
Abstract
Introduction:
The natural progression of asymptomatic kidney stones remains unclear. Such knowledge may promote value-aligned care for patients and reduce potentially unnecessary procedures. We sought to evaluate the natural history of asymptomatic kidney stones in adults undergoing active surveillance.
Materials and Methods:
Using themes of “Kidney Stone” and “Active Surveillance,” we performed a systematic review by searching for studies in MEDLINE, all Cochrane libraries, EMBASE, Cumulative Index to Nursing and Allied Health Literature, BIOSIS, Scopus, and Web of Science from inception through October 2017—in addition to ClinicalTrials.gov, American Urological Association Annual Meeting abstracts (2014–2017), Google Scholar, and references of included studies and prior reviews. Two blinded reviewers independently extracted data and assessed methodological quality. We qualitatively summarized rates of surgical intervention (primary outcome), spontaneous stone passage, symptom development, and stone growth. We assessed the relationship between surveillance duration and rate of surgical intervention with Pearson's correlation coefficient.
Results:
Of 7034 unique records, 13 studies met final eligibility criteria. There was substantial variation in reported rates of surgical intervention from 6/85 (7.1%) to 80/301 (26.6%), spontaneous stone passage from 1/32 (3.1%) to 101/347 (29.1%), symptom development from 7/96 (7.3%) to 231/300 (77.0%), and stone growth from 5/96 (5.2%) to 33/50 (66.0%). Mean surveillance duration spanned from 11.3 to 80 months (range 2–180 months). Longer mean duration of surveillance did not correlate with an increase in surgical intervention rate across studies (n = 13, r = 0.01, p = 0.98), and this finding persisted when restricting analysis to observational studies (n = 9, r = 0.12, p = 0.76).
Conclusions:
Active surveillance appears to be a durable strategy for a majority of patients with asymptomatic kidney stones, as there was no increase in failure of watchful waiting despite increasing duration of surveillance. Higher quality studies are needed to ascertain which patients may benefit most from active surveillance.
Introduction
Costs for kidney stone care amount to over $2 billion annually, and the prevalence of kidney stones has increased in the United States from 5.2% in 1994 to 8.4% in 2010. 1,2 These findings are in part due to a rise in incidental asymptomatic stone diagnoses because of more frequent abdominal imaging. 3 The natural progression of asymptomatic kidney stones remains unclear; some patients may develop renal colic and require surgical intervention, whereas others may remain symptom-free and even undergo spontaneous passage. 4 –6
There are multiple guideline-endorsed management options for asymptomatic kidney stones, including active surveillance, ureteroscopy, percutaneous nephrolithotomy, and shockwave lithotripsy. 7 The 2016 American Urological Association/Endourology Society Guidelines provide conditional recommendation (Grade C) to practicing urologists that active surveillance may be offered to adults with asymptomatic kidney stones. 7,8 Yet, there is diverging evidence regarding the progression of asymptomatic kidney stones, 4 –6 and the choice of active surveillance must be weighed against the possibility of future symptom development and need for surgery. These trade-offs must also be compared with the option of prophylactic treatment and potential risks of surgical complications. 9 Two prior systematic reviews (including a published article and a conference abstract) have evaluated the natural progression of asymptomatic kidney stones and been unable to provide any definitive recommendations regarding optimal management. 9,10 Since these systematic reviews, there have been several more studies that have evaluated the natural progression of asymptomatic kidney stones, and these studies may shed further light on the issue. 4,11,12
One may question whether longer duration of active surveillance will lead to increased failure and need for surgical intervention. We examined this question through a systematic review evaluating the natural history of asymptomatic kidney stones; outcomes included rates of surgical intervention, spontaneous passage, symptom development, and stone growth in adults managed by active surveillance. With this knowledge, practitioners may be able to better predict outcomes and counsel patients regarding the various treatment options available. Patients and clinicians may feel more informed when selecting active surveillance, thereby not only promoting patient value-aligned care but also minimizing potentially unnecessary procedures.
Materials and Methods
Review protocol
We followed the Cochrane's recommended methodology as well as the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to report our methods and results. 13,14 Our original protocol was registered on the PROSPERO International Prospective Register of Systematic Reviews (CRD42018087110).
Study eligibility criteria
We included studies that reported the natural history of asymptomatic kidney stones managed with active surveillance for at least 2 months in adults who did not need their stones urgently removed. 15 We considered the terms active surveillance, watchful waiting, and conservative management to be synonymous—referring to the elective clinical decision to withhold surgical intervention.
