
Abstract
Introduction:
Changes in the surgical treatment of nephrolithiasis, owing to recent technical advances and innovations, have made treatments more effective and less invasive. In this retrospective, observational cohort study, we identified the changing trends in the treatment of nephrolithiasis.
Materials and Methods:
We included patients with newly diagnosed nephrolithiasis who received any treatment in the United States, including extracorporeal shockwave lithotripsy (SWL), retrograde intrarenal surgery (RIRS), percutaneous nephrolithotomy (PCNL), and open surgery, from January 2007 to December 2014. Demographic factors, such as age, sex, region, surgical treatment type, and cost data, were analyzed.
Results:
The median age of patients at treatment was 52 years, and the ratio of men and women was similar. There were definite changes in the trends of all treatment modalities (p < 0.01). Both the number and percentage tended to increase for RIRS, whereas for SWL, the number increased, but the percentage showed a steady decrease. In PCNL, both number and percentage increased to a minor degree. The overall cost of nephrolithiasis treatments during the study period nearly doubled (from $30,998,726 to $57,310,956). The number of treatments and average cost per treatment increased annually for each treatment modality. RIRS was the least expensive; the other procedures in decreasing order of their mean costs were as follows: SWL, PCNL, and open surgery.
Conclusions:
There was a gradual but constant change in treatment trends of nephrolithiasis, with an increasing trend for RIRS and a decreasing trend for SWL. Although PCNL has relatively invasive characteristics, it is still in steady demand.
Introduction
Urolithiasis, or urinary tract stones, is one of the most common diseases occurring in at least 13% of men and 7% of women over the course of their lifetime, with recurrence rates as high as 50%. 1,2 The prevalence of urolithiasis has been increasing due to population increases, diet, lifestyle changes, and underlying diseases. 3 Not only does urolithiasis exist in the form of kidney stones, which can cause inflammation, infection, hematuria, and kidney function deterioration, but it may also migrate to the ureter. Ureteral stones often require emergent medical intervention because they can cause tremendous flank pain and infection. This disorder presents a significant treatment burden within the health care system. 4,5
As with other diseases, consistent technical advancements provide surgeons and patients with several options for the treatment of renal calculi, including extracorporeal shockwave lithotripsy (SWL), percutaneous nephrolithotomy (PCNL), retrograde intrarenal surgery (RIRS), and conventional open surgery. SWL, which delivers shock energy to the stone extracorporeally, has represented a significant breakthrough in minimally invasive treatment since its development. This technology has provided effective and easily accessible options for patients with urolithiasis and has achieved satisfactory success rates; therefore, it is still considered to be the first-line treatment for urolithiasis. 6 Advancements in optic technology make it possible to approach the kidney stone through small-caliber incisions and to pass into the flank using a rigid renoscope through a procedure called PCNL. Despite its relative invasiveness, PCNL has become a major treatment for renal stone disease because of the ease of access and manipulation and success rate of treatment for large renal stones. 7 As optical and mechanical technologies continue to evolve, intrarenal surgery, which is called RIRS, using flexible ureteroscopic devices and lasers through a retrograde approach has emerged. RIRS was regarded as a promising methodology; thus, it was expected to replace all other methods of kidney stone surgery. 8 However, it was associated with some difficulty in the manipulation of the surgical device, particularly in cases of large stones, lower pole stones, or unusual kidney structure, and these drawbacks have yet to be fully overcome. However, it is still a viable and competitive treatment option and continues to grow as a treatment method for nephrolithiasis due to its technical advancement and minimally invasive nature. 9
Adaptation of new technology and changes in preference are taking place rapidly in management of renal calculi, but there are only a few studies reporting these changing trends. Research using large sample-size data would be the most useful method for looking at these large and time series trend changes. We sought to determine the changes in nephrolithiasis treatment trends, characteristics of these changes, and their effects on the total medical costs of nephrolithiasis treatments.
Materials and Methods
Data source
This retrospective, observational cohort study was performed using the IBM® MarketScan® Research Databases. These databases contain retrospective claims information, including inpatient and outpatient enrollment demographics in the United States. All data were deidentified to maintain compliance with Health Insurance Portability and Accountability Act (HIPAA) regulations. The Institutional Review Board (IRB) determined that because this research did not involve prospective testing on human subjects, IRB approval was not required.
Patients and data inclusion
We included all newly diagnosed patients with nephrolithiasis (aged 18 to 70 years) at the time of diagnosis, who underwent any form of treatment, such as SWL, RIRS, PCNL, and open surgery, from January 1, 2007, to December 31, 2014. The patient cohort with nephrolithiasis was selected using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code for renal calculi. Each of the treatment methods was searched by Current Procedural Terminology code.
