatment of different urological conditions.
Methods:
Following guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses, a systematic literature search in Web of Science, PubMed, Cochrane Library, and EMBase was carried out to identify relevant studies published up to May 2018. Articles published in the English language of both randomized and observational studies comparing 3D and 2D laparoscopic systems in urological surgeries were included. Level of evidence and quality assessments of all included studies were conducted. Interested data were extracted for comparison and meta-analysis.
Results:
Our literature search generated 17 studies comparing 3D and 2D laparoscopic systems in different urological surgeries. Of these, 13 studies containing 548 and 449 patients operated on with 2D and 3D laparoscopic systems, respectively, were included for meta-analysis. These 13 studies were divided into three groups according to surgical type. Group 1: Partial nephrectomy (PN); operative time (p = 0.19), estimated blood loss (EBL) (p = 0.51), dissecting time (p = 0.58), and suturing time (p = 0.28) were not statistically significant between 2D and 3D laparoscopic systems. However, warm ischemia time during PN was significantly shorter during 3D laparoscopy (p < 0.00001). Group 2: Pyeloplasty; this procedure showed no significant difference between the two systems. Group 3: Radical prostatectomy (RP); shorter operative time (p < 0.0001) and lower EBL (p = 0.001) were associated with the 3D laparoscopic system.
Conclusion:
Three-dimensional laparoscopy mainly improves the depth of perception, leading to better visibility, which is important for some complex urological surgeries such as PN, pyeloplasty, and RP. Based on our findings, 3D laparoscopy seems to provide better clinical and surgical outcomes in some urological procedures compared with conventional 2D laparoscopy.
Introduction
C
There are three main challenges in laparoscopy: (1) the limited range of motion of laparoscopic instruments, (2) poor depth of perception in the two-dimensional (2D) laparoscopic imaging system, and (3) longer learning curve. To tackle these problems, new technologies have been developed such as laparoscopic robotized needle holders that can mimic the surgeon's hand movement 4 ; this instrument has simplified intracorporeal suturing difficulties. Other advances include the three-dimensional (3D) laparoscopic imaging system. 5 Together, these two technologies have improved intracorporeal dissection, suturing quality, ergonomics, and depth of perception during laparoscopic surgery.
Another significant milestone in the field of minimally invasive surgeries is development of the da Vinci robotic system (Intuitive Surgical, Inc., Sunnyvale, CA). Compared with conventional laparoscopy, da Vinci robotics provides better ergonomics and an excellent robotic arm (EndoWrist) that can rotate as much as 7° and is able to eliminate human hand tremors in addition to its impeded 3D imaging technology. However, a significant limitation of this system is the higher cost to purchase and maintain it. The cost of a da Vinci robotic machine ranges between 1 and 2.3 million dollars depending on the version and its configurations with an additional 180,000 dollars annually for maintenance. In comparison, the 3D laparoscopic system costs around 250,000 dollars plus 25,000 dollars of annual costs. 6 The above information clearly shows the economic benefits of the 3D laparoscopic system over da Vinci robotics.
The 2D laparoscopic system consists of a single camera (monoscopic), which is the primary reason why this system lacks depth of perception. On the other hand, 3D laparoscopy contains two side-by-side cameras (stereoscopic). Images from these two different cameras pass through an eyeglass in which each eyepiece corresponds to one camera. Finally, images are filtered and received as one; this leads to an increase of depth of perception. 7 Increased depth of perception is associated with higher accuracy and speed in performance, as well as a shorter learning curve. 8
Majority of the studies comparing 3D and 2D laparoscopic surgeries focused on novices, experts, residents, and students using training boxes, human cadavers, or animal models. 9 –11 However, there are some clinical trials and comparative observational studies comparing the efficacy, safety, clinical, and surgical outcomes between 2D and 3D laparoscopic systems. 12,13
Although considerable benefits were associated with the 3D laparoscopic imaging system over conventional 2D laparoscopy, the 3D laparoscopic system is not yet universally adopted. Based on the existing clinical literature, we conducted this systematic review and meta-analysis to assess the safety, efficacy, and clinical outcomes of 3D vs 2D laparoscopic imaging systems during different urological surgeries.
