
Abstract
Introduction:
Percutaneous nephrolithotomy (PCNL) is the gold standard treatment for upper tract stone burdens greater than 2 cm. Metabolic syndrome (MetS) is a constellation of conditions (diabetes mellitus, hypertension, dyslipidemia, and obesity) and is a risk factor for nephrolithiasis. Our objective was to investigate adverse cardiovascular outcomes of PCNL in patients with comorbid MetS diagnoses.
Materials and Methods:
Data from the Healthcare Cost and Utilization Project State Inpatient Database for Florida and California were used to identify PCNL patients (ICD9: 55.03, 55.04) between 2007 and 2011. Patients were categorized having 0, 1–2, or 3–4 components of MetS. Postoperative myocardial infarction (MI) and inhospital mortality rate outcomes were identified. Multivariate logistic regression was used to control for patient characteristics (age, race, and primary insurance provider) and medical comorbidities.
Results:
PCNL was performed on 39,868 patients, of whom 17,932 (45.0%) had no MetS conditions, 19,268 (48.3%) had 1–2 MetS conditions, and 2668 (6.7%) had 3–4 MetS conditions. With increasing MetS conditions, patients had increased incidence of postoperative MI (0: 0.6%; 1–2: 1.0%; 3–4: 1.8%, p < 0.001). On multivariate analysis, the presence of 3–4 MetS comorbidities increased the odds of a postoperative MI (1–2: odds ratio [OR] 1.2, 95% confidence interval [CI] 0.94–1.53, p = 0.147; 3–4: OR 2.2, 95% CI 1.54–3.15, p < 0.001).
Conclusions:
MetS patients have an increased risk of MI following PCNL given their pre-existing comorbidities. Routine preoperative cardiac testing may benefit this population before PCNL.
Introduction
I
Numerous studies have implicated components of the metabolic syndrome (MetS) as risk factors for nephrolithiasis. 2 The MetS is a constellation of cardiovascular risk factors that include diabetes, hypertension, dyslipidemia, and obesity (defined as body mass index [BMI] >30 kg/m2). MetS affects up to 33% of the U.S. adult population. 3 Previous reports have found that nearly 10% of patients undergoing PCNL have MetS. 4 Specifically related to PCNL, retrospective studies have shown increased hospital stay and blood loss in patients with MetS. 5 Tefekli and colleagues detected a risk of major complications after PCNL (including hemorrhage necessitating blood transfusion, adjacent organ injuries, and severe infections) to be higher in patients with hypertension, diabetes, or MetS. 4 Other studies that evaluated long-term outcomes following PCNL have shown an increased stone recurrence rate and worse long-term renal function in patients with MetS compared with those without. 6 Many of these past studies contain small cohorts of subjects and do not assess cardiovascular complications. In all surgical patients, those who have components of the MetS have been shown to have an increased risk of postoperative complications and morbidity. 4 However, cardiovascular complications during or after PCNL have not been assessed in this cohort of patients.
No previous studies have determined if patients with components of MetS have an increased risk of cardiovascular complications, specifically myocardial infarction (MI), after PCNL. It is widely accepted that MetS is associated with an increased risk of ischemic cardiovascular events, however, it is controversial whether or not MetS is a greater predictive factor than BMI for MIs. 7 With our interest in PCNL outcomes, our objective was to use a large population-based database to investigate perioperative outcomes, specifically postoperative MI after PCNL, in patients with comorbid MetS diagnoses. This will help improve risk stratification for cardiovascular optimization before PCNL.
