
Abstract
Introduction:
Staging of upper tract urothelial carcinoma (UTUC) remains a dilemma due to imaging and biopsy limitations leading to understaging. We seek to determine the accuracy of endoluminal ultrasound (ELUS) for clinical staging of UTUC.
Materials and Methods:
Patients evaluated for UTUC underwent retrograde pyelography, ureteroscopy, and ELUS. ELUS was performed using mechanical radial scanning at 20 MHz in B-mode with a 5F probe. Cine clips were evaluated by 2 radiologists blinded to ureteroscopic and pathology findings. Results were compared to pathology from nephroureterectomy. Inclusion criteria were patients who underwent nephroureterectomy without pretreatment or managed endoscopically for cTa-1 disease and were without recurrence for >1 year.
Results:
From 2008 to 2013, 53 patients underwent ELUS without complication. Twenty-seven patients met inclusion criteria with conclusive ELUS imaging. ELUS accurately identified 16 of 21 patients with non-muscle invasive (MI) disease (18 pTa, 2 pT1, 1 CIS) and 1 of 6 patients with at least MI disease (2 pT2, 4 pT3). For MI disease, the positive predictive value (PPV), negative predictive value, and accuracy was 76.2%, 16.7%, and 63%, respectively, while for non-organ confined (OC) disease results were 0%, 81.8%, and 66.7%, respectively.
Conclusions:
With current technique and instrumentation, ELUS may prove useful in select cases to confirm findings of non-MI and OC disease. However, it has insufficient PPV for stage pT2-3 disease. Further studies and better instrumentation are needed before incorporation into clinical practice.
Introduction
T
We have previously performed a pilot study to investigate the utility of ELUS with respect to diagnostic accuracy in UTUC. 8 In that pilot study, 6 of 7 patients had accurate ELUS staging when correlated with the pathologic findings. The pilot study was limited by the small number of patients and absence of blinded evaluation. We report an expanded study further evaluating ELUS to determine if this modality can accurately stage patients with untreated UTUC based on assessment by evaluators blinded to ureteroscopic and pathologic findings.
Materials and Methods
This was an Institutional Review Board approved retrospective protocol. ELUS was performed by mechanical radial scanning at 20 MHz using a 1.7-mm (about 5F) diameter probe (UMG2029R3; Olympus Corp America, Orangeburg, NY) in B mode. This probe allows for placement over a guidewire, and it has a shielded, continuously rotating transducer that provides radial images, with adjustable scanning depths of 2–12 cm (Fig. 1). Due to absence of tissue penetration beyond 4 cm at such high frequencies and the small anatomy of the upper urinary tract, ranges of 2–4 cm were utilized.

ELUS equipment and probe. The ELUS keyboard is covered in sterile plastic to allow handling by the surgeon. The probe tip has a clear wire guide and housing for the rotating transducer. Rotation is afforded by a motor attached to the other end of the probe (arrow). ELUS = endoluminal ultrasound.
Retrograde pyelography and ureteroscopy were performed by the senior author to evaluate for additional filling defects or otherwise identifiable tumors and then correlated to the fluoroscopic images. The ureteroscope was withdrawn, and the ELUS probe passed over a guidewire under fluoroscopy to the previously fluoroscopically-correlated location(s) of interest. The sonographic image gain and contrast were adjusted to produce an anechoic signal for the surrounding fluid for optimal image acquisition. The imaging depth of field was also adjusted to obtain optimal viewing and resolution, usually at 2–4 cm (Figs. 2 and 3). Cine clips and images which included notation of the laterality and general location of the tumor were saved; if multiple tumors were present, all were attempted to be documented with notation made of the index (largest) tumor. After ELUS was performed, the probe was removed and further treatment was carried out, including endoscopic biopsy and ureteral stent placement.