Methods
Search strategy
Two separate reviewers performed a systematic search in PubMed, Web of Science, Cochrane Library, and EMBase. We used the following search terms: “three-dimensional laparoscopic” or “3D laparoscopic” and “urology” or “adrenalectomy” or “nephrectomy” or “pyeloplasty” or “cystectomy” or “prostatectomy” to identify relevant studies published up to May 2018. We followed guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses. 14
Selection criteria
Inclusion criteria
Articles published in the English language or at least their abstract written in the English language.
Studies comparing 3D and 2D laparoscopic systems in urological surgeries only.
Both randomized and observational studies.
Both in adults and children.
Exclusion criteria
Studies that are not reporting patients, but instead comparing urology experts, residents, and students utilizing laparoscopic training boxes, human cadavers, or animal models.
Studies addressing 3D laparoscopy only and not comparing it with the 2D laparoscopic system.
Studies comparing 3D and 2D laparoscopic systems in nonurological surgeries.
Abstract articles for academic conferences without the full article.
Data extraction
Two reviewers performed data extraction and quality assessment of all the included studies. The following information was extracted from each included study: first author's name, publication year, 3D equipment system, surgical type, number of participants, age, gender, estimated blood loss (EBL), and operative time. We also extracted some specific clinical and surgical outcomes of interest from each surgical type. For instance, urethrovesical anastomosis (UVA) time, positive surgical margins (PSMs), continence recovery, and hospital stay data were extracted from the studies addressing radical prostatectomy (RP), while dissecting time, suturing time, and warm ischemia time (WIT) were obtained from articles reporting partial nephrectomy (PN) for comparison and meta-analysis. Finally, we divided all the included studies according to surgical type for a precise and accurate comparison.
Quality assessment
We used criteria provided by the Oxford Centre for Evidence-Based Medicine to rate the level of evidence for each study. The Newcastle–Ottawa Scale was used to assess the methodological quality of studies. Two reviewers performed the procedure, respectively. Disagreements were resolved through discussions. If disagreement persisted, a third investigator would participate in the discussion until a consensus was reached.
Statistical analysis
This meta-analysis compares the efficacy, safety, and overall clinical outcomes of 3D vs 2D laparoscopic systems for different urological surgeries. Review Manager software (RevMan v.5.3; Cochrane Collaboration, Oxford, United Kingdom) was used to analyze the studies in this meta-analysis for comparison. Odds ratio (OR) and mean difference (MD) were used to evaluate dichotomous and continuous variables, respectively. The statistical calculation reported by Hozo and colleagues 15 was used (when continuous data are reported as means and ranges) to calculate the standard deviation. Results are shown with 95% confidence interval (CI). Heterogeneity of the studies was assessed using the chi-square test. A p-value <0.05 was considered statistically significant.
Results
Study characteristics
Our literature search generated 17 studies (4 randomized and 13 observational) comparing 3D and 2D laparoscopic systems during different urological surgeries. 16 –32 These studies contained 630 and 520 patients who were operated on with 2D and 3D laparoscopic systems, respectively. Author's name, publication year, study design, study characteristics, and quality assessment of all the studies are summarized in Table 1. Of these, four studies 17,20,23,27 were excluded from the meta-analysis (one adrenalectomy study, one ureterolithotomy study, and one cystectomy study were excluded because there were no similar studies to compare with since we designed our study to compare studies addressing similar procedures, and the fourth study about pyeloplasty was excluded due to lack of a standard deviation parameter for meta-analysis comparison). The remaining 13 studies (3 randomized and 10 observational) containing 548 patients operated on with a 2D laparoscopic system and 449 patients operated on with a 3D laparoscopic system were divided into three groups according to surgical type. Meta-analysis results of these 13 studies are shown in Table 2. Viking 3D HD (United States of America), Karl Storz 3D (Germany), and Olympus 3D (Japan) were the 3D laparoscopic systems used in the studies we reviewed. Flow chart diagram illustrating our search and selection strategy is shown in Figure 1.