Search methods
We searched MEDLINE (1946–2017), the Cochrane Library (1898–2017 for the Cochrane Central Register of Controlled Trials [CENTRAL], 1996–2017 for the Cochrane Database of Systematic Reviews [CDSR], 1994–2017 for the Database of Abstracts of Reviews of Effects [DARE]), EMBASE (1947–2017), the Cumulative Index to Nursing and Allied Health Literature (CINAHL) (1937–2017), BIOSIS (1926–2017), Scopus (1788–2017), Web of Science (1900–2017),
Outcomes and data collection
Our primary outcome was the proportion of patients or stones receiving surgical intervention. We deemed this outcome to be most meaningful to both patients and physicians when deciding how best to proceed with care. Surgical intervention composed of shockwave lithotripsy, ureteroscopy, or percutaneous nephrolithotomy. Secondary outcomes included the proportion of patients or stones experiencing spontaneous stone passage, symptom development, and stone growth. We included these often-described outcomes in stone care to offer a better understanding on the natural history of asymptomatic kidney stones. To broaden the scope of our review, we included studies regardless of how they defined these outcomes.
Two blinded reviewers (i.e., without knowledge of authorship, journal, or date of publication) screened titles and abstracts to determine study eligibility, excluding only clearly irrelevant articles. The remaining articles then underwent full-text assessment in duplicate and were considered eligible based on prespecified inclusion criteria. After ascertaining study eligibility, two blinded reviewers independently abstracted study characteristics and outcomes using a standardized data collection form. Discrepancies at each stage of the systematic review were resolved by group discussion.
Data analysis
Measure of active surveillance effect
We reported the proportion of patients or stones undergoing surgical intervention, spontaneous passage, symptom development, and stone growth—in addition to summarizing author-reported predictors (i.e., patient and stone characteristics) for these outcomes. If average surveillance duration was provided, we plotted these values against their study's respective rate of surgical intervention; we assessed the relationship of these variables with Pearson's correlation coefficient with STATA version 15. 16 We calculated missing data such as standard deviation of age and initial stone size using individual subject values. 17
Sensitivity analysis
We restricted the correlation analysis by study design to see if this changed the overall direction, magnitude, and significance of findings.
Methodological quality assessment and publication bias
Two blinded reviewers independently ascertained methodological quality using the Cochrane Risk of Bias tool for randomized controlled trials (RCTs) and the NewCastle–Ottawa Scale for observational studies. 14,18 Because our analysis was not amenable to a formal test for publication bias, we aimed to minimize the possibility of publication bias by including not yet published articles and studies with both significant and nonsignificant results.
Results
Description of studies
Search results generated 11,189 records. After the study selection process (Fig. 1), 13 studies met inclusion criteria, including 9 cohort studies and 4 RCTs. 4,6,11,12,17,19 –25 During full-text review, we excluded two studies that included patients with asymptomatic postoperative stone fragments. 26,27 Collectively, the 13 articles encompassed 1636 patients diagnosed with at least 1 asymptomatic kidney stone. Table 1 describes the characteristics of included studies. There was a wide range of sample sizes (range 24–347 patients). In most studies, the majority of patients were male and older than 45 years. Table 2 summarizes the reported outcomes.
