
Abstract
Purpose:
Excessive bulking force during ureteral access sheath (UAS) placement may induce injury. The sliding friction between surfaces can be reduced with the application of ultrasonic vibration. We investigated the efficacy and safety of an ultrasonic vibration transducing device for reducing the maximal ureteral access sheath insertion force (UASIF).
Materials and Methods:
A device was developed for transducing ultrasonic longitudinal-axis vibration onto the UAS at an adjustable amplitude and frequency while measuring the degree of UASIF. In the pilot study, six porcine models were used to investigate the optimal amplitude and frequency of vibration and to calculate sample size. Twelve porcine models were utilized in a randomized controlled trial. Resected ureters were pathologically evaluated for ureteral injury.
Results:
The transduction of ultrasonic vibration at an amplitude of 0.04 g and a frequency of 18,000 Hz resulted in a maximal UASIF reduction of 36.4% (interquartile range 32.7–43.1). Maximal UASIF tended to decrease with increasing vibration frequency. No significant differences in UASIF reductions were observed according to amplitude. In the randomized controlled trial, the maximal UASIF reduction was 37.0% (interquartile range 21.4–44.2). Grade II injury was pathologically diagnosed in 8.3% (1/12) of the ureters in both groups.
Conclusions:
The transduction of ultrasonic longitudinal-axis vibration onto the UAS reduces maximal UASIF and does not harm the ureter. Reducing the velocity of sheath insertion may further reduce maximal UASIF.
Introduction
The use of a ureteral access sheath (UAS) has expanded the role of retrograde intrarenal surgery and has become increasingly popular. Advantages of the UAS include improvement of the collecting system access, facilitation of multiple entries, and reduction of intrarenal pressure. 1,2 However, a drawback for its routine use is ureteral injury caused by excessive force during primary access. Attempts have been made to decrease the UAS insertion force (UASIF), including hydrophilic coatings, prestenting, and active balloon dilation. 3 –5 Nevertheless, ureteral injury is still reported in up to 46% of cases. 4
Effective UAS placement depends on the friction of the sheath surface in relationship to the axial force that results in buckling of the sheath. 3 Therefore, it is feasible to develop means to minimize the UASIF by manipulating intrinsic and extrinsic factors. Alpha-blockers are used as a medical expulsive therapy for ureteral stones by reducing intraureteral pressure and ureteral contractions. 6 –8 In our previously reported randomized controlled study, a homemade UASIF measurement device was developed and utilized to demonstrate that preoperative α-blockade reduces the UASIF. An additional finding was that the UASIF should not exceed 600 g to avoid ureteral injury (≥GII). 9 Meanwhile, there have been no attempts to reduce the UASIF by manipulating extrinsic factors using mechanical intervention.
In mechanical engineering, it is well known that ultrasonic vibration longitudinal to the sliding direction reduces friction between the surfaces due to the change in the magnitude and direction of the resultant sliding velocity vector. 10 The amount of friction depends on the frequency and amplitude of the ultrasonic vibration and the properties of the sliding surface. 10 The beneficial effects of ultrasonic vibration have been applied in machining processes to improve performance, as in grinding, milling, and turning. 11
We developed a device with the capability of transducing ultrasonic longitudinal-axis vibration onto the UAS. The primary study endpoint of our randomized controlled trial was the efficacy of vibration for the reduction of the UASIF. The secondary endpoint was the safety of ultrasonic vibration in terms of ureteral injury.
Materials and Methods
Development of an ultrasonic vibration transducing apparatus
Figure 1 shows the representative diagram of the apparatus capable of transducing ultrasonic vibration onto the UAS and measuring the UASIF. The apparatus consisted of (A) an electromagnetic exciter to generate ultrasonic vibration (Minishaker Type 4810; Brüel & Kjær Sound and Vibration, Nærum, Denmark) with a frequency range from DC to 18 kHz and maximum peak-to-peak displacement of 4 mm, (B) a load cell (SMNT-32B; CAS Instruments), (C) a linear motion bearing, (D) a V-block jig to secure the UAS hub, (E) data acquisition software (LabVIEW™; National Instruments Corporation), (F) a DAQ (NI-9234; National Instruments Corporation) and a signal generator (NI-9263; National Instruments Corporation), (G) a load cell signal conditioner, and (H) a power amplifier for the exciter (Type 2718; Brüel & Kjær Sound and Vibration) with a power output capability of 75 W and a current range from 1 to 5 A at a voltage gain of 40 dB.