Materials and Methods
A cross-sectional, retrospective review of patients was conducted using The Healthcare Cost and Utilization Project State Inpatient Database (HCUP SID) for Florida and California. We identified PCNL cases using the International Classification of Diseases, Version 9, Clinical Modification (ICD-9-CM) procedure codes 55.03 and 55.04 between the years 2007–2011. The HCUP provides inpatient hospitalization records for all payers in a deidentified, publicly available database. Patient demographic information, as well as acute and chronic medical diagnoses, is provided based on administrative discharge records. 8 The HCUP SID is organized using uniform formatting, allowing for use of HCUP tools and software to facilitate clinical research. A total of 17 states include variables to track sequential visits for an individual patient over time within the state. The consistency of encrypted person identifiers is measured by HCUP and varies by state. The states of California and Florida each have notably high reliability (88.3% and 96.0%). 9 Beginning in 2007, diagnoses could be labeled as “present on admission,” allowing preexisting conditions to be identified and differentiated from those arising during hospitalization. 8 Also, a unique linkage variable is assigned to individual patients in each SID, allowing for the longitudinal assessment of preoperative comorbid conditions as well as complications after the initial surgical hospitalization. 8 This study was deemed exempt from institutional review board approval based on the use of deidentified records.
Patients identified in this database underwent PCNL. We then identified comorbid components of the MetS by ICD-9 code. These patients were categorized as having 0, 1–2, or 3–4 components of MetS. The 2001 NCEP:ATPIII definition of MetS was utilized, which includes obesity, hyperlipidemia, hypertension, or elevated fasting glucose. 10 Comorbidity assessment is built into the HCUP data set that identifies coexisting medical conditions not directly associated with the principal reason for admission. Comorbidities are identified utilizing ICD-9-CM codes and Diagnosis-Related Group codes on discharge. For each component of MetS, there is an indicator of whether or not comorbidity is present on admission.
In our PCNL cohort, we assessed how patient characteristics and degree of MetS predicted which patients had higher odds of having a postoperative MI during their hospitalization. MIs were identified by ICD-9 code and excluded if there was an associated present on admission indicator. Baseline characteristics were identified for all patients and were stratified into the number of MetS comorbidities. Descriptive statistics were performed with continuous variables reported as means with standard deviations, with a Student's t-test performed to assess significance. For categorical variables, chi-squared tests were performed. Univariate analysis was performed comparing patients who did and did not have a postoperative MI during their hospitalization. Multivariate logistic regression was then used to control for patient characteristics (age, gender, race, and primary insurance provider) as well as medical comorbidities significant on univariate analysis predicting increased risk of MI. All significance tests were two sided with an α of 0.05 considered statistically significant. All statistical analyses were performed using STATA® version 13.
Results
Using the HCUP database, 39,868 patients were identified who underwent PCNL between 2007 and 2011. Each patient was categorized as having 0, 1–2, or 3–4 components of MetS. Patient demographics were identified and stratified by MetS components. Of the nearly 40,000 procedures performed, the average patient was 59.9 years old. 48.1 percent of all the patients were male, and 61.7% were Caucasian. Seventeen thousand nine hundred thirty-two (45%) had 0 components of MetS, 19,268 (48.3%) had 1–2 components, and 2668 (6.7%) had 3–4. Table 1 demonstrates the baseline patient characteristics of this cohort.
MetS = metabolic syndrome; PCNL = percutaneous nephrolithotomy; SD = standard deviation; UTI = urinary tract infection.
Univariate analysis was then performed to determine rates of perioperative MI following PCNL (Table 2). Of all the PCNLs performed, 350 patients (0.9%) had a postoperative MI. Older age, use of Medicare or Medicaid as primary insurance, preoperative urinary tract infection (UTI), and an increased Charlson comorbidity index were all associated with a significantly increased risk of postoperative MI. In addition, comorbidities of congestive heart failure (CHF), valvular heart disease, chronic renal failure, chronic lung disease, or peripheral vascular disease were all associated with increased rates of MI. Of the components of MetS, obesity, diabetes mellitus, and hypertension were all independently associated with a significantly increased risk of postoperative MI. Dyslipidemia approached but did not reach a statistically significant increased risk (p < 0.06).
Bold type indicates statistically significant (p < 0.05).
