
Abstract
Purpose:
To investigate the principles that govern ureteral stent failure by digitally and mechanically characterizing their luminal reduction in response to various extrinsic compression forces. To explore the relationship between ureteral stent “material area,” “luminal area,” and “cross-sectional area (CSA)” for resisting extrinsic compression forces.
Materials and Methods:
We mechanically investigated 4.8F (n = 9), 6F (n = 9), and 7F (n = 9) ureteral stents to determine parameters that contribute to resisting radial compression forces. Digitalized images of luminal reduction values under incrementally increased reductions of stent outer diameters were obtained (0%, 25%, 50%, and 60% of original outer diameter). Forces (Newton [N]) and percentage luminal reduction that resulted in complete ureteral stent obstruction were determined.
Results:
Uniaxial incremental compression in the radial direction demonstrated complete luminal reduction (95%–100%) when 58% to 62% of the outer stent diameter was compressed. The 6F ureteral stents demonstrated the greatest resistance to extrinsic compression and the greatest “material area” relative to “CSA” (mm2). The force (N) required for 50% compression of outer stent diameter was 10.44, 28.13, and 25.39 N for 4.8F, 6F, and 7F ureteral stents, respectively. The “material area”/“CSA” at 50% compression of the outer stent diameter was 76%, 86%, and 78% for 4.8F, 6F, and 7F ureteral stents, respectively.
Conclusions:
Maintenance of intraluminal stent diameter in the presence of extrinsic compressive forces is primarily dependent on the stent's ratio of “material area” to “CSA.” Urologists should be aware of these findings to decrease the risk of ureteral stent failure when treating extrinsic ureteral obstruction.
Introduction
T
Methods
Overview of experimental design