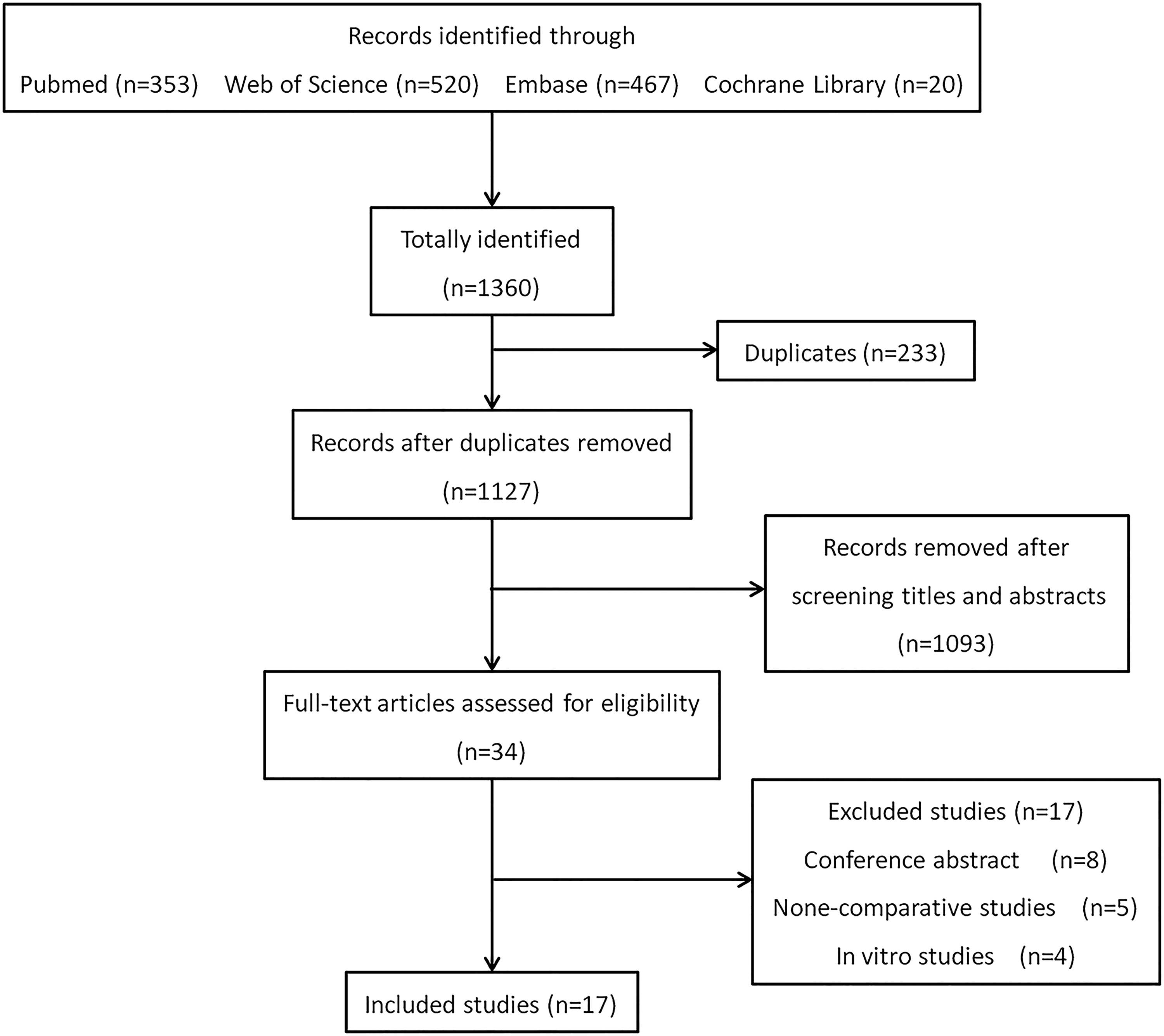
Flow chart of study search, inclusions, and exclusions.