On univariate analysis, with increasing MetS components, there was an increased incidence of postoperative MI. Patients with 0 MetS had a 0.6% risk of postoperative MI. Patients with 1–2 MetS had a 1.0% risk of postoperative MI. Patients with 3–4 MetS diagnoses had a 1.8% risk of postoperative MI (p < 0.001) (Fig. 1).
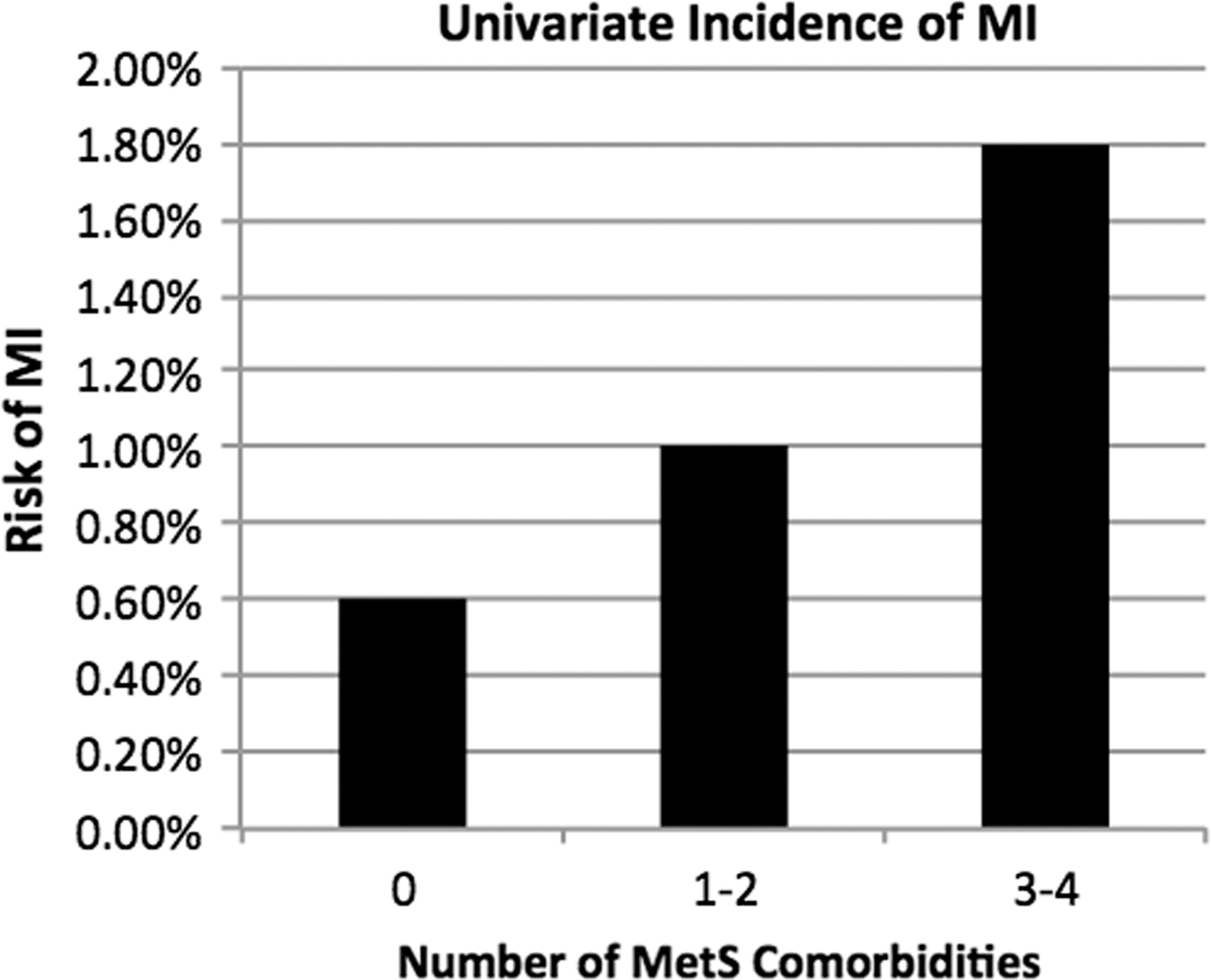
Univariate analysis shows that the increasing number of MetS comorbidities is associated with increasing risk of MI. MetS = metabolic syndrome; MI = myocardial infarction.