Commercially available ureteral stents were selected to evaluate the force (N) required to resist stepped or constant compression loading similar to extrinsic ureteric obstruction (n = 27). Studies were performed in the BioScience and BioEngineering Research group, University of Limerick, Limerick, Ireland. Ureteral stents of various sizes (French [F]) from Boston Scientific Percuflex Plus© were investigated (i.e., 4.8F [n = 9], 6F [n = 9], and 7F [n = 9]). Briefly, ureteral stents were compressed using a Mecmesin© Uniaxial test system (Fig. 1A and Supplementary Fig. S1; Supplementary Data are available online at
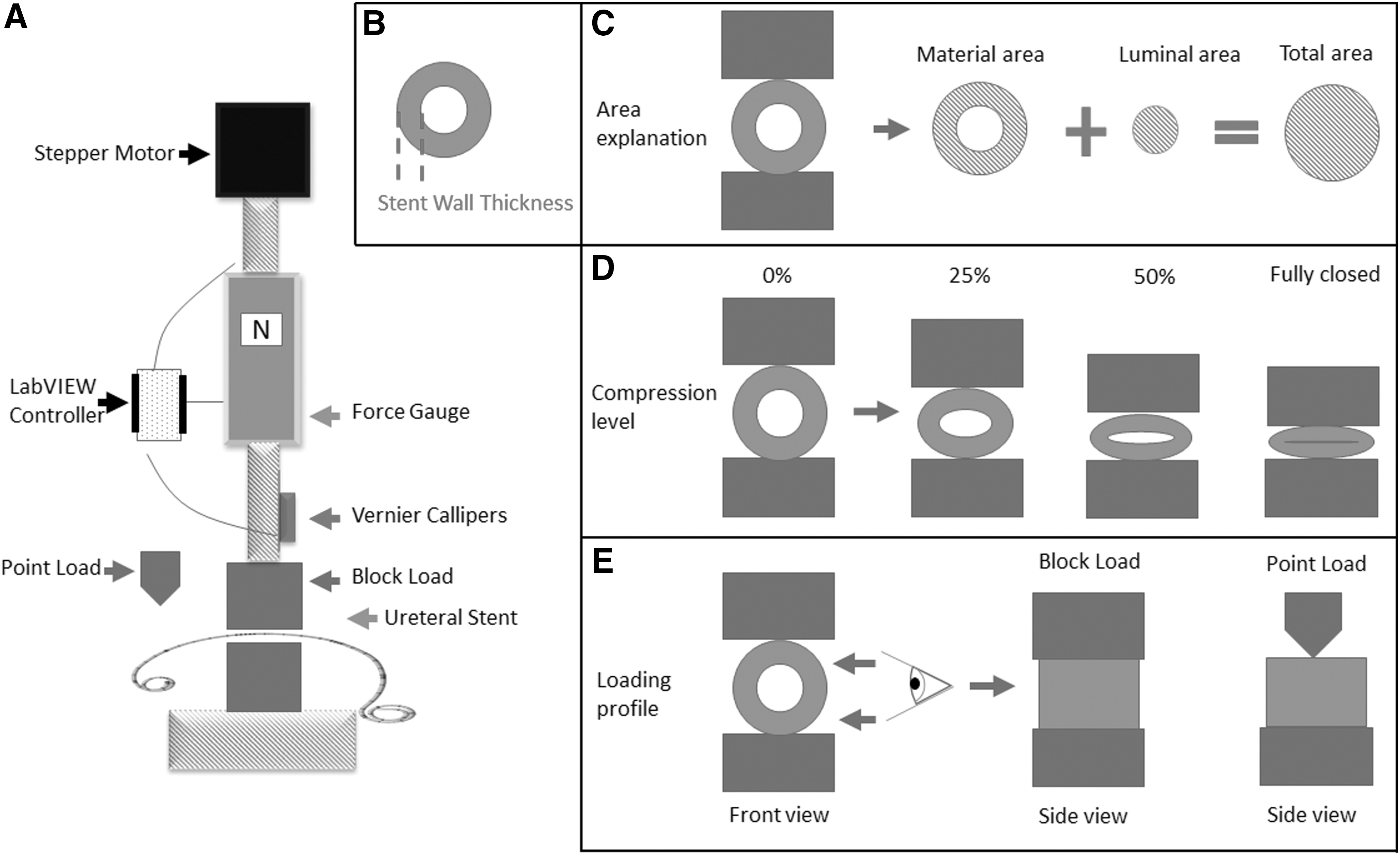
Overview of experimental set-up.
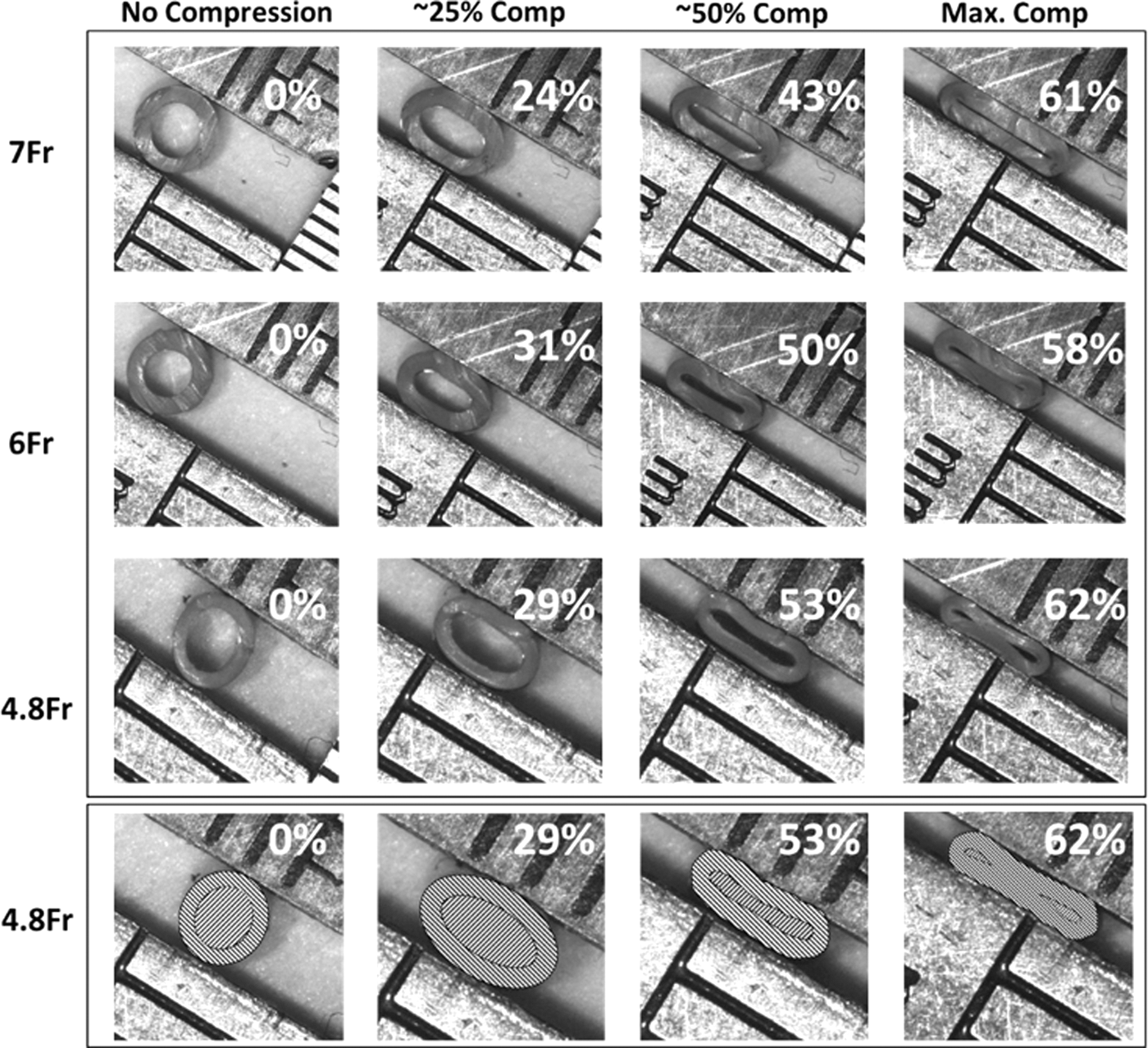
The total CSA of 7F, 6F, 4.8F Boston Scientific Percuflex Plus ureteral stents under compressions of 0%, 25%, 50% (of original diameter), and the maximal percentage compression required to occlude the stent's lumen. Figure 1(D) illustrates the purpose of this experiment to show the reduction of luminal area as the ureteral stent is compressed. The bottom row of grids depicts lumen CSA selection to record CSA measurement using Image J software (lines \ = material surface and lines / = luminal area). CSA = cross-sectional area.
Measurement of stent CSA
Figure 1B and C demonstrates definitions for “stent wall thickness (mm),” “luminal area (mm2),” and “material area (mm2)” that were measured using ImageJ© software. Image J is a freeware image processing program that accurately records imported image-based measurements (imagej.nih.gov/ij/). 4 Initially, a scale is set using a defined reference based on “calibration length” from the imported image. Once the appropriate scale was set based on a calibrated ruler, the freehand selection tool was used to manually trace the edge of the inner and outer diameter and form an enclosed area for the overall stent profile and lumen. Stent wall thickness, luminal area, and material CSA were recorded automatically from the enclosed area using the measurement function (Fig. 2, bottom row).
