
Abstract
Renal ischemic time is one of the most variable risk factors in partial nephrectomy (PN). Our purpose was to investigate if intermittent ischemia could decrease renal impairment in the process of PN in porcine model and explore the feasibility of this surgical procedure in nephrectomy. A kidney ischemia–reperfusion injury model was successfully established in six pigs under laparoscopic surgery. One kidney of each pig was continuously ischemic, and intermittent ischemia was administered to the kidney of another side. Laparoscopic renal artery occlusion was applied to each kidney for 120 minutes. Intermittent ischemia was 15/3 minutes of cycles (ischemia for 15 minutes and reperfusion for 3 minutes). Microdialysis technique, immunohistochemistry, and histopathology were used to evaluate the extent of renal function injures. The concentration of glycerol in intermittently ischemic group was significantly lower than that in continuously ischemic group (F = 19.06, p = 0.001). NGAL and BCL-2 immunostaining of the renal tubular epithelial cell in the intermittent ischemia kidneys was significantly reduced compared with that in the continuously ischemic kidneys (F = 5.51, p = 0.041; F = 13.53, p = 0.004). Our study has shown that intermittent ischemia is a possibly effective and practicable surgical process for reducing renal ischemic damage in porcine model nephrectomy.
Introduction
Minimally invasive partial nephrectomy (PN) including robotic/laparoscopic is the viable approach for selected patients who are feasible to receive nephron sparing surgery. In PN, it is usually necessary to block renal blood flow by pedicle clamping, particularly for hilar tumors and larger or more deeply infiltrating tumors. 1,2 In the cases with the isolated renal tumors or the multiple renal tumors, ischemic time is one of the most variable risk factors for PN. Longer warm ischemia times are related to poor short- and long-term renal outcomes. 3,4 The primary objective of PN is to preserve more renal function. The duration of safe warm ischemia during PN remains controversial. 4,5 To maintain as much renal function as possible, we developed more comprehensive laparoscopic techniques, such as renal hypothermia, transient renal hilar control, zero ischemia PN, and controlled excision of the tumor in a bloodless field. However, the common major drawbacks of these techniques include complex manipulation, high risk of complications, and the possibility to perform operations only in selected patients. For instance, cooling the kidney safely and exactly during tumor resection remains a challenging issue, which leads to narrow surgical indications for the techniques. 6 –8 Thus, expanding the duration of safe warm ischemia and increasing the renal tolerance of vascular clamping are important clinical and experimental research objectives for challenging and complex laparoscopic PN.
Intermittent ischemia might be a beneficial intervention to reduce ischemia–reperfusion (I/R) injury and had been applied in various tumor resections. 9 Intermittent clamping was reported to attenuate liver damages and to facilitate recovery of the liver function in long-term ischemia compared with continuous clamping. 9,10 The aims of this study were to establish a model of porcine kidney I/R injury as well as to investigate if intermittent ischemia could alleviate renal function damage in the process of PN with obtained porcine model.
Methods
Animals and operative protocol
With the approval of the Ethical Committee of Chinese PLA General Hospital of the Chinese People's Liberation Army, six female pigs weighing close to 40 kg underwent general anesthesia and laparoscopic surgery. Anesthesia was maintained by using isoflurane in a 40% to 60% air–oxygen mixture adopting 2% isoflurane, and pulse oximetry levels were kept above 98%. During the whole operation, the pneumoperitoneum pressure was kept at 15 mm Hg. Standard PN procedure was performed with mobilization of the colon, renal arterial dissection, and clamping approaches. After renal hilum vessels were isolated, the renal artery was clamped with laparoscopic bulldog clamp. One kidney of each pig was continuously ischemic, and intermittent ischemia was administered to the kidney of another side; three right kidneys and three left kidneys were managed by each method and were included in intermittent ischemia group and continuous ischemia group. One hundred twenty minutes of laparoscopic renal artery clamping was administered to each kidney. Intermittent ischemia was performed in 15/3 minutes of cycles (ischemia for 15 minutes and reperfusion for 3 minutes), whereas continuous ischemia was performed by artery occlusion lasting 120 minutes. Subsequently, the laparoscopic bulldog clamp was removed followed by 30 minutes of reperfusion. None of the animals received any preconditioning treatment preoperatively. The whole experiments were conducted in line with correlative demands and rules.
