
Abstract
Background:
Cystoscopy is a safe diagnostic procedure commonly used to evaluate lower urinary tract symptoms. This can cause pain, anxiety, and dissatisfaction in patients undergoing cystoscopy.
Objectives:
The aim of this study was to compare the effects on pain, anxiety, and satisfaction of distraction methods used during cystoscopy.
Design:
Single-center, open-label, randomized, parallel-group trial.
Setting:
Cystoscopy unit of a training and research hospital in Turkey.
Participants:
Male patients ≥18 years of age who underwent rigid cystoscopy for the first time.
Methods:
A total of 120 male patients were recruited and randomized into four groups as music, stress ball, video, and control group. Data were collected using visual analog scale for pain and satisfaction, State-Trait Anxiety Inventory for anxiety, and hemodynamic parameters. The primary outcome was the difference with respect to pain scores among intervention groups. Other outcome measures were anxiety and satisfaction scores.
Results:
Pain severity during cystoscopy was found to be significantly lower in the intervention groups than the control group. In the video group, the severity of pain during cystoscopy was also found to be significantly lower than music and stress ball groups (p = 0.006, p < 0.001). After cystoscopy, anxiety levels were significantly lower and satisfaction levels were significantly higher in the intervention groups than in the control group. Anxiety levels were significantly lower in the video group than music and stress ball groups (p < 0.001, p < 0.001). Satisfaction levels were also significantly higher after cystoscopy in the video group than in the music and stress ball groups (p = 0.018, p = 0.018).
Conclusions:
According to this study, distraction methods used during rigid cystoscopy were found to have a reducing effect on pain, anxiety, and dissatisfaction. As the results of the study are evaluated, video should be recommended to be the first preferred distraction method during rigid cystoscopy.
Introduction
C
Patients may experience fear, anxiety, and pain when a cystoscope is placed into the urethra or during the procedure. 6 –8 In cases when a patient is extremely anxious, cystoscopy can be performed under general anesthesia to ensure that the patient is quiet and calm during the procedure. 9 The procedure is more painful for men than women. 10 –12 In men, most pain occurs during the cystoscope's passage through the membranous urethra, the shortest and narrow segment of the urethra. 2,13,14
Distraction methods provide ways for patients to relax during surgical procedures. 15 These methods allow refocusing the patient's consciousness by drawing attention from pain to a more pleasing sensation. 15,16 There are several randomized controlled studies that have shown that any simple distraction method could be individually used to decrease pain and anxiety during cystoscopy. 6,9,12,17,18 Although there are a few studies comparing the effectiveness of multiple simple distraction methods such as music, stress ball, or video on pain and anxiety during painful procedures, 15,19 there are no studies in the literature that compare the effects of different distraction methods used during cystoscopy. The aim of this study was to compare three distraction methods (music, stress ball, and video) with regard to their effects on pain, anxiety, and satisfaction levels relative to standard treatment during rigid cystoscopy.
Methods
Design and setting
This study was a single-center, open-label, randomized, parallel-group trial. The study was carried out in the Cystoscopy Unit of Department of Urology of a Training and Research Hospital, in Ankara, Turkey between March 2016 and March 2017. Research nurse carried out the eligibility screening when the patient applied to the cystoscopy unit.
Eligibility criteria
Participants who met the following inclusion criteria were eligible for the study: (1) age ≥18 years, (2) male gender, and (3) rigid cystoscopy for the first time. Exclusion criteria consisted of several parameters: (1) presence of any contraindication for cystoscopy (such as lidocaine allergy, urinary tract infection, and urethra-related anatomical disorders); (2) any analgesic used 24 hours before cystoscopy; and/or (3) manipulations such as Double-J stent placement or removal, and/or bladder biopsy.
Interventions
The study was divided into three stages: (1) before, (2) during, and (3) after cystoscopy. Patient's hemodynamic parameters, including systolic and diastolic blood pressures, heart rate, and oxygen saturation, were measured about 5–10 minutes before, during (when the cystoscope was placed into the urethra), and within 10 minutes after the cystoscopy procedure was complete.
All the patients who participated in the study underwent the standard protocol used in the Cystoscopy Unit of our institution. This standard care protocol followed several steps: Before the cystoscopy procedure, once explanatory information was given to a patient by a research nurse and a surgical technician, who work in the cystoscopy unit, the patient was laid on his back on the cystoscopy table in a lithotomy position. The patient was asked to put his legs on two metal stirrups and bend the knees. The area to be treated was covered with sterile cover. After the patient's penis was cleansed with povidone iodine, 2% lidocaine gel 10 mL was instilled into the urethra and left there for 15 minutes. A 19F rigid cystoscope was used for all patients. Cystoscopy was performed by a specialist and a surgical technician. During the procedure, the patient was not given any analgesic drug. After the procedure, an intramuscular first-generation cephalosporin antibiotic (1 g) was prophylactically administered to the patients.