Boldface indicates statistically significant values.
2D = two-dimensional; 3D = three-dimensional; M/F = male/female; SN = simple nephrectomy; RN = radical nephrectomy; PN = partial nephrectomy; NA = not available; — = not applicable; HD = high-definition; LTV = laparo-thoraco videoscope.
Boldface indicates statistically significant values.
WIT = warm ischemia time; UVA = urethrovesical anastomosis; MD = mean difference; OR = odds ratio; CI = confidence interval; EBL = estimated blood loss; PSM = positive surgical margin.
Quality assessment
The evidence levels of studies by Ruan and colleagues 25 and Kinoshita and colleagues 21 were rated Level 2, while the rest were Level 3 based on the Oxford level of evidence criteria. The studies by Aykan et al. 18 and Kinoshita and colleagues 21 were scored nine stars according to the Newcastle–Ottawa Scale, which was considered to be of high methodological quality. The remaining studies were scored eight stars each.
Meta-analysis
Partial nephrectomy
For PN, four studies comparing 2D and 3D laparoscopic systems comprising 193 vs 147 patients, respectively, were included. 22,25,26,32 Using a random effect model, results showed no statistical difference between the two groups on operative time (MD: 9.56; 95% CI: −4.60 to 23.73; p = 0.19), EBL (MD: −12.76; 95% CI: −50.56 to 25.04; p = 0.51), dissecting time (MD: 0.88; 95% CI: −4.02 to 2.25; p = 0.58), and suturing time (MD: 2.17; 95% CI: −2.19 to 7.16; p = 0.28). Warm ischemia time was significantly shorter in the 3D laparoscopic imaging system group compared with the 2D laparoscopic group (MD: 2.85; 95% CI: 1.85–3.86; p < 0.00001) (Fig. 2).

Forest plot and meta-analysis results of partial nephrectomy (2D vs 3D laparoscopy). 2D = two-dimensional; 3D = three-dimensional; M-H = Mantel–Haenszel; CI = confidence interval.
Pyeloplasty
Three studies 16,24,31 compared 2D and 3D laparoscopic systems during the pyeloplasty procedure (53 vs 45 patients, respectively). Of all the parameters reported in these studies, only operative time and EBL were comparable for meta-analysis. There was no significant difference between the two systems on both operative time and EBL (MD: 20.77; 95% CI: −24.82 to 66.35; p = 0.37 and MD: 10.88; 95% CI: −19.44 to 41.20; p = 0.48, respectively) (Fig. 3).

Forest plot and meta-analysis results of the pyeloplasty procedure (2D vs 3D laparoscopy).
Radical prostatectomy
Six studies 18,19,21,28 –30 compared 2D and 3D laparoscopic systems (containing 268 and 223 patients, respectively) during RPRP. Operative time and EBL revealed significant statistical differences between 2D and 3D laparoscopic imaging systems (MD: 42.85; 95% CI: 17.44–68.27; p < 0.0001 and MD: 78.38; 95% CI: 31.59–125.1; p = 0.001, respectively). Three-month postoperative continence recovery was significantly higher in the 3D laparoscopic radical prostatectomy (LRP) group than those operated on with 2D laparoscopy (OR: 0.40; 95% CI: 0.21–0.78; p = 0.007). UVA time, PSMs, and hospital stays showed no statistical difference in the analysis (MD: 18.23; 95% CI: −1.78 to 38.24; p = 0.07, OR: 1.57; 95% CI: 0.68–3.64; p = 0.29, and MD: 2.94; 95% CI: −2.20 to 8.90; p = 0.26, respectively) (Figs. 4 and 5).

Forest plot and meta-analysis results of radical prostatectomy (2D vs 3D laparoscopy).