Representative diagram of the apparatus capable of transducing ultrasonic vibration onto the UAS and measuring the UAS insertion force. The apparatus consisted of (A) an electromagnetic exciter to generate ultrasonic vibration onto the UAS, (B) a load cell, (C) a linear motion bearing, (D) a V-block jig to secure the UAS hub, (E) data acquisition software, (F) a DAQ and a signal generator, (G) a load cell signal conditioner, and (H) a power amplifier for the exciter. UAS = ureteral access sheath.
In the absence of preliminary studies that may provide optimal ranges of frequencies and amplitudes that can minimize the UASIF, an electromagnetic exciter capable of providing wide ranges of frequency and amplitude was needed. Therefore, the Minishaker Type 4810 exciter was selected, despite its relatively large size and weight.
Ex vivo validation
The accuracy of the load cell measurement was validated using six serial weights (1–150 g) applied on the V-block jig. At a static state, linear measurements showed excellent correlation (r = 1.0; p < 0.001). To validate the dithering efficacy, the device was mounted on a linear ball-screw motor stage driven at a fixed insertion velocity of 20 mm/second. A 12/14F diameter UAS (Navigator™; Boston Scientific) and a biological sponge were used to measure UASIFs at amplitudes of 0.04 and 0.08 g at frequencies of 300, 500, 1000, 8000, 12,000, and 18,000 Hz. Compared to performance without ultrasonic vibration, a 21.0% reduction in the maximum UASIF was observed with ultrasonic vibration transduced at an amplitude of 0.04 g and frequency of 300 Hz (Fig. 2).
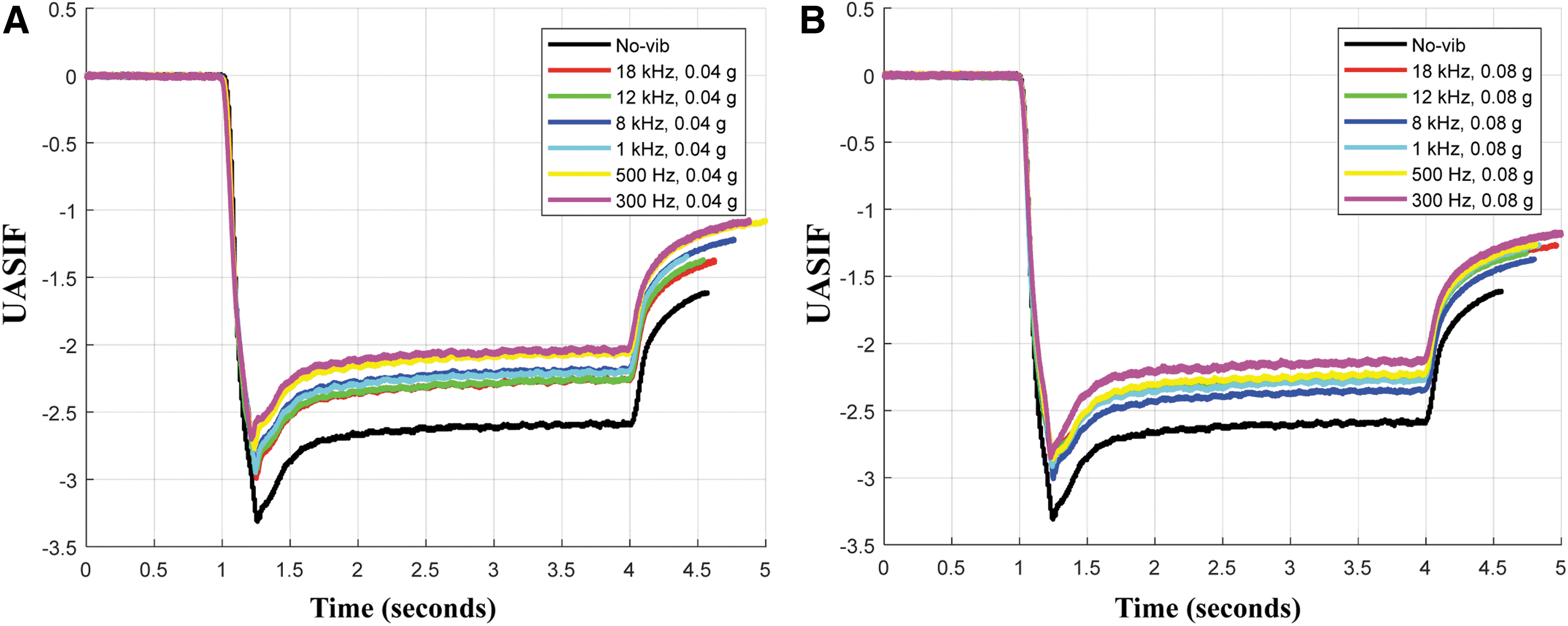
Ex vivo validation of the ultrasonic vibration efficacy for reduction of UAS insertion force. A linear ball-screw motor stage driven at a fixed velocity of 20 mm/second was used to measure insertion forces at 300, 500, 1000, 8000, 12,000, and 18,000 Hz frequencies, each at acceleration amplitudes of
Experimental animals and procedure
Animals
Yorkshire pigs weighing between 35 and 40 kg were used. Female pigs were used in all cases to facilitate cystoscopic identification of the ureteral orifices and to minimize the effect of urethral resistance. This study was approved by the Yonsei Biomedical Research Ethics Committee after review of the study protocol (2018-0166) and is reported according to the Animal Research: Reporting of In Vivo Experiments Guidelines. 12
Anesthesia
The pigs were fasted 12 hours before anesthesia. The induction of anesthesia was performed using a combination of telazol (4.4 mg/kg) and xylazine (2.2 mg/kg). All pigs were orotracheally intubated, and isoflurane (2.5%–3.5%) was used to maintain general anesthesia. Ketamine or atropine use was prohibited due to their potential effect on ureteral peristalsis.