The patients who met the inclusion criteria were assigned to one of the four groups: (1) music, (2) stress ball, (3) video, or (4) control group. The music group listened to music of their choice with a headset from an MP3 player starting at ∼10–15 minutes before cystoscopy until completion of the procedure. These music types included Turkish folk music, Turkish art music, Turkish arabesque music, Turkish pop music, foreign pop music, rock music, and/or classical music. The stress ball group was given stress balls in both palms ∼10–15 minutes before cystoscopy. The patients in stress ball group were instructed to “squeeze the balls twice after counting up to five” and “repeat until the end of the entire procedure.” This ball was medium hard and made of high-quality silicon. The video group watched the video of their choice from a ceiling-mounted television starting at ∼10–15 minutes before cystoscopy until the procedure was completed. These video types consisted of nature, Guinness records, adrenaline-filled action videos, soccer, comedy, and camera jokes. The control group received the standard treatment from a surgical technician who works in the cystoscopy unit starting before cystoscopy until the end of the procedure. The patients in the control group were given information about the procedure similar to the other groups.
Sample size
The sample size for recruitment was calculated to be at least 92 patients (at least 23 patients per group) for 5% and 20% alpha and beta errors, respectively, (
Randomization and allocation
Block randomization was used to allocate subjects into four equal-sized groups as previously described. Eligible patients were randomly assigned to one of the four groups according to a computer-based block randomization list generated by an advisory biostatistician in our institution. Although participants and researchers were not blinded to group allocation, the biostatistician remained blinded.
Outcome measures
In the study, outcome measures were obtained using the VAS for pain and satisfaction and State-Trait Anxiety Inventory (STAI) for anxiety. Research nurse asked the participants to rate their pain, anxiety, and satisfaction levels.
The primary outcome was the difference among intervention groups with respect to pain intensity based on the VAS as reported by the participants at the end of cystoscopy compared with baseline. The VAS is an unidimensional measure commonly used to measure pain intensity. The VAS is a measuring tool with length of 0–10 cm (0–100 mm). High scores on the scale indicate that pain intensity is high. 20 In this study, pain assessment was performed before, during, and after cystoscopy.
The secondary outcomes were the differences among intervention groups with respect to anxiety levels using the STAI at the end of the cystoscopic procedure compared with the baseline and on satisfaction level based on the VAS as reported by the participants at the end of cystoscopy. STAI was developed by Spielberger and colleagues in 1970 to measure anxiety. 21 The Turkish adaptation of the scale was performed by Öner and Le Compte in 1985. 22 The scores on the scale ranges from 20 to 80. The high scores on the scale indicate that anxiety is high. Anxiety assessment was performed before and after cystoscopy. Satisfaction assessment was also performed immediately after cystoscopy. The high scores obtained from the VAS demonstrate that satisfaction level was high.
Statistical methods
The Statistical Package of the Social Sciences (SPSS) 22.0 was used for the data analysis (SPSS, Inc., Chicago, IL). Number, percentages, means, standard deviations, medians, and minimum and maximum values were used for descriptive statistics of the study. The Shapiro–Wilk test was used to indicate whether data were normally distributed. The chi-squared test was used for statistical comparison of the descriptive data. The Kruskal–Wallis test was used to compare difference among four groups with non-normal distribution, whereas analysis of variance was used to compare difference among four groups with normal distribution.
Ethical considerations
This study was conducted after approval from the Ethics Committee of our institution in Ankara, Turkey (No: 50687469-1491-263-16/1648-736) was obtained and registered with
Results
Participants
Participants were recruited between March 2016 and March 2017 in the cystoscopy unit. A total of 435 patients were evaluated for eligibility, and 315 patients were excluded from the study. A total of 254 patients were excluded from the study because they did not meet the inclusion criteria and another 61 patients were also excluded for other reasons. A total of 120 patients were included in the study and they were randomly assigned into four groups (30 patients per group). No patient dropped out of the study, and all 120 patients completed the study (Fig. 1). Sociodemographic characteristics are given in Table 1.