Mechanical characterization of ureteral stents
Ureteral stents were applied with an uniaxial compressive loading (constant or step) in a radial direction with a block load (25 mm) and a point load. Constant loading is defined as an unchanged rate of application of radial compressive force to the ureteral stent until 100% luminal reduction and similar removal of force (unloading) until no force is measured. Step loading is defined as sequential application of radial compressive force in 0.01 mm increments with a hold time of 30 seconds between steps. The same process is performed when the force is unloaded. The “point load” is a metal rod, with a radius of 1 mm, applied radially to the ureteral stent perpendicular to its longitudinal axis to mimic a “sharp” obstruction on the stent (Fig. 1E). The “block load” is a square block of metal that applies a flat surface, 25 mm in length, to the ureteral stent along its longitudinal axis, mimicking substantial extrinsic obstruction (Fig. 1E).
A stepper motor (Radionics 440–458) was controlled using a LabView card (USB-6218) at a strain rate of 0.1 mm/s where force values (N) were measured with a Mecmesin (BGF 50N) and displacement (mm) with a Vernier caliper (Mitutoyo 500-196; Fig. 1A). Block or point loads (Fig. 1E) were placed in contact with ureteral stents with a preload of 0.05 N. Loading was applied until 65% compression of the outer diameter (as this level of radial compression resulted in complete collapse of the stent and a spiked increase in force was seen due to compression on the lower clamp; Fig. 1D). Block and point load were applied at three different locations, proximal, central, and distal, along the lengths of each of the ureteral stents (Fig. 1A).