Experimental procedure
In the lithotomy position, the standard procedure initiated with the cystoscopic identification of both ureteral orifices, followed by retrograde ureteropyelography to exclude preexisting ureteral stricture. After placement of a hydrophilic safety guidewire (ZIPwire; Boston Scientific) up to the collecting system, an Amplatz super-stiff guidewire (Urowire XF; Boston Scientific) was introduced under the guidance of a ureteral catheter. After removing the ureteral catheter and the cystoscope, the UAS attached to the ultrasonic vibration transducing device was placed over the Amplatz guidewire. In all cases, a 35-cm 12/14F diameter UAS (Navigator; Boston Scientific) was used. Before insertion, the UAS was soaked in saline without the use of lubricants.
Under fluoroscopy, the UAS was advanced until the distal tip reached the ureteropelvic junction. Intervention was performed by a single investigator (K.C.K.) blinded to the UASIF recordings, and measurements were recorded by investigators who were blinded to randomization (K.S.L. and G.R.M.).
Experiments were performed without applying vibration for the control ureters and with vibration for the contralateral experimental ureters at frequencies of 300, 500, 1000, 8000, 12,000, and 18,000 Hz, and acceleration amplitudes of 0.04 and 0.08 g.
Removal of the ureters for pathologic evaluation
To evaluate the effect of ultrasonic vibration on the ureteral mucosa, the ureters were harvested in vivo using laparoscopic instruments. One centimeter of the midureteral segments between the resection margins was fixed in 10% neutral-buffered formalin. Finally, the pigs were euthanized under anesthesia using 20 mL of phenobarbital.
The fixed ureters were serially cross-sectioned at 3 mm intervals and paraffin embedded. Hematoxylin and eosin slides were prepared, and the presence and grade of injury were evaluated by agreement between two pathologists (J.S.K. and B.J.L.), according to the previously reported classification. 4
Statistical analysis
The Mann–Whitney U-test and the Fisher's exact test were used to compare continuous and categorical variables, respectively. The one-sample t-test was used to calculate sample size. Statistical analysis was performed using SPSS software version 18 (SPSS, Inc., Chicago, IL) and PASS software version 12 (NCSS, LLC, Kaysville, UT). All tests were two-sided, with statistical significance set at p < 0.05.
Results
Pilot study and sample size calculations
Pilot study
A pilot study was performed to investigate the optimal amplitude and frequency of ultrasonic vibration, and to calculate sample size for a randomized case-controlled study. For this purpose, 12 ureters from 6 pigs were allocated to respective vibration settings (Table 1).
Pilot Study Results of Maximal Ureteral Access Sheath Insertion Force and Percent Reduction at Various Amplitude and Frequency Settings
UASIF = ureteral access sheath insertion force.
The peak UASIF observed during a single UAS placement session was considered as the maximum UASIF. An example of the UASIF measured with and without ultrasonic vibration is shown in Figure 3. Maximal UASIF measurements showed that at a set amplitude, the maximum UASIF tended to reduce with increasing frequency; however, this change was statistically insignificant (r = −0.45; p = 0.074). Compared to the control ureters, the maximal %reduction in median UASIF of the contralateral experimental ureters was 36.4% (interquartile range 32.7–43.1) at a vibration amplitude of 0.04 g and a frequency of 18,000 Hz. There were no significant differences in UASIF reduction between to the two amplitude settings (p = 0.468).