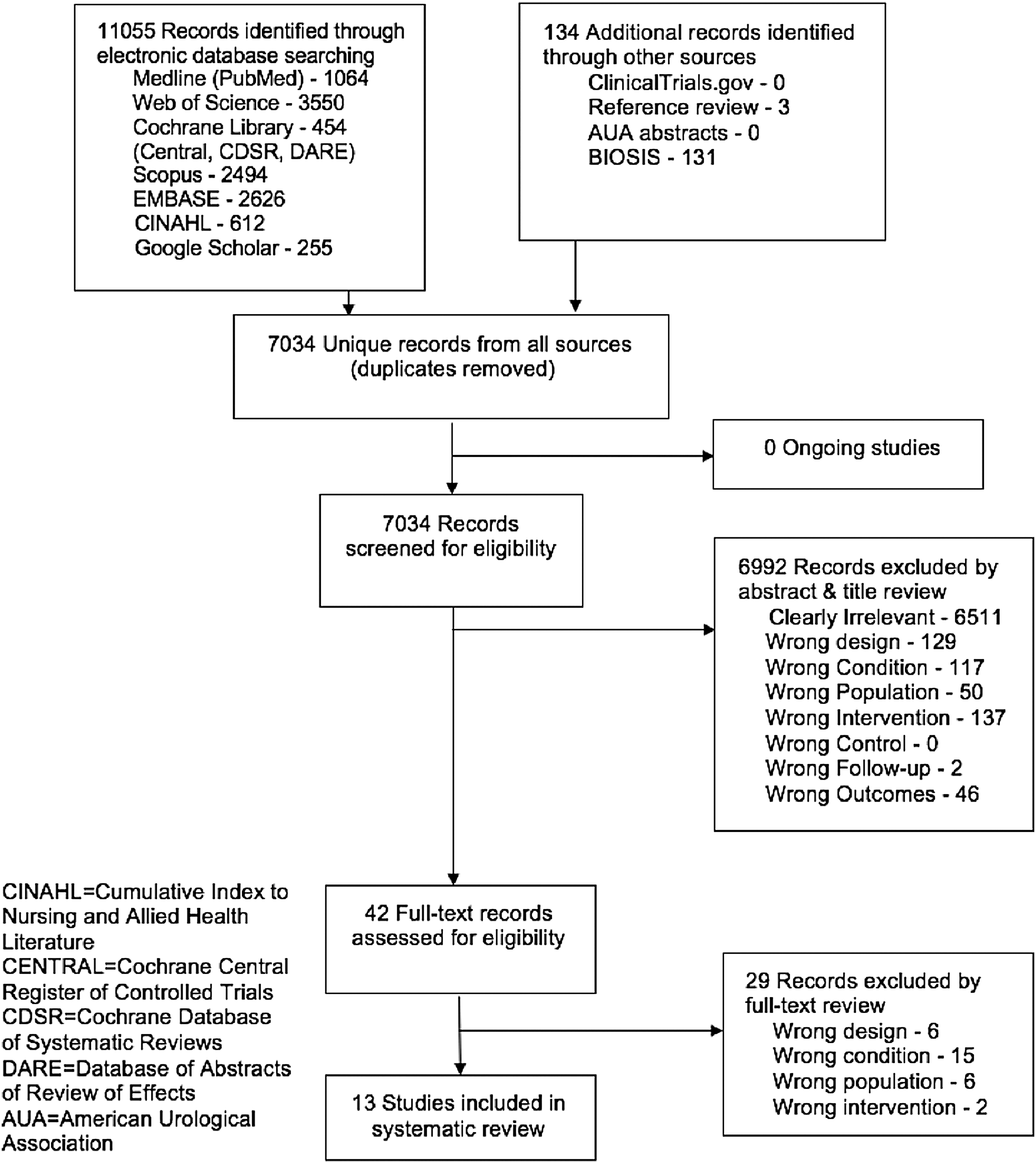
PRISMA diagram of study identification and selection. Of 7034 unique records captured in the search strategy, 13 studies met inclusion criteria and were included in analysis. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Baseline Characteristics of Studies Included in Systematic Review
Darrad et al., Dropkin et al., and Koh et al. analyzed their cohorts using renal units and were composed of 238, 110, and 50 patients, respectively.
Darrad et al. and Seseke et al. reported the median follow-up duration.
Measurements obtained from the study's initial cohort.
Jewett et al., Keeley et al., Sener et al., and Yuruk et al. reported completeness of follow-up: 79/79 (100%), 99/115 (86.1%), 47/50 (94.0%), and 32/33 (97.0%), respectively. Despite loss to follow-up, Sener and coworkers calculated outcome rates with 50 patients as denominator.
Yuruk and coworkers measured initial stone size in mm2.
L = lower pole; M = mid-kidney; NR = not reported; P = pelvis; PC = prospective cohort; Pt = patients; RC = retrospective cohort; RCT = randomized controlled trial; S = stones or renal units; SD = standard deviation; U = upper pole.
Primary and Secondary Outcomes of Included Studies
Burgher et al. and Yuruk et al. documented the symptom development statistic to include stone growth and other stone-related events.