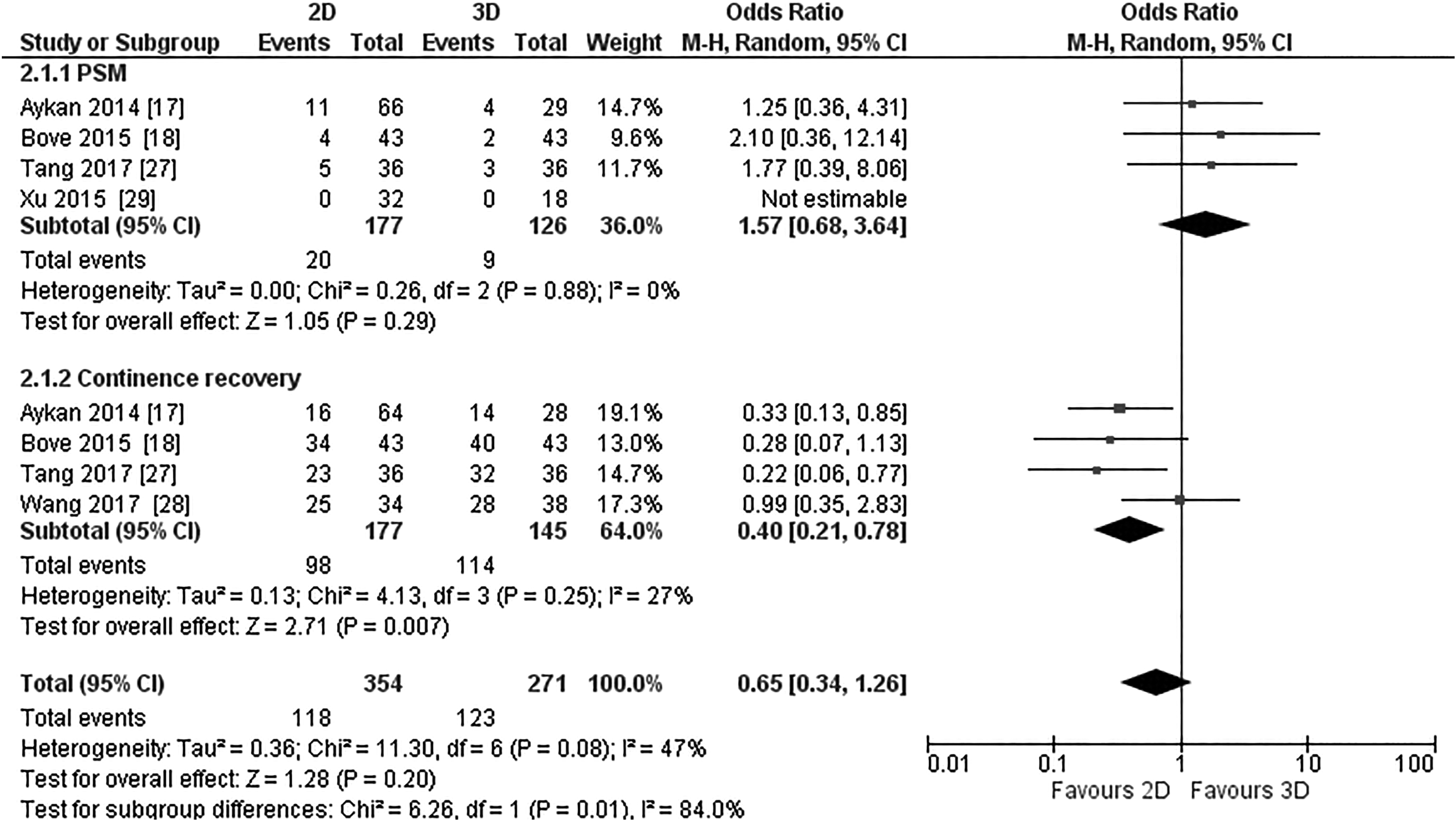
Forest plot and meta-analysis results of PSMs and continence recovery after radical prostatectomy (2D vs 3D laparoscopy). PSMs = positive surgical margins.