Microdialysis and measurement of renal interstitial glycerol concentration
Microdialysis is a technique to collect samples by setting a small probe in a targeted organ and collect samples to analyze the interstitial molecules. It was found that the concentration of renal interstitial glycerol was directly related to the renal warm ischemia time, suggesting that glycerol was a specific maker that can reflect renal function in real time. 11 The microdialysis method was used to observe the correlation between renal function and glycerol concentration.
Before microdialysis probe was placed, the renal blood vessels were dissociated from the two kidneys, which ensured that there were no collateral vessels in the arteriovenous system. An 18-caliber 24-mm needle was placed under the laparoscope to the anterior mid-portion of the kidney at less than an angle of 45° to the surface of the kidney. Theoretically, the cortical depth of the kidney is no less than 12 mm in this area, and the needle from this angle ensured that the path was confined in the renal cortex. Then, we withdraw the needle and a CMA/20 Elite 14/10 polyarylethersulfone microdialysis probe (CMA Microdialysis, Solna, Sweden) was placed into the renal parenchyma through the needle sheath. The probe is available in a length of 24 mm and an outer diameter of 0.67 mm. In particular, a 10-mm permeability membrane (cutoff at 20,000 Da) is at the distal end of the probe. The CMA/400 pump was connected to the input tube and continuously pumped into the pump perfusate (CMA Microdialysis) containing 156 mmol/L chloride, 147 mmol/L sodium, 4 mmol/L potassium, and 2.3 mmol/L calcium and maintained at a rate of 1 μL/minute. After 30 minutes of equilibrium in which the probe was properly inserted into the kidney tissue with effective perfusion, a laparoscopic renal artery clamp was placed for artery occlusion and renal dialysis fluid was collected into a separate collection bottle for every 10 minutes. The renal artery was clamped continuously in kidneys of the continuous ischemia group and occluded for 15 minutes and then perfused for 3 minutes for a total of eight cycles in the intermittent ischemic group. A total of 3 samples were collected before ischemia, 12 samples were collected during the 120-minute ischemic time, and 1 sample was collected after the ischemia. Samples were stored at −80°C and then analyzed on the ISCUS Microdialysis Analyzer (CMA Microdialysis) for glycerol concentrations.
Renal cortical tissue interstitial fluid samples were assembled at 30, 60, 90, and 120 minutes to provoke an ischemia using a tissue biopsy gun. After 30 minutes of reperfusion (150 minute of experimental period), a piece of tissue blocks (5 mm × 5 mm × 5 mm) was cut from each kidney.
Immunohistochemistry
Corporate feasible antibodies were adopted in the whole studies of immunohistochemistry. The following antibodies were studied: anti-NGAL (1:50 dilution, mouse monoclonal, cat# BPD-ABS-048-28-02; Enzo Life Sciences, Inc., Farmingdale, NY), anti-Bcl-2 (1:250 dilution, rabbit polyclonal, cat# sc-492; Santa Cruz Biotechnology, Inc., Santa Cruz, CA), anti-caspase-3 (1:500 dilution, rabbit polyclonal, cat# ab4051; Abcam, Cambridge, United Kingdom), and anti-tumor necrosis factor alpha (TNF-α, 1:200 dilution, rabbit polyclonal, cat# ab6671; Abcam). The immunostaining level was measured by counting 1000 cells in 10 large grids visible under the microscope. The staining intensity was reported in the semiquantitative manner at a ratio of 0 to 3, where 0 was negative, 1 was weak, 2 was medium, and 3 was strong. It was reported that the percentage of tubular epithelial cell staining was 0% to 100%, with augment of 10%. The product of cell staining intensity and percentage forms a composite score. All slides were examined and scored independently by two pathological consultants blinded to the intervention. For any disagreement, a consensus was reached by discussion.
Histological examination
Histological processing
The samples were fixed in 10% formalin immediately and stored on it for 24 hours followed by 0.1 M phosphate-buffered saline until dehydrated. They were then inserted in paraffin and divided into 5-μm sections. The morphological changes were observed by periodic acid–Schiff staining, according to the standard protocol.