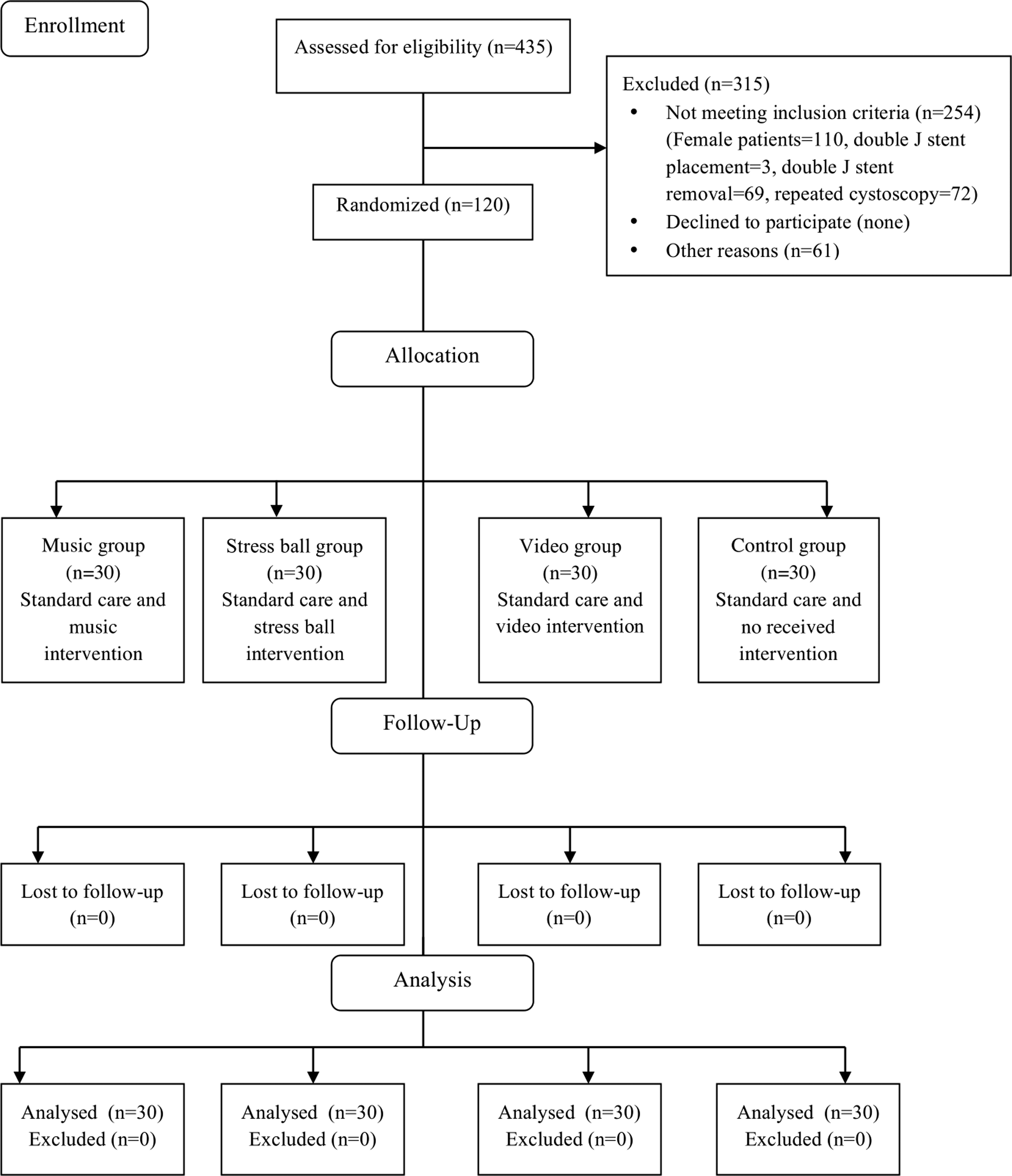
Flowchart of the study. The flowchart was divided into stages: enrollment, allocation, follow-up, and analysis.
Kruskal–Wallis test.
One-way analysis of variance test.
Chi-square test.
BMI = body mass index.
Outcomes
The comparison of VAS pain scores among groups of participants in the study is given in Table 2. Pain intensity during cystoscopy was significantly lower in the intervention groups (p < 0.001) than in the control group. Pain intensity during the procedure was significantly lower in the video group than in the music and stress ball groups (p = 0.006 and p < 0.001, respectively).
Kruskal–Wallis test.
Music group–control group.
Stress ball group–control group.
Video group–control group.
Music group–stress ball group.
Music group–video group.
Stress ball group–video group.
Bold values indicate statistical significance (p < .05).
VAS = visual analog scale.
The comparison of STAI cores among the four groups of participants in the study is given in Table 3. After cystoscopy, participants' anxiety levels were significantly lower in intervention groups (p < 0.001) than in the control group. After the procedure, anxiety levels were significantly lower in the video group than in the music and stress ball groups (p < 0.001 for both groups).
Kruskal–Wallis test.