A case example of the UAS insertion force without ultrasonic vibration (blue line) and with ultrasonic vibration (red line). Red circle indicates the maximal UAS insertion force.
Sample size calculations
Under the presumption of α = 0.05, 1-β (power) = 0.8, and an estimated rate of decrease and standard deviation of 10% ± 10%, 10 samples were needed to validate our hypothesis. Considering an estimated dropout rate of 10%, the minimum sample size to find a difference between the 2 arms was 12 samples.
Randomized case-controlled study
Twelve female Yorkshire porcine models weighing between 35 and 40 kg were prepared. The laterality of the ureter that served as the control arm was randomized according to a computer-generated number. The contralateral ureter of the same porcine model served as the experimental arm. Anesthesia, experimental procedure, and UASIF measurements were all performed in the same manner as in the pilot study. As shown in Table 2, results were in accordance with those obtained in the pilot study, with a median percent reduction in the maximal UASIF of 37.0% (interquartile range 21.4–44.2).
Randomized, Case-Controlled Study Results of Maximal Ureteral Access Sheath Insertion Force and Percent Reduction at a Vibration Amplitude of 0.04 g and Frequency of 18,000 Hz
IQR = interquartile range.
Pathologic evaluation
Pathologic evaluation of the resected ureters revealed low-grade injury (G0 and GI) in 91.7% (11/12) of the ureters in both groups. The proportion of mucosal injury (≥GII) between the control and experimental group was comparable (p = 0.656; Table 3 and Fig. 4).
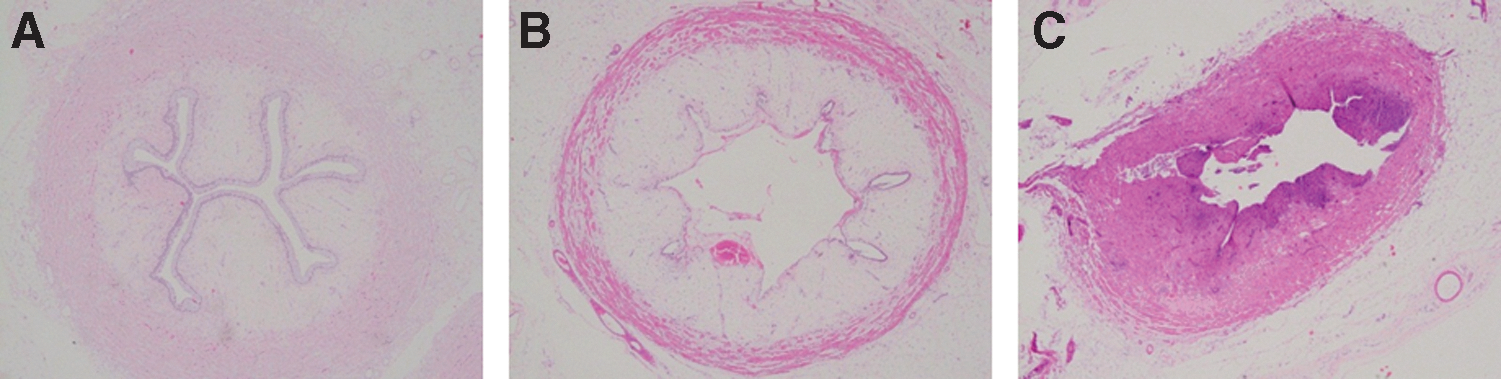
Pathologic analysis of ureteral injury caused by UAS insertion.
Pathologic Evaluation of Ureteral Injury
Ureteral injury (GII) occurred in one control ureter and one experimental ureter, both from a single porcine model (model No. 10). This model had the lowest weight among all pigs used in this study. Considering that the maximal UASIFs observed in this model were exceedingly higher than those of the other models (Table 2), we may presume that the injury was due to an excessive bulking force related to the relatively small diameter ureters, rather than from the transduction of ultrasonic vibration.
Discussion
Under the hypothesis that ultrasonic vibration applied to a sliding surface of a moving object reduces the effective friction, our experimental study is the first to demonstrate that ultrasonic longitudinal-axis vibration transduced onto the UAS may reduce the maximal UASIF. Clear advantages in reduction of the UASIF were seen in the application of vibration at a frequency of 18,000 Hz and amplitude of 0.04 g. The results of the ex vivo and animal experiments differed in the degree of friction reduction with respect to frequency, probably due to differences in the frictional conditions of the UAS and the ureter.