Histological analysis
In a blinded manner, 10 randomly selected areas in the cortical and medullary regions were evaluated under a light microscope. The histological kidney damages were analyzed by semiquantitative grading based on the following parameters/indexes: tubular necrosis, vacuolization of tubular cells, loss of the brush border, distortion of the tubular basement membrane, neutrophil infiltration, and intratubular casts. The sections of each kidney were examined by a pathologist blinded to the intervention. According to the detected changes/the percentage of damaged tubules per field, the level of each parameter was graded from 0 to 4 separately: 0 (normal kidney/no morphological deformities), 1 (≤25%), 2 (26%–50%), 3 (51%–75%), and 4 (>75%). Adding different scores of each index, the total score was defined as histopathological score and calculated for histological analysis.
Statistical analysis
The data are presented as mean (the standard error of mean) or mean (the standard deviation). Repeated-measures analysis of variance (ANOVA) was used for comparisons of the two groups regarding the glycerol concentrations at different time points. In particular, the date of 30-minute baseline interval and that of the last 30 minutes in each ischemic group were compared. Similarly, comparisons of the two groups regarding the immunohistochemical composite score at respective select time points were performed by using repeated-measures ANOVA. The Mann–Whitney nonparametric test was used to compare the histopathological scores between the groups. SPSS version 19 (SPSS, Inc., Chicago, IL) was used in statistical analysis. p-Value of <0.05 was considered statistically significant.
Results
The ischemia and reperfusion were confirmed by laparoscopic observation of the kidney. After the renal artery was occluded, the entire kidney immediately showed uniform blanching in all cases. After the removal of the renal artery clamp, the recovery of the renal artery pulsations and kidney color changes were observed in all cases. Figure 1 shows the mean renal interstitial glycerol concentrations determined by microdialysis in the intermittent ischemia group and the continuous ischemia group. The first 30 minutes meant baseline values, and the solid lines showed mean values in each group. The two ischemic groups did not differ in analyzed baseline concentrations. However, significant differences were noted after clamping the renal artery. Measurements and the glycerol concentrations increased with ischemic time in both groups (F = 69.62, p < 0.001); the intermittent ischemia kidneys had significantly lower glycerol concentration in the process of ischemia than the continuous ischemia kidneys (F = 19.06, p = 0.001).