Methodological quality of included studies
There was substantial variability in study design and outcome definitions. Among observational studies, it was uncertain whether patients were representative of the broader population due to investigator-dependent patient inclusion (Fig. 2a). 4 –6,11,17,19,20,23 For RCTs, it was unclear if research personnel were blinded to subject allocation 12,21,22,24 ; however, as authors were interested in hard outcomes, performance bias was less of a concern (Fig. 2b). Length of follow-up was deemed appropriate across studies with minimal risk for attrition bias, except for one study available only as an abstract at the time of review. 11
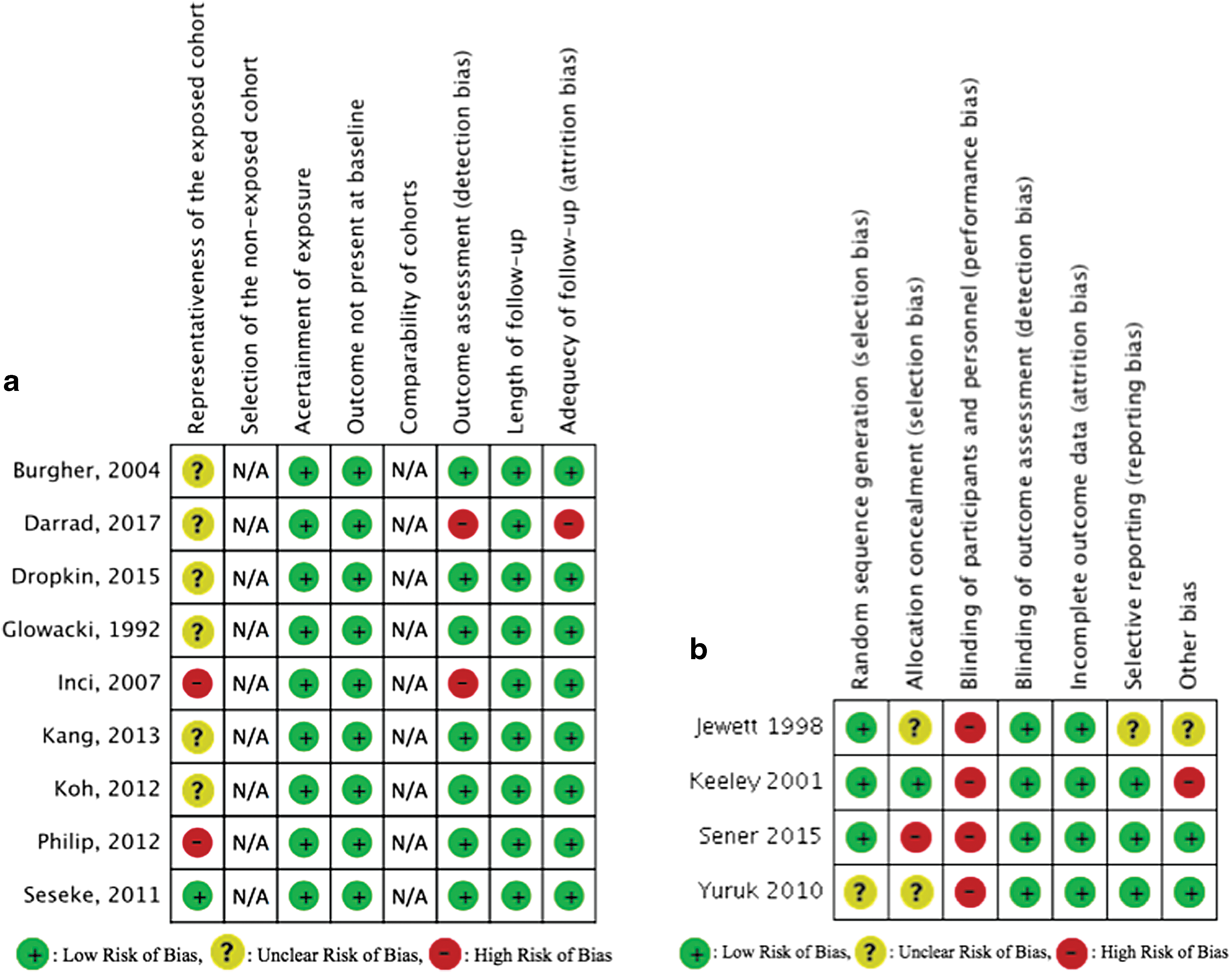
NewCastle–Ottawa Scale risk of bias tool for observational studies (
Surgical intervention rate
Surgical intervention rate ranged from 6/85 (7.1%) to 80/301 (26.6%) across all studies, with average surveillance durations spanning from 11.3 to 80 months (range 2–180 months). Many studies examined predictors of surgical intervention, and certain studies suggested a positive association between larger initial stone size and surgical intervention rate. 5,6,19,23 While Dropkin and colleagues did not observe that initial stone size was associated with intervention rate, the authors did find that kidney stones located in the upper pole and mid-kidney were significantly more likely to become symptomatic (28/69, 40.6%) than stones in the lower pole (17/70, 24.3%). 4 Conversely, Burgher et al. and Koh et al. did not find that stone location predicted disease progression. 6,19
Several studies reported time-to-event analyses. 5,17,20 Glowacki et al. and Kang et al. found that the cumulative 5-year probability of symptomatic events was 48.5% and 47.0%, respectively. 5,20 In 301 renal units, Darrad and colleagues observed that the average time to intervention was 42 months. 11 Among studies with relatively smaller cohorts, Inci and coworkers found that no patients required intervention during the first 24 months of follow-up, 17 and Yuruk and coworkers reported the average time to intervention as 22.5 months.