Patients who were diagnosed with simultaneous ureteral and renal calculi were excluded because the existence of the ureteral stone might have influenced the choice of treatment method for the renal calculi. In patients who underwent SWL, three separate SWL treatments within a 3-month period were considered one treatment session. For patients who received two or more treatment modalities within 3 months, only the first treatment was counted as the study treatment because our goal was to determine the surgeon's first choice of treatment. For patients who received two or more treatments after a 3-month interval, each case was considered independently. Demographic factors, such as age, sex, region, and total cost, were extracted from the database. Cost estimates were calculated for patients who underwent SWL, as many as three trials within 3 months after the renal stone diagnosis. For patients who underwent surgery, the costs from the time of first diagnosis to discharge after treatment were calculated. For patients who had treatment-related complications, the entire cost accrued through the time of hospital discharge was included in the cost analysis.
Statistical analysis
To evaluate the trend over the years, the Cochran–Armitage trend test was applied for treatment trends, and a linear regression was used to evaluate the cost per treatment. Beta coefficients and 95% confidence intervals were reported. All tests were two-sided with p < 0.05 considered significant. Statistical software (SAS Institute Inc., Cary, version 9.4) was used.
Results
Over the 8-year study period, a total of 1,329,311 patients were diagnosed with nephrolithiasis; however, only 67,792 patients (5.25%) received any type of treatment. The annual treatment numbers increased from 2007 to 2012 (from 6208 to 10,113), but then slightly decreased until 2014. The median age of patients at the time of treatment was 50.3 years. In opposition to the known fact that nephrolithiasis occurs more commonly in men than in women, the number of treatments showed a similar distribution between sexes. Regional differentiation was also similar in terms of the number of stone diagnoses and treatments, in which both are quite increased in the southern region, indicating that the southern region has increased incidence of nephrolithiasis (Table 1).
Demographics and Characteristics of the Cohort
SD = standard deviation.
There were definite changes in trends for all types of treatment modalities (p < 0.01). Both the number and percentage tended to increase for RIRS, whereas for SWL, the number increased, but the percentage steadily decreased. For PCNL, both the number and percentage increased, but only to a mild degree. Within the period of investigation, the number of open surgeries was small and did not fluctuate, and the overall rate steadily decreased (Table 2 and Fig. 1).