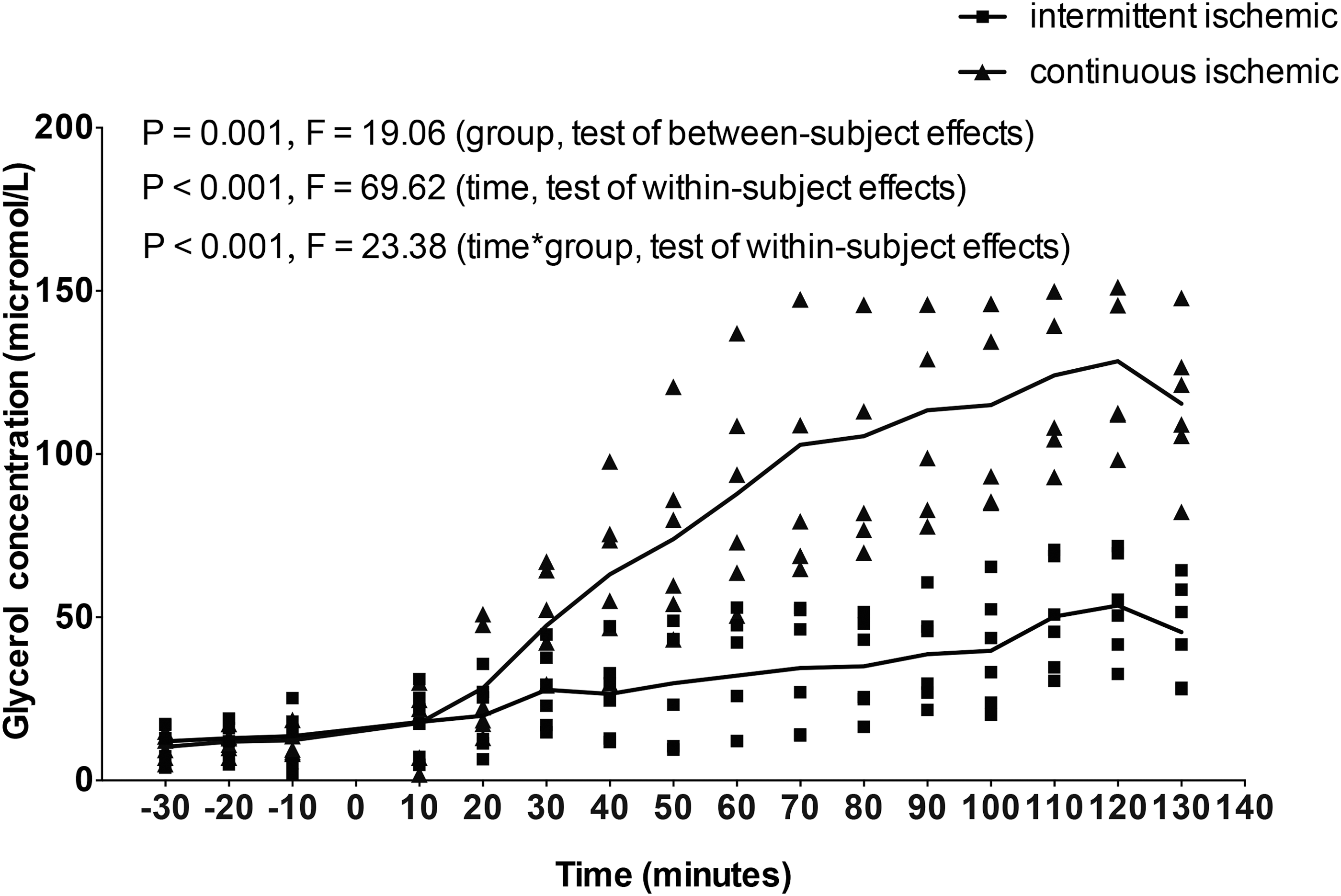
The effect of intermittent ischemia and continuous ischemia on renal cortical interstitial glycerol concentration levels. The first 30 minutes before ischemic period represent baseline values, and the long solid lines represent mean values in each group. Triangles indicate the intermittent ischemia group and squares indicate the continuous ischemia group. The degree of significance for glycerol concentration levels is shown in the upper right corner of the figure, using repeated-measures ANOVA. ANOVA = analysis of variance.
Figures 2 and 3 show representative immunohistochemical section images of the kidneys subjected to ischemia in each group. As shown in Figure 2B, the NGAL immunostaining of renal tubular epithelial cell in the ischemia kidneys increased with the prolongation of ischemic time (p < 0.001, F = 20.90). The NGAL immunostaining of the renal tubular epithelial cell in the intermittent ischemia kidneys were significantly reduced compared with that in the continuously ischemic kidneys (F = 5.51, p = 0.041). In Figure 2D, the BCL-2 immunostaining of the ischemia kidneys increased with ischemic time (p < 0.001, F = 30.09) and was significantly lower in the intermittent ischemia kidneys than in the continuous ischemia kidneys (F = 13.53, p = 0.004). However, no statistically significant difference was found in the other two markers (TNF-α and caspase-3 levels) between the two groups (Fig. 3B, D). With ischemic time increasing, both groups demonstrated an increasing tendency that was basically consistent with those previously described (F = 13.94, p < 0.001; F = 11.96, p < 0.001).

Comparison of NGAL and BCL-2 IHC in renal tissues between the intermittent ischemia and continuous ischemia groups

Comparison of IHC of caspase-3 and TNF-α in renal tissues between the intermittent ischemia and continuous ischemia groups
The histopathological examination of renal tissues revealed no significant difference between the continuous ischemia group and the intermittent ischemia group (U = 20.1, p = 0.55), whereas in each group, a significant high degree of impairments was observed with the increase of ischemia time (150 minutes vs 60 minutes, intermittent ischemia group: p = 0.002, continuous ischemia group: p = 0.003). Significant tubular damages (loss of the brush border, distortion of the tubular basement membrane, intratubular casts, and tubular necrosis) were found from tissue samples removed after the reperfusion period (150 minutes) in both groups. Briefly, we confirmed renal damage by histological examination using several characteristic morphological changes in each group; the sum of histopathological scores for each group is shown in Figure 4.