Some studies examined the association between stone growth and surgical intervention. Darrad and coworkers found that stones experiencing growth of more than 1 mm per year were significantly more likely to have either a stone-related symptom or require intervention. 11 In 300 patients, Burgher and associates found that the most common reason for intervention in upper pole stones was stone growth and that growth into very large stones (greater than 15 mm) virtually guaranteed intervention. 19 In contrast, Inci and associates found that no patients who experienced an increase in stone size required intervention. 17
Authors suggested that various other factors were associated with surgical intervention, including male sex, 5 younger age, 5,11 and stone radiodensity (HU greater than 1000). 11 Kang and colleagues found that patients receiving intervention were significantly more likely to have a stone history; however, Burgher and colleagues discerned no association. 5,19
Despite the varying patient and stone characteristics associated with surgical intervention rate, there was no correlation between average duration of follow-up and surgical intervention rate across studies (Fig. 3, n = 13, r = 0.01, p = 0.98). This finding was robust on sensitivity analysis when restricting to observational studies only (n = 9, r = 0.12, p = 0.76).
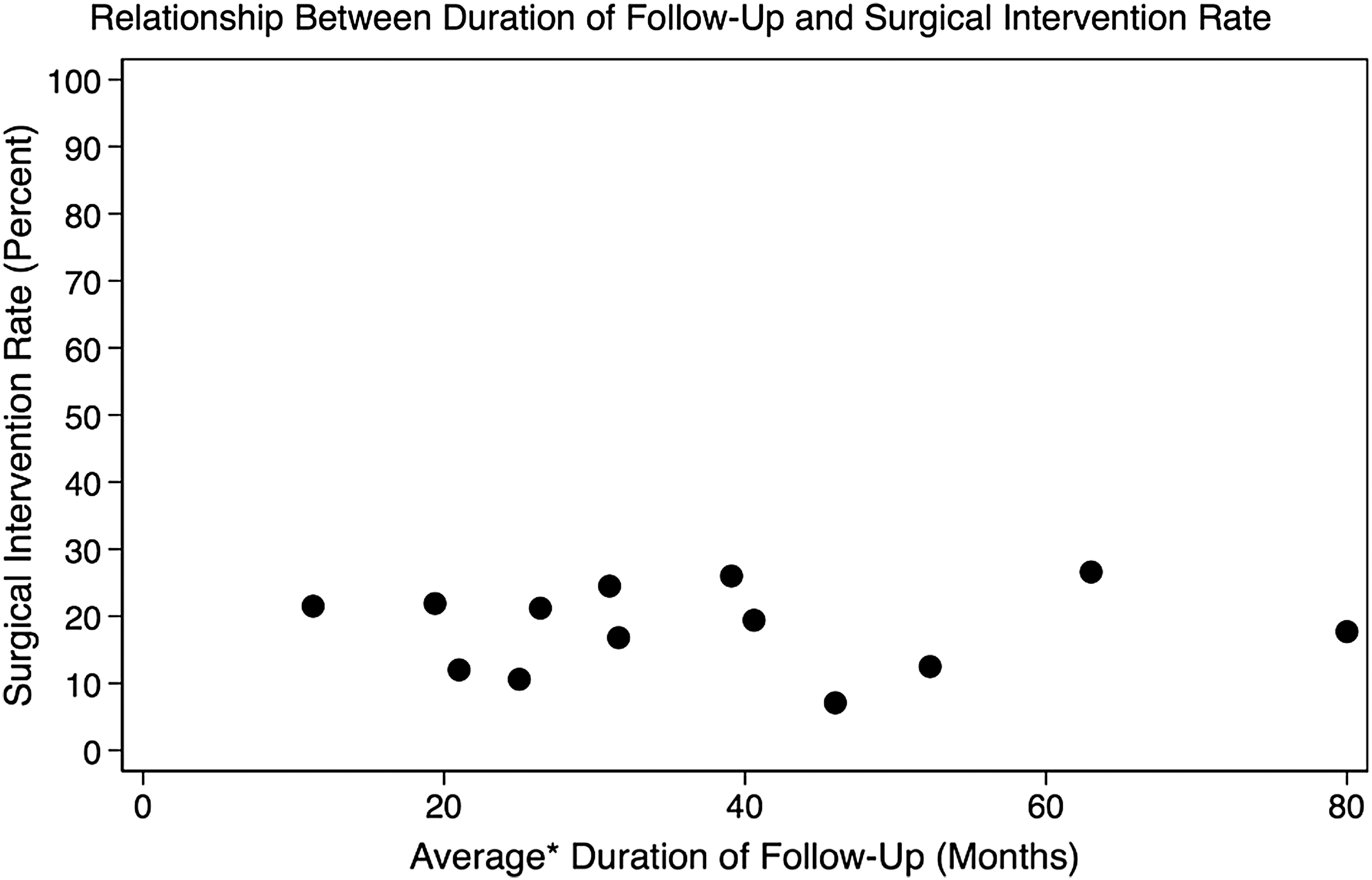
Relationship between average duration of follow-up and surgical intervention rate, where each point represents a study. Across all studies, there was no correlation between the duration of follow-up and surgical intervention rate (n = 13, r = 0.01, p = 0.98), which was robust on sensitivity analysis restricted to observational studies only (n = 9, r = 0.12, p = 0.76). *Darrad et al. and Seseke et al. reported the median follow-up duration.
Spontaneous stone passage
Among the nine studies reporting on spontaneous stone passage, spontaneous passage rates ranged from 1/32 (3.1%) to 101/347 (29.1%). Surveillance duration spanned from a mean of 19.4 months to a median of 63 months (range 6–180 months). Inci and colleagues found in their 24 patient cohort that 50% of stones measuring less than 5 mm, 16% of stones measuring 5 to 10 mm, and 0% of stones measuring greater than 10 mm passed spontaneously; specific ratios were not reported. 17 With a sample size of 85 stones, Koh and colleagues found that 16/57 (28%) of stones measuring 5 mm or less, 1/21 (4.8%) of stones measuring 5 to 10 mm, and 0/7 (0%) of stones measuring greater than 10 mm passed spontaneously. 6 Regarding stone location, Koh and colleagues found no significant difference in the incidence of passage according to initial stone location. 6 In contrast, Dropkin and colleagues reported that lower pole stones were significantly less likely to pass spontaneously during follow-up (2/70, 2.9%) when compared with stones in the upper pole and mid-kidney (10/69, 14.5%). 4