The percentage of treatment types in each year.
Trends in the Treatment of Renal Calculi During the Index Years
SWL = extracorporeal shockwave lithotripsy; RIRS = retrograde intrarenal surgery; PCNL = percutaneous nephrolithotomy; OS = open surgery.
During the period of investigation, the treatment cost per year nearly doubled (from $30,998,726 to $57,310,956). Treatment numbers and average cost per treatment increased annually for each treatment modality. Among the various therapies, RIRS was the least expensive; the other procedures in decreasing order of their mean costs were as follows: SWL, PCNL, and open surgery (Table 3 and Fig. 2).
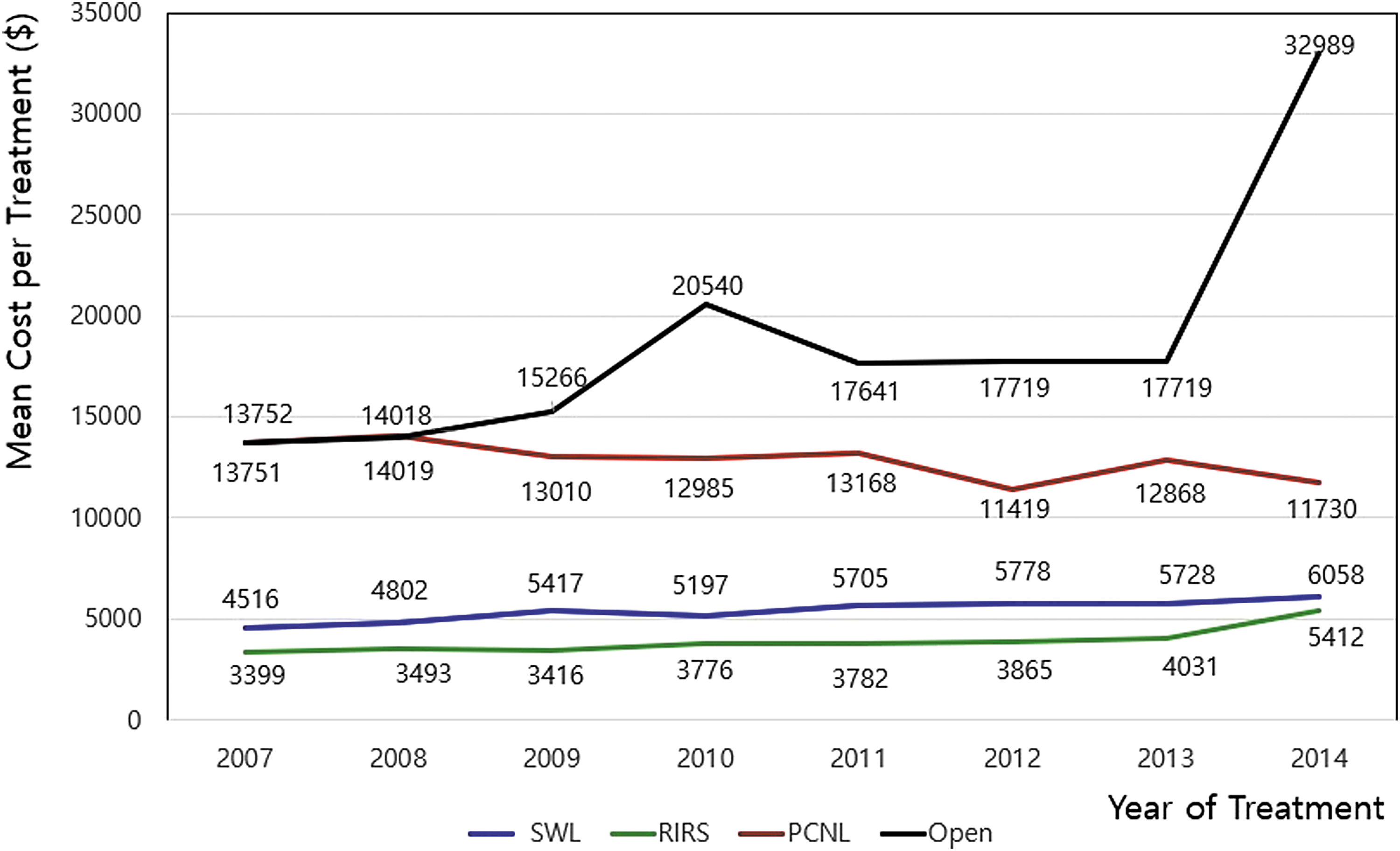
Mean cost per treatment type (in U.S. Dollars, adjusted to the level of 2014).
Medical Expenditures of Renal Stone Treatment (in U.S. Dollars, Adjusted to the Level of 2014)
The p-values are <0.0001.
The p-values are <0.001.
CI = confidence interval.
Discussion
In addition to the increased prevalence of urolithiasis and nephrolithiasis due to diet, lifestyle, and underlying disease, as well as increased detection rates due to improved medical accessibility and health examination, diagnosis of nephrolithiasis has been rapidly increasing. 3 As a result, treatment costs for renal calculi have imposed a great burden on the medical health care system.
Unlike patients with ureteral stones who usually need immediate medical intervention due to severe pain, patients with nephrolithiasis often do not need emergent treatment because they are often asymptomatic and the symptoms manifest slowly. Therefore, in cases of renal calculi found incidentally during testing in other departments, the stones are often ignored without treatment. Furthermore, even urologists are also hesitant or do not initiate active treatment recommendations when the calculi are too small and too numerous because of procedural efficacy and economic burden. In our study, only 5.25% of patients (69,792 of 1,329,311 patients) underwent treatment. Unfortunately, there are no specific guidelines on how to treat asymptomatic patients with multiple small stones. The only recommendation available, from the European Association of Urology (EAU), encourages the observation of small lower pole stones. 10 However, it is important to establish treatment principles in situations wherein 94.75% of patients are left untreated, because appropriate guidelines might give the patients and their doctors motivation to treat, thereby preventing potential renal damage and consequently decreasing the total medical cost to society.