Representative photomicrographs and histopathological scores of renal tissues showing tubular damage [
Discussion
Transient renal artery occlusion is a common step and method of nephron sparing surgery. It is also one of the risk factors for chronic renal damage after surgery. 12,13 The time thresholds of irreversible renal dysfunction are confirmed in different conditions, indicating that the warm ischemia time is an important element for renal injury. 14,15 Renal I/R injuries have been extensively studied. In the ischemia process, a cascade of reaction that damages the renal tubular function occurred. The loss of adenosine triphosphate leads to imbalance of the sodium–potassium pump on the membrane. At the same time, the imbalance of the ion pump can lead to the dysfunction of electrolyte and water, and destruction of cytoskeletal components, which is the key to renal tubular function. 3 Reperfusion after the ischemic process may result in a series of inflammatory response and eventually produce destructive reactive oxygen species, leading to the death of tubular epithelial cells. 16
Ischemic intermittent occlusion in animal model has been studied in several researches. The results of these studies on intermittent occlusion are contradictory. Truss reported some advantages of intermittent clamping. 17 Formiga and colleagues presented a rabbit experiment to show that the artery only and intermittent clamping was the most protective clamping method, which is similar to our research conclusions. 18 However, some studies have also pointed out the defects of intermittent ischemia. Lyrdal found that intermittent occlusion for 30 minutes resulted in mild congestion compared with 30 minutes of continuous occlusion, but the degree of decrease in renal function was similar. 19 The absence of significant changes in renal function may be due to the short time of artery occlusion. Stueber and colleagues concluded that it might be better to escape the clamp opening when performing a nephtolithotomy. 20 However, they also pointed out that previous period of ischemia methods could have a protective effect after 3 or 4 weeks, which suggested that further studies are needed to investigate the long-term consequences of intermittent ischemia.
Using microdialysis technique, immunohistochemistry, and histopathological examination, this study showed that intermittent ischemia decreased renal function injury in a large animal model of renal warm ischemia. Microdialysis is a method for controlling the concentrations of molecules in the interstitial fluid of internal organs and tissues. This method involves implanting a microdialysis probe into the target organs and tissues, and continuously pumping into the pump perfusate through a probe to collect renal dialysis fluid into a separate bottle. The probe mimics the blood vascular capillary, allowing a certain part of the interstitial molecules to diffuse through the probe membrane. This method takes samples of extracellular molecules and provides a feasible technique for detecting cell stroma stability and cell function metabolic activity. The successful application of renal microdialysis method had been reported by several authors. 21,22 When the cell membrane keeps being damaged or disintegrates during ischemia process, the ingredients of the cell membrane could reach interstitial fluid, including glycerol. The direct relationship between glycerol concentration and the time of renal warm ischemia in animals and human kidneys showed that the markers were released continuously during the whole process of ischemia. 21,22 In this study, the concentration of glycerol during intermittent ischemia process was significantly lower than that in the continuous renal ischemia; therefore, we concluded that intermittent ischemia decreases renal function injury during renal warm ischemia.
The I/R is complex and associated with a series of inflammatory and cellular damage processes, involving the production of reactive oxygen species, inflammation, endothelial cell functional disorder, necrosis, and apoptosis. 23 In this study, we examined several biomarkers to analyze the protective effects of intermittent ischemia on tubular damage, inflammation, and apoptosis. NGAL was found to be a predictive biomarker of acute kidney injury for many years and a diagnostic biomarker of acute kidney injury, which emerges earlier than serum creatinine by 36 to 48 hours. BCL-2 signaling pathway was reported to play an important role in necrosis and apoptosis. Several studies showed that altered levels of BCL-2 have been associated with renal ischemia injury by activating a downstream caspase cascade and mitochondria-mediated apoptosis. Caspase-3 was also considered a pivotal molecule to mediate apoptosis, which may act as a downstream effector in this cascade. 24 TNF-α is a well-validated proinflammatory cytokine involved in the pathological process of I/R injury. 25 In the present study, the expression level of BCL-2 and NGAL during intermittent ischemia was significantly lower compared with that during continuous ischemia. However, no statistical difference was found in caspase-3 and TNF-α levels between the two groups. Considered together, intermittent ischemia may protect against acute tubular injury, cell inflammation, and apoptosis and may be a potentially effective technique to prevent I/R damage.