Series of images from a case depicting filling defect on retrograde pyelography
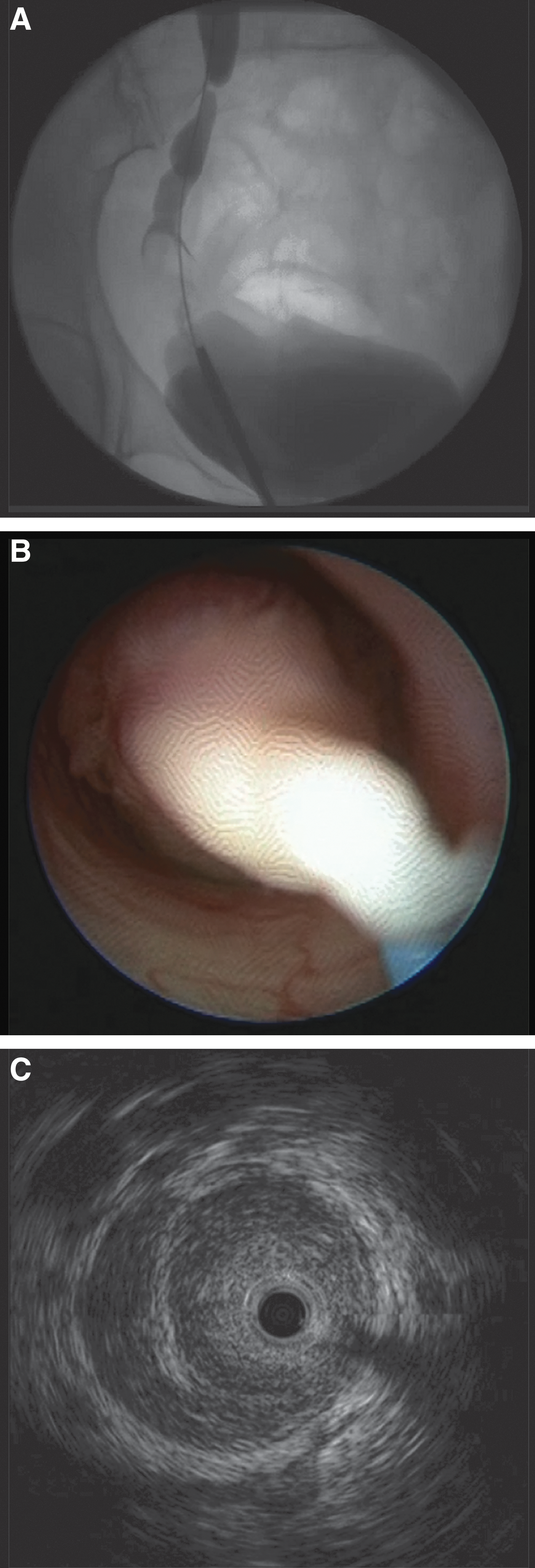
Series of images from a case depicting a larger tumor, again seen on retrograde pyelography
Two radiologists with expertise in ultrasound and having previously reviewed training ELUS cases interpreted the sonographic images and cine clips; both were blinded to the endoscopic and pathologic findings. Standard landmarks such as the iliac vessels, psoas muscle, and the renal vessels in the pelvis were used for orientation, as well as correlation with retrograde images and annotations on the images. Disagreements between the two blinded evaluations were resolved by consensus discussion. Any circumferential or eccentric thickening in the ureter was noted. The integrity of the sonographically identifiable outer ureteral or renal pelvic layer (interface between muscularis and retroperitoneal fat, renal vein, or renal parenchyma) was used to determine the depth of invasion when possible. Non-organ confined (OC) disease was defined by tumor penetrating through the muscularis or extending into the surrounding soft tissue. In addition, the location and size of the lesions were recorded.
Patients undergoing definitive surgery without neoadjuvant chemotherapy or those who were managed endoscopically for cTa-1 disease and who were without sign of recurrence or progression for a minimum of 1 year, underwent correlation of pathology findings to ELUS findings. The ability of ELUS to predict muscle invasive (MI) and non-OC disease was determined using Fisher's test for association and significance, as well as standard sensitivity, specificity, and predictive value analysis.
Results
From September 2008 to September 2013, a total of 53 patients underwent ELUS. No complications occurred as a result of the ELUS procedure. Ten patients underwent neoadjuvant chemotherapy before nephroureterectomy and were excluded from the analysis. Eleven patients did not undergo surgery due to metastatic disease and did not have final pathology for correlation. Five patients had uninterpretable images, either due to large size or location distant from the ELUS probe (lower caliceal tumors). After these exclusion criteria, 27 patients were eligible. Median time between ELUS and nephroureterectomy was 30 days.
Table 1 shows clinical, ureteroscopic, ELUS, and pathologic characteristics, and Tables 2 and 3 show the correlation of sonographic and pathologic findings. Nineteen patients were found to have pTa disease, and ELUS accurately staged 14 of these. Of the five ELUS-overstaged pTa patients, two were read on ELUS as ultrasound (u)T1 and three as uT3. Four patients were found to have pT3 disease, and ELUS understaged three of them as uTa and one as uT2.
P
ELUS = endoluminal ultrasound.
ELUS accurately identified 16 of 21 patients with non-MI disease and 1 of 6 patients with MI or higher disease. ELUS accurately identified 18 of 22 patients with OC disease and 0 of 4 patients with non-OC disease. Overall ELUS understaged 6 (22.2%) and overstaged 7 (25.9%) patients. The positive predictive value (PPV) for <pT2 (non-MI) and ≤pT3 (OC) disease was 76.2% and 78.3%, respectively, but for MI and non-OC disease, PPV was 16.7% and 0. Accuracy for MI disease was 63.0% and for non-OC disease was 66.7% (Tables 2 and 3).