Success rates are important factors to be considered when choosing the optimal treatment; however, it is quite difficult to make conclusions on the superiority of nephrolithiasis treatments according to their success rates. The lack of proper randomized prospective trials comparing different treatments is one factor that is associated with that difficulty. 8 Moreover, the other factor is the difficulty in comparing different procedural success rates owing to their associations with multiple factors such as calculus size, shape, composition, location, multiplicity, obesity, retreatment rates, and complications. 11 In addition, cost also should be considered. Therefore, it is difficult to determine the superiority of any treatment modality because these various factors are associated with various outcomes. The rationale used in choosing RIRS over SWL for treating nephrolithiasis has yet to be determined. There are some studies that have reported that the treatment success between SWL and RIRS is not significantly different. 12 –14 However, other studies have shown that RIRS has greater stone-free rates and lower retreatment rates and that RIRS may be more effective in terms of stone clearance after a single session, particularly for larger lower pole renal stones. 15,16 Given that the efficacy of RIRS is high despite its short history, it became one of the main surgical treatments for nephrolithiasis. It has also been reported that PCNL shows greater success for any stone size. Furthermore, the success rate of PCNL in the treatment of lower pole renal calculi was significantly better compared with SWL. 17,18
In this study, we identified a change in the treatment trend of nephrolithiasis, with RIRS showing an increasing trend and SWL demonstrating a decreasing trend. Given the fact that relatively large renal calculi are treated with PCNL and open surgery, PCNL and open surgery continue to be performed at a similar frequency. It was predicted that the number of RIRS procedures would surpass the number of SWL treatments within 3 years based on reports of a 5-year study of the trends in urolithiasis in England from 2009 to 2015. 13 However, in our study, the degree of increase in RIRS procedures was far less than predicted, which was probably due to some limitations, such as manipulation difficulty, delayed learning curve, or difficulty in access and fragmentation. Considering these limitations, RIRS is still an incomplete surgical option, and there is scope for further development. These limitations can also be overcome by technological advancements associated with development of microengineering and robotic surgery. If these innovations can overcome limits of RIRS, this procedure might overtake SWL as expected and eventually become the treatment of choice for renal calculi in a short period of time.
As with treatment of renal calculi in adults, the increase in RIRS has also been seen in children younger than 18 years, but the characteristic of the increase in performance of RIRS is slightly different from that observed for adults. The increase in RIRS is indicated by a decrease in PCNL (data not shown). In adults, RIRS has replaced SWL based on the premise that there is no significant difference in safety between RIRS and SWL; however, RIRS has replaced the more invasive PCNL in children (data not shown). PCNL in adults tended to increase because of the existence of mechanical limitations and difficulties in the approach with flexible equipment despite recent improvements in technology, whereas the most invasive open surgery decreased slightly.
When multiple treatments compete in the clinical field, decisions regarding the optimal treatment option in an individual patient are determined by medical factors, such as procedural efficacy, success rate, and safety. However, from a broader perspective, these decisions reflect the integration of factors, including the abovementioned factors, as well as doctor's preference, cost-effectiveness, medical care status, and insurance authorization. Therefore, identifying changing trends in the numbers or rates of certain treatments is important because it provides a comprehensive assessment of the treatment of that disease that can be used in clinical management. 19
The average cost per treatment and overall treatment numbers have been increasing annually, and therefore, the overall cost of treatment has also increased. In our study, RIRS was associated with the lowest cost among all the treatments, although the cost difference between SWL and RIRS is gradually decreasing. Although we should be looking at further changes in trends currently, we can say that these changes are desirable to curb the overall increased medical costs associated with the treatment of nephrolithiasis.
This study has some limitations using a large, retrospective cohort-based database to obtain patient and study data. First, various conditions such as location, multiplicity, and composition of renal calculi were not considered because we are unable to obtain this information from retrospective data. Second, we were not able to obtain important information of stone disease, such as the success rate or stone-free rate, because it is impossible to distinguish additional treatments and other stone treatments in a large dataset. Thus, in case of SWL, we considered three SWL treatments within a certain time period as one treatment session because SWL has a relatively low success rate during the first treatment (49–69%) and a high retreatment rate. 20,21 However, using this criterion, the following problems may occur: (1) in the case of more than two treatments for one patient, if the interval was less than 3 months, it was considered to be an additive treatment; thus, there might be underestimation; and (2) if the interval was more than 3 months, we counted all the procedures because it was predefined as treatment for contralateral or other new renal calculi; thus, there might be overestimation. Although these inevitable disadvantages exist in the study of kidney stones using a large dataset under the current disease classification code system, if the same criterion is applied annually in the case of data collection during the time series to compensate for these shortcomings, the large data study itself, which can show the whole flow, is also important and advantageous. Finally, there is a sudden increase of mean cost of open surgery in 2014, possibly owing to several severe and costly complications after open surgery. As presented, the number of open surgeries was too small (n = 20) such that the average cost increased dramatically owing to the significant increase in medical expenses due to some severe side effects.
In conclusion, our study found that there was indeed a change in the treatment trends for nephrolithiasis. These changes showed an increase in RIRS and decrease in SWL; however, due to limitations of RIRS, these changes are taking place gradually. Although PCNL has relatively invasive characteristics, it is still in steady demand as a treatment for nephrolithiasis.
Footnotes
Acknowledgment
The authors thank Robert Lawrence for his cooperation in editing this article.
Author Disclosure Statement
The authors state that there are no external sources of funding related to this research. There are also no competing interests to declare.