In our study, the glycerol concentration showed a significantly increased level during continuous ischemia. The immunohistochemistry data showed lower level of BCL-2 and NGAL in the intermittent ischemia kidneys. The histopathological changes were similar between the two groups. Therefore, we concluded that intermittent ischemia decreases renal function injury during renal warm ischemia. We suggest that the potential mechanism of intermittent ischemia may be the suppression of a series of cascade processes that produce injury in the cellular function. However, no significant difference was found in tubular injury among the two ischemic groups. We suspect that short reperfusion time would be the reason because warm ischemia time was 120 minutes, whereas the reperfusion time was only 30 minutes, and molecular level differences might not have had enough time to induce histological difference. However, renal functional recovery after the injury should be measured by accurate irreparable renal ischemic injury assessments. Serum creatinine, creatinine clearance, and renal scans should be analyzed with intervals of days to weeks after the ischemia before the final recovery of the renal function is determined. That should be performed in the subsequent experiments.
In our operative approach, we chose artery-only (AO) occlusion during PN. Many studies have compared perioperative results during PN with AO occlusion and renal artery and vein (AV) occlusion. Animal studies have suggested AO occlusion is more tolerance to ischemia than AV occlusion during PN. 26,27 According to previous literature reports, the advantage of AV clamping lies in shorter warm ischemic time and visualization of the tumor bed, especially for some complex renal tumors with large wounds, or severe intraoperative venous hemorrhage near the base of the tumor. 28 Therefore, which clamping method is more advantageous is still controversial, especially in cases with prolonged ischemic time. Further study is necessary to compare the renal functional outcomes of AO occlusion and AV occlusion with ischemic intermittent during laparoscopic PN.
Most centers are known to prefer a hypothermic approach on patients having potential chronic kidney disease or a solitary kidney. However, with the advent of minimally invasive approach in renal tumors, it is still a challenging problem that how to cool the kidney effectively in safety and decrease the ischemic injury during tumor resection. Hypothermic approach includes external surface cooling using ice or low-temperature solvents, intravascular cold-infusion techniques using vascular catheters, and retrograde renal pelvis perfusion. However, the high cost of interventional radiology, the long time in guiding a catheter to the renal artery under fluoroscopy, the potential incidence after the femoral artery puncture, exposure to contrast, and fluoroscopy are the major drawbacks of these techniques. 29
Zero ischemia was subsequently introduced as a technique to eliminate the renal ischemia induced by hilar clamping. However, zero ischemia is a challenging approach and can be only applied to highly selected patients and has not been widely accepted. 7,8,29 If intermittent ischemia can be applied in laparoscopic surgery, it might be an innovative and suitable approach for renal tumor diseases to reduce the impact of ischemia injury. In addition, it provides an opportunity to immediately use this technique depending on the intraoperative condition, whereas the application of external surface cooling techniques has to be discussed in preoperative decisions.
In conclusion, a model of porcine kidney I/R injury was established in success. Our findings demonstrated that intermittent ischemia could alleviate renal function damage in the process of PN with obtained porcine model. As far as we know, there is no animal study on the effect of intermittent ischemia in laparoscopic PN and comparison of different ischemia methods. Further studies are needed to investigate the long-term consequences of intermittent ischemia in the porcine model.
Footnotes
Acknowledgments
The supportive programs were the screening and clinical validation of characteristic protein biomarkers in renal cancer based on a large-scale biobank (2014AA020607, China) and clinical exploratory application of LESS and NOTES in urology (2012AA02101, China). This study was supported by the Ministry of Science and Technology of People's Republic of China.
Authors' Contributions
X.M., L.W., and C.P. contributed to study conceptual exploration and took part in the study design, data collection, data analysis, compilation, and interpretation. L.W., C.P., Y.G., Y.F., and L.C. contributed to general anesthesia and laparoscopic surgery. Q.M. and C.Z. devoted to the evaluation of immunostaining levels. X.M., L.W., Y.X., and L.R. contributed to data analysis and writing of the report.
Author Disclosure Statement
No competing financial interests exist.