Results
Uniaxial incremental compression
Uniaxial incremental compression of ureteral stents in the radial direction demonstrated complete luminal reduction (95%–100%) when 58% to 62% of the outer stent diameter was compressed (Table 1). Tables 1 and 2 demonstrate the measured forces (N) of interest for the stent compression images illustrated in Figure 2 at intended compressions of 0%, 25%, 50%, and full luminal occlusion. The force (N) required for 50% compression of outer stent diameter was 10.44, 28.13, and 25.39 N for 4.8F, 6F, and 7F ureteral stents, respectively. The material area/CSA at 50% compression of outer stent diameter was 76%, 86%, and 78% for 4.8F, 6F, and 7F ureteral stents, respectively (Table 2). Figure 3 and Table 3 demonstrate that more force (N) was required to compress a 6F Boston Scientific Percuflex Plus stent compared with a larger 7F ureteral stent. This finding indicates that a 6F ureteral stent has the greatest potential for resisting radial compression and that “material area” relative to “CSA” is the most important stent parameter for resisting extrinsic compression forces in ureteral stents (Fig. 1, Table 2).
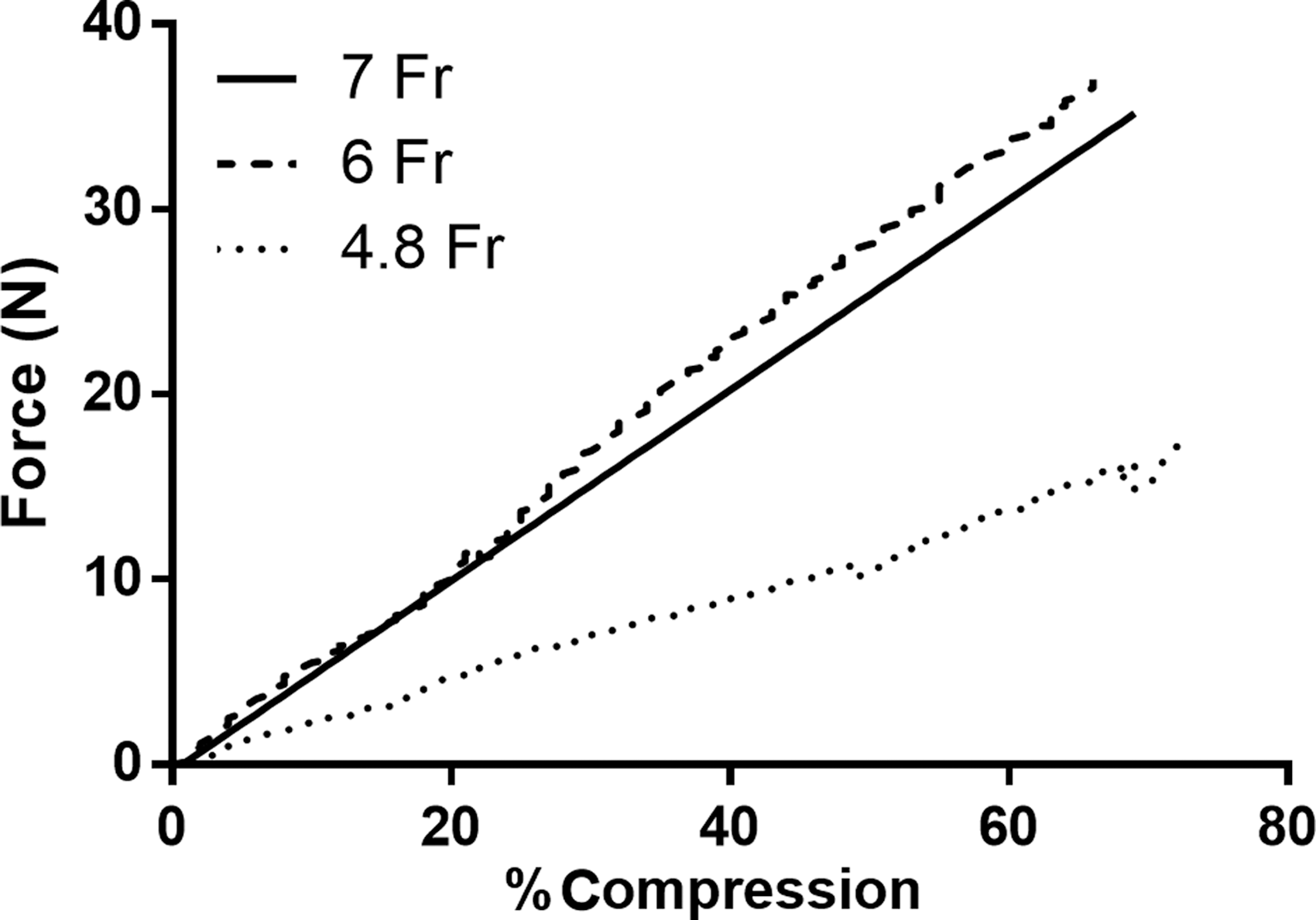
Force (Newton) vs percentage compression curves comparing the 4.8F, 6F, and 7F Boston Scientific Percuflex Plus ureteral stents using a block load during uniaxial compression. The 6F ureteral stents consistently demonstrated the greatest resistance to compression forces.