The sliding friction between contacting surfaces can be reduced when ultrasonic vibration is superposed on the macroscopic sliding velocity.
13
This phenomenon forms the basis for several processes of ultrasonic machining to improve the performance of machining tools and workpieces.
14,15
When vibration acts longitudinally to the sliding direction in a plane containing the interacting surfaces, the friction reduction can be explained in terms of changes in vibration amplitude, frequency, and the sliding velocity vector:
10
where F 0 is the frictional force in the absence of vibration, Fa is the frictional force with vibration. Fa can be reduced with increasing amplitude (a) and frequency (ω). Notably, a higher velocity vector of the sliding object (Vs ) results in a greater resultant frictional force (Fa ).
The effect of ultrasonic vibration on reducing friction has been studied in medical devices, primarily needle insertion devices. 11,16,17 Yang and Zahn developed a hypodermic needle coupled with an actuator exerting a vibration amplitude of 0.6 mm. 17 Skin penetration from excised animal tissue showed a 70% reduction in insertion force. Similarly, Tan and colleagues developed a model to explore the effect of ultrasonic amplitude on the needle–tissue interaction force. 11 Maximal puncture force and frictional force depended on the vibratory amplitude and resulted in maximal reductions of 60.8% and 80.7% in puncture force and friction force, respectively. The experiments were performed at a frequency of 20 kHz, while amplitude settings were modified. Considering that high amplitudes may induce ureteral injury, we limited our amplitude to 0.08 g and attempted to reduce the UASIF by varying the frequency settings.
We acknowledge that the degree of maximal UASIF reductions observed in our study were relatively lower than those previously reported. Unfortunately, the upper frequency limit of our electromagnetic exciter was 18 kHz. Considering that Huang and colleagues demonstrated maximal reduction in needle insertion force at frequency settings up to 121 kHz, we believe there is still scope for further reductions in the UASIF with unidentified vibration settings. 16 Furthermore, friction depends on the properties of the sliding surface. 16 Porcine ureters have a tortuous course and are incompletely fixed within the retroperitoneum. Therefore, it is presumable that differences in tissue properties may have attributed to the lower efficacy of ultrasonic vibration transduction and subsequent lower reductions in the UASIF observed in the present study compared with those in previous studies.
The strength of this study is the implementation of a randomized controlled study design, with an objective measurement tool to enable uniform reporting of outcomes. Moreover, the concept of our device is potentially applicable to various medical devices that require a reduction in insertion friction, such as percutaneous nephrostomy and endoscopic devices.
Our study also has limitations. First, the magnitude of the sliding velocity may have affected UASIF measurements as the vibration was applied parallel to the direction of UAS placement. As can be inferred from the analytical model of friction reduction, higher UAS insertion velocity (Vs ) may have resulted in a greater resultant frictional force (Fa ). 10 Although experiments were performed by a single surgeon in a uniform manner, variations in the velocity of UAS insertion may have affected our results. To preclude this potential bias, the duration of UAS insertion was compared between the control and experimental ureters (3.56 ± 0.07 seconds vs 3.37 ± 0.06 seconds; p = 0.172). Considering that all porcine models weighed between 35 and 40 kg, it may be presumed that the lengths of the ureters were comparable between the two groups, which provide evidence that there were no significant differences in insertion velocity. Second, potential damage to the surrounding organs and the long-term safety on the ureter have not been demonstrated. Third, due to the external attachment and limited vibration transmissibility of the UAS, the amplitude of the longitudinal vibration may gradually decrease along the UAS. However, the positive results of our study imply that the vibration generated by the exciter does not have to be fully transduced to the UAS if the amplitude of vibration is large enough to offset the transmission loss. Finally, unidentified ranges of amplitude and frequency of vibration may exert further reductions in the UASIF. Moreover, porcine ureters have a tortuous course and are wider in diameter than are the human ureters. Therefore, further studies with various vibration settings in the human ureter are warranted.
Conclusions
The application of ultrasonic longitudinal-axis vibration onto the UAS may reduce frictional force between the UAS and the ureteral mucosa, and consequently decrease the maximal UASIF. Insertion velocity of the UAS is a potential surgeon-modifiable factor that may further reduce the UASIF. Our apparatus would be applicable to future investigations to aid in identifying factors that will predict effective UAS placement and to provide a cornerstone for safe and effective retrograde intrarenal surgery.
Footnotes
Acknowledgment
This study was supported by a faculty research grant of Yonsei University College of Medicine (6-2017-0147).
Author Disclosure Statement
No competing financial interests exist for all authors.