Discussion
Several clinical and nonclinical studies have shown higher advantages in the 3D laparoscopic system over conventional 2D laparoscopy. 5,9,33,34 Reduced performance time and lower precision errors favoring the 3D laparoscopic system are examples. 35,36 Despite the advantages, 3D laparoscopy is not widely adopted. According to some authors, higher cost to purchase the 3D system compared with the 2D system is the main reason for its lack of broad adaptation. 37 In contrast, Vettoretto and colleagues reported that adaption of the 3D system saves money for hospitals based on reduction in the operating time. 38 However, other investigators failed to find any significant difference between 2D and 3D laparoscopic surgeries concerning total surgical expenses. 27,28 On the other hand, discomfort, nausea, dizziness, and eye strains are among the reported limitations associated with the old generation of the 3D laparoscopic system. 39 However, the new 3D high-definition generations did not show any of the above limitations compared with the 2D laparoscopic system. 40
Urologists, in particular, showed special interest toward advances in 3D laparoscopic technology since most urological diseases can be managed with the assistance of laparoscopy. Many clinical studies compared 3D laparoscopy with the traditional 2D laparoscopic system during different urological surgeries to investigate the superiority claims favoring 3D laparoscopy. In this meta-analysis, data of 997 patients (548 vs 449 patients, 2D vs 3D laparoscopy, respectively) from 13 studies (3 randomized and 10 observational) were analyzed to evaluate the safety and efficacy of the 3D laparoscopic system compared with the 2D laparoscopic system.
Partial nephrectomy
In the past three decades, the role of PN in renal tumors has tremendously increased. Both European Association of Urology 2018 and American Urological Association 2017 guidelines on renal tumors strongly recommended PN as the standard treatment for localized T1 tumors. 41,42 Although open, laparoscopic, and robotic approaches were equally suggested, minimally invasive techniques (laparoscopy or robotics) are preferred for their lower morbidity. 42 Supporting these guidelines, a recent study with an extended follow-up period by Cai and colleagues 43 compared laparoscopic partial nephrectomy (LPN) with laparoscopic radical nephrectomy (LRN). In the above study, they found 85.56% vs 85.69% and 88.00% vs 82.85% of 10 years overall and cancer-specific survival rates after LPN and LRN, respectively. These results indicate that LPN is equally effective as LRN in terms of cancer control in addition to its nephron-sparing advantage.
LPN is one of the commonly performed urological surgeries today. Since several nonclinical studies reported shorter suturing time in the 3D laparoscopic system, we expected similar results in our meta-analysis. However, only WIT was significantly shorter during 3D laparoscopic surgery, while other parameters such as operative time, EBL, dissecting time, and suturing time were comparable between the 2D and 3D laparoscopic systems during PN.
On the other hand, we should keep in mind that there are other factors such as surgeon's experience, operative approach, and R.E.N.A.L nephrometry score (RNS) that can influence surgical and clinical outcomes during LPN. Different operative approaches have different perioperative outcomes; for instance, a meta-analysis study by Fan et al. 44 reported higher operative time and more extended hospital stays in transperitoneal LPN (TLPN) compared with retroperitoneal LPN (RLPN), while WIT and EBL were not statistically different between TLPN and RLPN. Of the four studies 22,25,26,32 in our meta-analysis, only Komatsuda and colleagues 22 approached their cases transperitoneally, while the other three authors reported a retroperitoneal approach.
According to some reports, higher RNS is associated with more extended WIT and higher conversion rates (to open) during LPN. 45 Nevertheless, two of the three studies in our meta-analysis reported results of RNS with no significant difference between the groups.
Pyeloplasty
Laparoscopic pyeloplasty is a widely accepted procedure for management of ureteropelvic junction obstruction. Both transperitoneal laparoscopic pyeloplasty (TLP) and retroperitoneal laparoscopic pyeloplasty (RLP) approaches are safe and effective. However, according to Singh et al., 46 higher operative time and intracorporeal suturing time were found in RLP compared with TLP. Another study found that mean drainage output (mL) was significantly more in continuous sutured TLP compared with interrupted sutured TLP. 47
In this study, we considered pyeloureteral intracorporeal suturing time as a crucial parameter. Unfortunately, none of the studies we reviewed have provided any data regarding this vital parameter for comparison. Two of the three studies 16,31 in our meta-analysis comparing 2D with 3D laparoscopic pyeloplasty showed significantly shorter operative time favoring the 3D laparoscopic system. However, our meta-analysis failed to show any significant difference between 2D and 3D laparoscopic pyeloplasty concerning operative time and EBL.