Force (N), Luminal Area and Wall Thickness Parameters for Ureteral Stents at Compressions of 0%, 25%, 50%, and Maximal Percentage Compression
The force (bold font) required to compress the lumen of 6F ureteral stents was consistently greater compared with 4.8F and 7F ureteral stents.
Material Area and Total Cross-Sectional Area for Ureteral Stents at Compressions of 0%, 25%, 50%, and Maximal Percentage Compression
The material/total CSA for 6F ureteral stents was consistently greater compared with 4.8F and 7F ureteral stents (bold font).
CSA = cross-sectional area.
Calculated Reduction in Internal Diameter (Left) and Compression Percentage Change in Internal Diameter (Right) at the Measured Force Values (2.5, 5, 10, 15, 20, 30 N) for Each Stent Size Based on Measured Internal Diameters
The percentage reduction in internal diameter is less for 6F ureteral stents (bold values) at the same force values as the 7F due to increased “material to total cross-sectional area” ratio.
Step loading vs constant loading
The difference in mechanical response between step loading (0.1 mm increment, 30 seconds hold) and constant loading (0.1 mm/s) was assessed (Fig. 4). There was no difference in the mechanical response for both loading conditions in 6F ureteral stents. Step loading demonstrated stress relaxation properties in the material as the force required to displace the stent reduced over the 30-second hold. This finding indicates that a gradual reduction of the luminal area in the stent can occur post-insertion with the potential decrease in urinary flow.
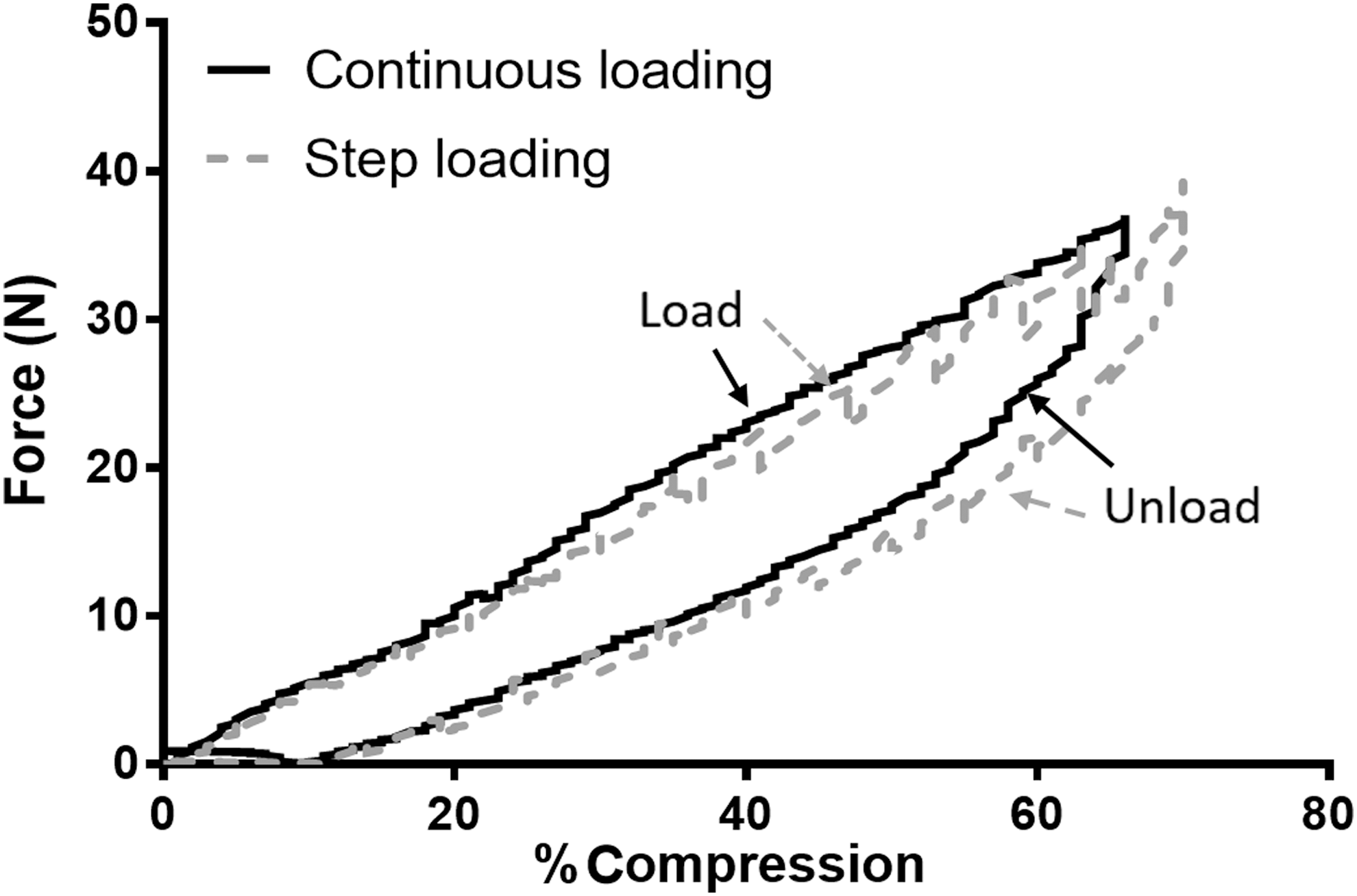