Discussion
This study demonstrates that ELUS appears to be best at confirming non-MI and OC disease, while it may not adequately confirm MI and non-OC disease. These results may be explained by technical factors, some previously discussed, as well as study limitations. 3,8 Optimal images are obtained with a surrounding column of fluid around the probe, thus imaging in the mid and proximal ureter and renal pelvis are usually most ideal, while distal ureter tumors may not be assessed as well due to the narrower ureter in this area and inability to instill saline during ELUS (Fig. 4). The probe is passed over a wire and is not deflectable, thus lower pole and interpolar calix tumors may not be well visualized. Most lesions are isoechoic, or of slightly lower echogenicity, to the intermediate muscle layer, and thus, muscle invasion may not be confidently performed. As noted above, presence of fluid within the renal pelvis helps identification of the three distinct layers of the upper tract collecting system on high frequency ultrasound. Pedunculated tumors can be sonographically diagnosed in a distended system when a stalk and its attachment can be seen. With larger tumors bulging the ureteral wall outward, diagnosis of invasion can be challenging. Visualization of the three distinct layers in the ureter should offer capabilities to accurately assess the depth of invasion of tumor similar to its application in various gastrointestinal malignancies, 9,10 but this would require a higher frequency and larger probe, none of which to our knowledge are currently available for safe use in the upper urinary tract. With improvements in these areas, the results of ELUS for staging of UTUC may improve. Limitations leading to these results may also relate to the relatively small number of patients with MI and non-OC disease. Other limitations include retrospective study design; we tried to minimize this bias by keeping the study radiologists blinded as to the ultrasound and pathologic findings and only providing cine clips from the ELUS evaluation and retrograde pyelography images. An additional limitation that affects the sample size is the attrition of patients due to receipt of neoadjuvant chemotherapy and lower pole tumors which were not seen well on ELUS. Five of the 10 patients excluded for having received neoadjuvant chemotherapy were read as having invasive disease, accounting for nearly half of the MI ELUS reads. These patients are at an increased suspicion of invasive disease yet their ELUS reads are excluded by the study design as potential downstaging may have confounded results.

Series of ELUS images:
Current conventional methods for staging rely on ureteroscopy and cross-sectional imaging, typically with CT. Both, however, have significant limitations. Ureteroscopy is usually unable, if not unsafe for risk of perforation, to obtain muscle in the specimen for assessment of invasion; thus ureteral staging is usually limited to clinical classification as Tx (unable to assess invasion), Ta, T1, or Tis. However, other findings such as sessile architecture and biopsy high grade are strongly associated, but not confirmatory, for invasive disease. 11,12 CT can reliably demonstrate clear-cut cases of infiltration into the renal parenchyma, but does not have the spatial resolution to demonstrate the thin muscularis of the ureter and renal pelvis, although it can provide secondary signs of locally advanced disease, such as hydronephrosis, or periureteral stranding 13 ; these are also associated, but not confirmatory, for invasive disease.
ELUS has seen development and success in staging of gastrointestinal malignancies. 9,10,14 Endovascular applications have also been investigated. 15 Despite the development of ELUS in these areas, as well as other urologic applications, 14 –16 there are limited data available regarding the use of ELUS with UTUC. Prior urologic studies are primarily aimed at ureteropelvic junction obstruction and the evaluation of extraluminal vessels. 17 Upper urinary tract neoplasms have been evaluated; however, only two patients from another study were confirmed by final pathology on nephroureterectomy. 3 Further experience with use of ELUS in the urinary tract was reported, including one patient with UTUC. 4 ELUS has been evaluated for urothelial carcinoma of the bladder with some documented success in diagnosis of invasion. 18 The same group would later correlate bladder wall layers with ELUS in an animal study using a higher frequency 30 MHz probe. 19 There have been prior novel studies published with subsequent literature reviews regarding three-dimensional ELUS; however, none of these include pathologic correlation of imaging findings. 16,20
Of additional interest in the area of clinical risk stratification for UTUC are two other technologies in evaluation. Confocal laser endomicroscopy (CLE) use for UTUC was first explored by the group from Stanford. Bui and colleagues 21 reported an initial feasibility study in 14 patients, showing that the technology had no adverse events, and allowed imaging the tumor and anatomy. Breda and colleagues 22 recently evaluated ability for CLE to perform histologic grading of 14 patients, showing agreement with pathologic review of specimens in 7/7 low grade tumors, 5/6 high grade tumors, and 1/1 with carcinoma in situ. Another promising technology involves use of optical coherence tomography (OCT), with the most extensive work performed from the group from Amsterdam. Bus and colleagues 23 reported the diagnostic accuracy of OCT in staging and grading of 26 patients with UTUC undergoing surgical resection. OCT had sensitivity and specificity of 100% and 92%. False positive results were seen for tumors >2 mm and presence of inflammation. Further evaluation from both technologies is eagerly awaited, but at this time all three require further studies before dissemination into clinical practice.
Conclusions
ELUS may prove useful in select cases to confirm findings of non-MI and OC disease, especially if endoscopic management is being considered as it can provide additional confidence for this approach. However, improvement of current instrumentation is needed, possibly with use of a larger, higher resolution probe, before recommending its routine use to confirm MI or non-OC disease.
Footnotes
Acknowledgments
The authors thank Catherine Hiatt, Eugene Familiar, Robin Bragg, and Darryl Rigby for their assistance with ELUS equipment management and Maiden Suire with article preparation.
Author Disclosure Statement
Supported, in part, by the Monteleone Family Foundation for Research in Kidney and Bladder Cancer and the Eleanor and Scott Petty Fund for UTUC Research. None of these sponsors played any part in the study.