STAI difference: before cystoscopy − after cystoscopy anxiety scores difference.
Music group–control group.
Stress ball group–control group.
Video group–control group.
Music group–stress ball group.
Music group–video group.
Stress ball group–video group.
Bold values indicate statistical significance (p < .05).
STAI = State-Trait Anxiety Inventory.
The comparison of VAS satisfaction scores among the groups of study participants is given in Table 4. After cystoscopy, satisfaction levels were significantly higher in intervention groups (p < 0.001) than in the control group. After the procedure, satisfaction levels were significantly higher in the video group than in the music and stress ball groups (p = 0.018, p = 0.018 for both groups).
Kruskal–Wallis test.
Music group–control group.
Stress ball group–control group.
Video group-control group.
Music group–stress ball group.
Music group–video group.
Stress ball group–video group.
Bold values indicate statistical significance (p < .05).
The comparison of hemodynamic parameters measured during cystoscopy among the four groups is given in Table 5. Systolic and diastolic blood pressures during cystoscopy were significantly lower in the intervention groups (p < 0.05) than in the control group. Heart rates during cystoscopy were significantly lower in the stress ball and video groups (p = 0.048 and p = 0.005, respectively) than in the control group.
Kruskal–Wallis test.
One-way analysis of variance.
Music group–control group.
Stress ball group–control group.
Video group–control group.
Music group–stress ball group.
Music group–video group.
Stress ball group–video group.
Bold values indicate statistical significance (p < .05).
Discussion
In this study, the effects on pain, anxiety, and satisfaction levels of three different distraction methods used during cystoscopy were examined. As a result of literature review on distraction methods, there was no study in which these methods were used in combination during cystoscopy. However, there was only one study comparing the effect of multiple distraction methods (music, DVD, interaction, stress ball) on level of pain, anxiety, and satisfaction during vascular surgery. 15 In three different studies investigating the effects of music on pain and anxiety in patients who underwent cystoscopy, it was found that the music played during the procedure produced a relaxing effect on the severity of pain. 6,12,17 According to this study, distraction methods were found to be effective in reducing pain during and after cystoscopy; however, video was found to be more effective for pain relief than the others. The reason for video being more effective for pain relief could be the result of engaging more than one sense organ (audiovisual).
Cystoscopy can cause anxiety and fear in patients. 6 Several studies have demonstrated that music significantly decreased anxiety after the procedure compared with the control group. 6,12,17 In this study, distraction methods used during cystoscopy were found to be more effective for anxiety reduction. Video was found to be the most effective method for anxiety relief. This may be because the video method engages multiple senses, both visual and auditory.
In the study by Yeo and colleagues, music listened during cystoscopy was found to increase patients' satisfaction levels after the procedure. 6 In this study, distraction methods used during cystoscopy were found to be effective for improving patient satisfaction. However, video was found to be a more effective method for patient satisfaction than the others.
Cystoscopy may cause changes in patients' hemodynamic parameters in addition to pain and anxiety levels. 6 Pain and anxiety are perceived as a stressor by the body and can cause some harmful effects (increases in heart rates, increases in systolic and diastolic blood pressures, and increases in respiratory rates) on the system. 23 Several studies have shown that music is effective for stabilizing hemodynamic parameters. 6,12 In the study by Yeo and colleagues, there was a significant difference between music and control groups after cystoscopy in terms of heart rate and systolic blood pressure. 6 In another study, there was a significant difference between music and control groups in terms of heart rates after cystoscopy, and heart rates were found to be lower in the music group. 12 As a result of this study, distraction methods were found to have a reducing/shooting effect on systolic and diastolic blood pressures measured during cystoscopy. Stress ball and video methods were found to reduce heart rates during the procedure.
Conclusion
In conclusion, the distraction methods could provide a cost-efficient method for improving rigid cystoscopy tolerability. This study provides evidence that the music, stress ball, and video methods used during rigid cystoscopy produce reducing/shooting effects on pain and anxiety and also have a positive effect on hemodynamic parameters and patient satisfaction. According to this study, video should be recommended to be the first preferred distraction method during rigid cystoscopy.
Limitations
There were some limitations to this study. First, it was not possible to blind the researcher to group allocation because of study design and the nature of each intervention. Second, it was difficult to objectively evaluate pain because it is subjective, and pain sense can differ from individual to individual. Third, the applicability of this study to centers that utilize flexible cystoscopy may be limited. Finally, the results of this study cannot be generalized to women because the study sample consisted of male patients only.
Footnotes
Acknowledgments
We thank all the patients who participated in the study, and the nurses and doctors who work in the research clinic for their supports.
This study was not supported by any funding agency in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
The authors have not declared any conflict of interest.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.