Comparison of continuous loading to step loading of a ureteral stent using a block load. A force (Newton) vs percentage compression graph of a 6F Boston Scientific Percuflex Plus ureteral stent undergoing load and unload continuously or with stepped intervals.
Mechanical response to block load and point load
Differences in mechanical responses between block and point load at central, proximal, and distal 6F ureteral stent locations were compared (Fig. 4). In both load conditions (block or point), there was no difference in the mechanical response for each location (Fig. 5). A large increase in force is required to compress ureteric stents with a block load. The circumferential compressive effect of block load is more representative of physiological malignant extrinsic compression compared with point load, which is typically used for uniaxial radial compression tests that may clinically represent penetrating compression forces.
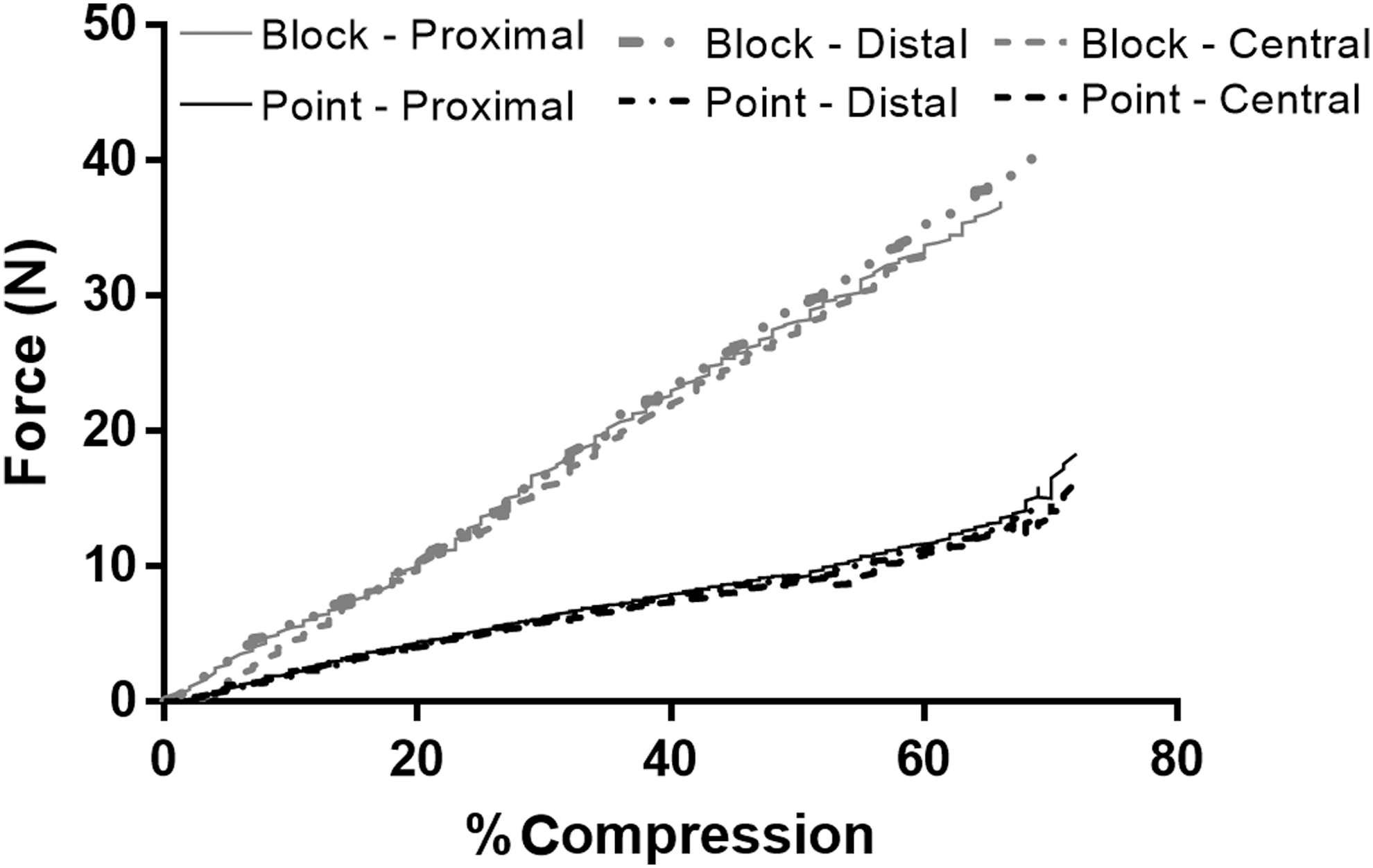
Force (Newton) vs percentage compression (percentage of outer diameter) comparison of block and point radial compression loading at proximal, distal, and central locations of Boston Scientific Percuflex Plus 6F ureteral stents (three locations on the same stent).
Discussion
Extrinsic ureteral obstruction is frequently managed by ureteric stenting to drain the renal collecting system. Malignant pathological conditions account for 90% of cases of ureteral obstruction, and the pathophysiology is due to extrinsic radial compression that is mimicked in the present in vitro ureteral stent evaluation study. 