Multivariate analysis was then performed and a model was created to assess the independent effect of MetS comorbidities on postoperative MI. This model controlled for other non-MetS variables that predicted postoperative MI on univariate analysis (age, use of Medicare/Medicaid, preoperative UTI, CHF, valvular heart disorder, chronic renal failure, chronic lung disease, and peripheral vascular disease). Through this analysis, the presence of 3–4 MetS diagnoses predicted MI (3–4 MetS, odds ratio [OR] 2.2, 95% confidence interval [CI] 1.54–3.15, p < 0.001). Having 1–2 MetS components did not predict increased risk of MI (OR 1.2, 95% CI 0.94–1.53, p = 0.147) (Table 3).
OR = odds ratio; CHF = congestive heart failure.
Discussion
While previous studies have demonstrated increased general complications after PCNL in patients with MetS, this study suggests that having 3–4 components of MetS is an independent predictor of postoperative MI. Although past research has shown that MetS is not a better predictor than increased BMI for all causes of MI, this cohort may elucidate a group of vulnerable patients in the postoperative setting. Nalbant and colleagues found a higher hematocrit loss in MetS patients undergoing PCNL. They speculated that the comorbidities of MetS produced vascular damage and thus increased blood loss. 5 While it is impossible to make such conclusions from this study, a similar vascular damage may contribute to increased risk of postoperative MI.
In the era of the Affordable Care Act and the possibility of Medicare/Medicaid reimbursement adjustments based on surgical outcomes and unplanned care, it is important to identify surgical risk factors for adverse postoperative outcomes. The univariate analysis demonstrated that there are many demographic factors and comorbidities that contribute individually to risk of postoperative MI. This analysis also showed that all of the individual components of MetS significantly (or nearly significantly) increased a risk of MI. Multivariate analysis, however, revealed that, controlling for non-MetS factors, having 3–4 MetS comorbidities did contribute to a significantly increased risk of MI. This suggests that identifying patients with true MetS (usually defined as central obesity + at least two additional MetS factors) may isolate groups of surgical candidates who need preoperative workup and closer postoperative monitoring. These patients may also be good candidates for medical optimization and MetS treatment before undergoing this usually elective surgery.
While this is a large population-based study, it is retrospective in nature and uses administrative data, thus presenting certain intrinsic limitations. MetS diagnoses were based on ICD-9 code and are thus subject to the limitations of coding errors and inconsistent definitions of obesity. PCNL technique was not documented and was performed at the discretion of the surgeon. Not all postoperative events may have been captured in this database and our information is only as accurate as the database input points. This study did not evaluate the use of antihypertensives, antidiabetic treatments, aspirin use, or lipid-lowering therapy. Thus, we did not assess any effect of the possible treatment modalities that are being used on these patients to improve their MetS. Continuing to expand this database and analyze the data over time may help to improve models to predict postoperative MI in patients undergoing PCNL. Since the components of MetS are often improved with lifestyle modification and medical treatment, further studies evaluating the benefit of these treatments on postoperative outcomes would be interesting and useful, especially in a group of patients who are already prone to stone disease. In addition, as some previous studies suggest that BMI is a similar risk factor to assess than MetS, comparing BMI alone to MetS may help to decide if this is truly a unique group of higher risk patients. 7
Conclusions
In a large cohort of patients, those individuals with MetS have an increased risk of MI following PCNL given their pre-existing comorbidities. Having 3–4 components of MetS is independently related to increased risk of postoperative MI.
Footnotes
Author Disclosure Statement
No competing financial interests exist.