Symptom development and stone growth
The proportion of patients experiencing symptoms and stone growth ranged from 7/96 (7.3%) to 231/300 (77.0%) and from 5/96 (5.2%) to 33/50 (66.0%), respectively. Definitions for each outcome varied by study, with some documenting the symptom development statistic to include stone growth and other stone-related events. 19,24 Additionally, the definitions for stone growth spanned from any growth, 12,17 growth greater than 1 or 3 mm, 6 and growth greater than 50% from initial imaging measures. 4,5 Burgher et al. and Inci et al. found that larger stones experienced the greatest stone growth. 17,19 Glowacki and coworkers, however, reported that smaller stones had greater increases in stone size. 20 Considering stone location, Burgher and colleagues found that stone growth seemed less common in the upper pole and mid-kidney compared with that in the lower pole (47% vs 61%); specific ratios were not reported. 19 Koh et al. and Dropkin et al. did not find significant differences in stone growth based on stone location, although with relatively smaller sample sizes. 4,6,19
Publication bias
Efforts to identify unpublished studies through
Discussion
Summary of main results
Active surveillance appears to be a reasonable option for the majority of patients with asymptomatic kidney stones, as longer mean follow-up duration (extending from 11.3 to 80 months) does not correlate with increased risk of failure and subsequent surgical intervention rate. This finding is surprising given that one would expect a higher rate of symptomatic events and disease progression with longer durations of surveillance. Although a variable number of adult patients experienced stone growth or stone-attributable symptoms, only a minority underwent surgical intervention. Because most studies were observational, clinical judgment and individual surgeon threshold to intervene may be appropriate in selecting patients with asymptomatic kidney stones who can avoid surgery most of the time. Finally, smaller initial renal stone size was consistently reported as a predictor for spontaneous stone passage, 6,17 aligned with the results of a prior study investigating ureteral stones. 28
Comparison with other studies
A previous systematic review qualitatively analyzed five articles (four cohort studies and one RCT) on the topic and called for better understanding of the natural history of asymptomatic kidney stones to guide decision for intervention. 9 With 13 included studies, our findings add to the body of literature on asymptomatic kidney stone management by providing a more quantitative analysis. We not only demonstrate that approximately one quarter of patients will undergo surgical intervention—similar to the findings of a prior conference abstract on the topic 10 —but also that there appears to be no relationship between follow-up duration and surgical intervention rate across studies.