5 After placement of a ureteral stent, the most important end-point is maintenance of continuous urinary flow. Ureteral stent failure is a multifactorial process involving the patient's disease process and the design characteristics of the inserted ureteral stent. 1 When managing malignant ureteral obstruction with a ureteral stent, the treating urologist should be familiar with several parameters such as the stent's mechanical properties, fluid mechanics in stented ureters, and the pathological ureteral obstructive process. The main finding of the present study is that complete ureteral stent occlusion due to extrinsic compression occurs when 58% to 62% of the outer ureteral stent diameter is extrinsically compressed. An important secondary finding is that ureteral stent “material area” relative to “CSA” is the most important parameter for providing resistance to extrinsic compressive forces.
Typically, ureteral stents facilitate efficient urine flow through their lumen and around their circumference. In the initial phases of malignant ureteral extrinsic obstruction, urine will not drain around the stent due to compressive forces between the inner urothelium of the ureter and the outer surface of the inserted ureteral stent, so flow must occur through the lumen of the stent.
6,7
Urinary flow is governed by the principles of Poiseuille's law, which states that Poiseuille flow (steady flow in a straight, rigid, circular pipe) is determined by the resistance to flow (Rf) and is expressed by equation
7
:
where μ = fluid viscosity, L = length of flow channel, and R = radius of flow channel.