Radical prostatectomy
Prostate cancer is the second most diagnosed cancer in men after lung cancer. 48 Perhaps this is due to the increase in human life expectancy (since prostate cancer is an age-related disease) and the extensive use of screening programs containing prostate-specific antigen examination and high-quality imaging techniques. Although open radical prostatectomy (ORP) is still the golden approach, almost all medium- to large-sized urological centers around the world are well adapted with LRP or robot-assisted radical prostatectomy (RARP) techniques for their lower morbidity. Irrespective of the method used during RP, five common goals should be achieved after the surgery, the so-called pentafecta (no evidence of PSMs, no early complications, sexual and continence recovery, and free from biochemical recurrence). 49 A newly published review article by Basiri et al. 2 reported higher PSM and complication rates in ORP than in RARP. In the same study, operative time, length of hospital stay, EBL, and transfusion rates were significantly lower in LRP than in ORP.
RP is a complex and delicate procedure that requires detailed anatomical understanding, especially when dealing with young patients with localized tumors, for better oncological and functional outcomes. For this reason, many centers around the world use the da Vinci robotic system for its excellent 3D vision and hand-like EndoWrist instrument. According to the Intuitive Surgical, Inc., 2016 annual report, over 162,000 RARP procedures were performed during 2016 alone. 50 Nevertheless, the use of the da Vinci robotic machine costs much money for both patients and healthcare providers. 2 Therefore, advances in traditional laparoscopy such as 3D technology and robotized laparoscopic instruments are essential for their lower cost compared with da Vinci robotics.
The operative time and EBL were significantly shorter in 3D LRP than in 2D laparoscopy in our meta-analysis, while PSMs and length of hospital stay were similar between the two groups. On the other hand, we might all agree that UVA during LRP requires complex maneuvers to accomplish leak-free anastomosis. The angle at which the anastomosis should be performed plus the limited motion of laparoscopic instruments makes UVA the most challenging step in the whole procedure. Of the four studies that reported UVA time, three of them 18,19,29 found significantly higher UVA time in 2D laparoscopy compared with the 3D laparoscopic system. Nevertheless, this meta-analysis did not notice any statistical significance between the 2D and 3D laparoscopic systems regarding UVA time (p = 0.07). Similarly, PSM rates were not significantly different between the two groups. In contrast, 3-month postprostatectomy continence recovery was higher in the 3D laparoscopic group (p = 0.007), perhaps the 3D laparoscopic imaging system improves visibility to allow preservation of important structures for faster continence recovery.
Sexual recovery after RP is another vital surgical outcome. Only two studies reported potency recovery outcomes in which results were conflicting. Bove and colleagues 19 reported similar potency outcomes (58% vs 63% in 2D and 3D laparoscopy, respectively) after bilateral nerve-sparing surgery. On the other hand, Tang et al. 28 found significantly faster sexual recovery in 3D LRP than in the 2D operated group (41.67% vs 25% and 58.33% vs 41.67% after 3 and 6 months, respectively).
The small data sample in our meta-analysis and shortcomings of observational studies are the two main limitations of our study; these two together may prevent an absolute conclusion.
Conclusion
Although the data sample is small for a concrete and conclusive argument, based on the above findings in our meta-analysis, the 3D laparoscopic imaging system seems to provide better clinical and surgical outcomes in some urological procedures compared with conventional 2D laparoscopy. Three-dimensional laparoscopy mainly improves the depth of perception for better visibility, which is important for complex urological surgeries such as PN, pyeloplasty, and RP. Future well-designed, randomized clinical studies comparing 2D and 3D laparoscopic systems are recommended to validate our findings.
Footnotes
Acknowledgment
The authors are grateful to Dr. Musa Male for grammatical corrections in the manuscript.
Author Disclosure Statement
No competing financial interests exist.