Annual follow-up appointments may be sufficient for patients with asymptomatic kidney stones, 9 and the American Urological Association recommends follow-up imaging as well. 7 However, an optimal follow-up schedule (e.g., imaging modality and frequency) has yet to be determined. That said, a recent study by Ravindra and coworkers suggests that perhaps more important than monitoring stone growth on serial imaging is educating patients with asymptomatic kidney stones to recognize symptoms of renal colic when they arise. 27
Quality of the evidence
We found an adequate number of studies investigating the natural history of asymptomatic kidney stones representing various international urologic communities. However, variability in study design (cohort study vs RCT) was a potential source of methodological sample bias; furthermore, differing secondary outcome definitions posed a challenge for interstudy comparisons. Additionally, the majority of studies lacked a control group, prohibiting a more robust meta-analysis. We therefore provided a more conservative correlation analysis of reported outcomes. Finally, two studies were only available as abstracts at the time of review, and so not all variables of interest may have been reported. 11,23
Strengths and weaknesses of the review
To provide clarity and transparency in the review process, this systematic review was registered a priori with PROSPERO. Additionally, we followed the methods outlined in the Cochrane Handbook and reported our results using the PRISMA guidelines. However, although all studies reported on surgical intervention, only a subset of studies reported on each secondary outcome. Furthermore, despite our comprehensive search strategy, it is possible that we may have overlooked relevant studies.
Conclusions
Overall, there was no correlation between mean surveillance duration and surgical intervention rate across studies. Furthermore, only a minority of patients in each cohort required surgical intervention—supporting that clinical judgment may appropriately guide patients to undergo active surveillance. With this knowledge, patients and providers may feel better-informed when deciding between active surveillance and intervention. Higher quality studies with active surveillance arms may provide information on which patients and stone characteristics (i.e., early stone growth vs stable stone disease) may benefit most from such management. Similarly, the development of a multi-institutional registry of patients with asymptomatic kidney stones who are managed by active surveillance may allow for larger sample time-to-event analyses, thereby further elucidating the natural history of disease.
Data Statement
The data underlying the article originate from the final 13 eligible studies in the systematic review.
Authors' Contributions
Conceptualization (D.S.H., D.L., N.B.V.R., V.M.P.), methodology (D.S.H., D.L., N.B.V.R.), formal analysis (D.S.H., B.A.Y.C.), resources (N.B.V.R.), data curation (D.S.H., B.A.Y.C., D.L., S.R., N.B.V.R.), drafting (D.S.H., B.A.Y.C., D.L., S.R., N.B.V.R.) and editing (all authors) of the article, supervision (N.B.V.R., V.M.P.), project administration (N.B.V.R., V.M.P.).
Disclaimer
Opinions expressed in this article are those of the authors and do not necessarily constitute official opinions of The Dartmouth Institute for Health Policy and Clinical Practice, Geisel School of Medicine, or Dartmouth-Hitchcock Medical Center.
Prior Abstract Publication
87th New England Section of the American Urological Association Annual Meeting, Podium Presentation (September 8, 2018) of the same title and author listing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.