Therefore, maintenance of luminal patency is vital for continuous and efficient urinary drainage for ureteral stents as drainage flow rates through stented ureters are very sensitive to changes in channel radius and luminal CSA (Table 1), and that flow resistance is inversely related to the fourth power of the radius. Given that Poiseuille's law explains such flow, the larger the inner luminal diameter of a ureteral stent, the greater the flow rate. Herein we noted that a 6F ureteral stent had a greater ability to resist radial compression compared with its 7F counterpart due to its greater material surface area (Fig. 3, Table 2). This principle remained consistent for a number of additional stents tested in a post hoc analysis (Supplementary Fig. S2). Our unique finding is important as it demonstrates that “material area” relative to “cross-sectional area” is the most important parameter for resisting extrinsic compression forces and maintaining flow through a patent ureteral stent lumen. Interestingly, this is counterintuitive to the traditional clinical credence that a larger stent leads to greater resistance to extrinsic compression and greater urinary flow rates.
Our study is unique in design and method because it uses validated digital imaging software to accurately measure many ureteral stent parameters such as luminal CSA and percentage luminal reduction for each stent investigated at multiple compression forces. Accurate digitalized area measurements are important because of the relationships between radius, luminal area, and Poiseuille flow. 8 Digital imaging methodology has not been previously considered for investigating extrinsic compression forces on ureteric stents, and the concept of “material area” for resisting extrinsic ureteral stent compression has been neglected.
In this study the relationship between the amount of force (N) required to compress the stent radially and the percentage displacement is also demonstrated. It is imperative, when analyzing force data, to also measure and understand the amount of material in the cross-section of the stent, as this has a direct effect on the amount of “stress” within the stent when compressed. Stress is a measure of the amount of force over CSA, and in the case of a hollow tubular structure (e.g., ureteral stent), the amount of material and its ratio to total CSA is of paramount importance as demonstrated in our findings. Our findings demonstrate that the volume of material (or thickness of the stent) is an important parameter to consider for designing ureteral stents. For a 6F ureteral stent, the larger ratio of material area to total area at 0% compression (70%) compared with 4.8F (58%) and 7F (63%) clearly demonstrates that there is more “material” for the stent to withstand the forces being applied.
Our findings are also clinically relevant for cases of malignant obstruction where early ureteral stent failure rates are ≤58% with a large proportion of these failures occurring within 1 week. 5 Hübner et al. 9 found that conventional urinary pressure–flow characteristics are inconsistent when stents are subjected to external compression forces. 10 Notably, the authors also found that larger-diameter ureteral stents were more susceptible to compression, and this is likely due to variable reductions in their luminal CSAs in response to external compression as demonstrated in Figure 2 and Table 1. Currently, a variety of different ureteral stents are commercially available, and Hübner et al. 9 also emphasize that a stent's material components, such as the “hardness,” are more important than luminal diameter for maintaining urinary flow in the presence of extrinsic ureteral compression. 10 Consideration must also be given to patient factors such as ureteral peristalsis and the compressive forces created by the retroperitoneal process. 11
Understanding some of the fundamental principles that govern ureteral stent failure due to extrinsic compression is important because ureteral stents are relevant to the daily practice of urology. Known factors that contribute to stent failure include failure to maintain luminal CSA, encrustation, and luminal obstruction. 3 Alternatives to overcome these factors, in particular maintenance of luminal CSA, are placement of tandem ureteric stents, metal mesh stents, and coil-reinforced ureteral stents. 10 Pedro et al. demonstrated significantly more resistance to compression for coil-reinforced stents compared with standard ureteral stents. 10
A potential limitation of the present study is the in vitro nature. The true in vivo pathological forces exerted in benign and malignant obstructing processes are currently unknown, and a robust in vivo study with intraureteric pressure transducers may be required to gauge and define the range of extrinsic forces that are exerted during obstructive processes.
Future Perspectives and Conclusions
Our study confirms that the traditional French sizing still used in current labeling for ureteral stents does not reflect the stent's material composition, material surface area, or inner luminal diameter. Moreover, an alternative ureteral stent labeling system, which includes these data, would provide more accurate data on the potential drainage characteristics when decompressing extrinsic ureteral obstruction. This proposed labeling system would provide important information to clinicians to decrease the risk of early stent failure. Our findings demonstrate that maintenance of intraluminal stent diameter in the presence of extrinsic compressive forces is primarily dependent on the stent's ratio of “material area” to “CSA.” Ideally, when treating extrinsic ureteral obstruction, a ureteral stent should provide maximal material surface area to provide resistance to extrinsic compression, thereby encouraging maintenance of maximal internal luminal diameter to facilitate urinary drainage. Urologists should be aware of these findings to minimize the risk of early stent failure when treating benign and malignant extrinsic ureteral obstruction.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviation Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.