
Abstract
Background:
The da Vinci Surgical System has led to a rapid growth in the volume of robot-assisted surgeries, with 877,000 surgeries performed in 2017. Despite the increasing prevalence of robotic urologic surgeries, few long-term studies exist that examine trends in reported adverse events (RAEs). We analyzed RAEs over the past decade.
Materials and Methods:
We extrapolated all entries from the Manufacturer and User Facility Device Experience (MAUDE) database with the manufacturer “Intuitive Surgical” from 2007 to 2017. Reports were analyzed for date and type of RAE (death, bodily injury, malfunction, and other). RAEs from urologic surgeries were analyzed further for specific information pertaining to death, bodily injury, and malfunction.
Results:
A total of 19,783 RAEs were analyzed. Instrument or robot malfunctions comprised the majority of RAEs (84.9%); bodily injuries comprised 8.2%. Death was the least common RAE (1.3%). RAEs for urologic robotic surgeries peaked in 2013 and 2014 and decreased since. A total of 69 (2.3%) deaths, 364 (12.2%) injuries, and 2544 (85.5%) instrument or robot malfunctions occurred. No reported deaths were attributed to system or mechanical malfunction, but rather to medical complications reported to be unrelated to surgery. The most common injuries were bowel (22.3%) and genitourinary (GU) (19.5%). Instrument malfunctions caused 16.8% of bodily injuries.
Conclusions:
RAEs for robotic urologic surgeries peaked in 2013 to 2014, and have decreased annually since. When malfunctions occurred, they did not result in death and infrequently resulted in bodily injury. Potential quality improvement targets include prevention of bowel and GU injuries through surgical coaching, and improved technology to prevent malfunction of the surgical system and instruments.
Introduction
Since its U.S. Food and Drug Administration (FDA) approval in 2000, Intuitive Surgical, Inc.'s da Vinci Surgical System has led to a rapid growth in the volume of robot-assisted surgeries, with 877,000 surgeries performed worldwide in 2017 (Annual Report, da Vinci Surgical). 1 The da Vinci Surgical System is currently approved for use in multiple surgical specialties, including urology, gynecology, general surgery, cardiothoracic surgery, and otolaryngology. Several advantages have been proposed with its use, the most well established and accepted of which being decreased blood loss 2 and reduced postoperative pain compared with open surgery. 3 Despite these advantages, robot-assisted surgeries are not without risk and are a relatively newer technology compared with laparoscopic and open surgical techniques.
Previous studies have analyzed robotic malfunctions and reported adverse events (RAEs) in robotic surgery using the FDA's Manufacturer and User Facility Device Experience (MAUDE) database. RAEs in the MAUDE database comprise any device-related adverse event that occurs over the course of a surgery, including instrument malfunctions or failures, device-related injury or death to the patient, and device failures that lead to surgical complications, such as conversion to the open approach or aborting the surgery altogether. A study by Alemzadeh et al. showed that surgical subspecialties that perform high-volume robotic surgery, such as urology and gynecology, experience fewer injuries, deaths, and conversions to open surgery. 4 Another study found that newer surgical systems and increased robotic experience led to fewer open conversions. 5 A smaller, short-term study found that the majority of RAEs were instrument malfunctions. 6 Despite the increasing prevalence of robotic surgery in urology, few long-term studies exist that examine trends in RAEs in robotic urologic surgeries.
The FDA's MAUDE database is a postmarket surveillance database of suspected device-associated deaths, serious injuries, and malfunctions that are reported by mandatory and voluntary reporters. Few long-term studies exist that examine trends in RAEs. We analyzed RAEs over the past decade to determine whether their cause was device or surgeon-specific.
Materials and Methods
Adverse events exported from MAUDE database
After obtaining institutional review board approval, data on RAEs in patients undergoing surgery with da Vinci Surgical Systems from 2007 to 2017 were searched using the MAUDE database. All RAEs from the manufacturer “Intuitive Surgical” from January 1, 2007, to December 31, 2017, were exported for analysis. This included RAEs from all products from Intuitive Surgical, Inc., including da Vinci Surgical system, da Vinci Xi, and da Vinci Si System. RAE type was determined from the MAUDE database classification and report text, with outcomes of interest being patient death, patient injury, and robot malfunction. The RAE type was reclassified based on report text if appropriate. Report text was used to determine whether an RAE met criteria for several event types. Duplicate entries were removed from analysis. The average number of days between RAE date and report filing date was 76 days.
Data analyses
A total of 21,045 adverse events were reported from 2007 to 2017 (Fig. 1). Of those, we excluded 1262 RAEs with no event date provided. This resulted in a sample of 19,783 RAEs. RAEs were then sorted by year and adverse event classification type, specifically, death, bodily injury, instrument or robot malfunction, or other. The designation “other” was given to reports that did not include a death, bodily injury, or instrument or robot malfunction. Total volume of robot-assisted surgeries by year was obtained from Intuitive Surgical, Inc.'s Annual Reports, and used to calculate RAEs rates per 100,000 surgeries per year. Data for total volume of robot-assisted urologic surgeries or specific types of urologic surgeries (prostatectomies, nephrectomies, etc.) are not published by Intuitive Surgical or any other source to our knowledge, thus we were unable to calculate RAE rate per 100,000 surgeries per year.
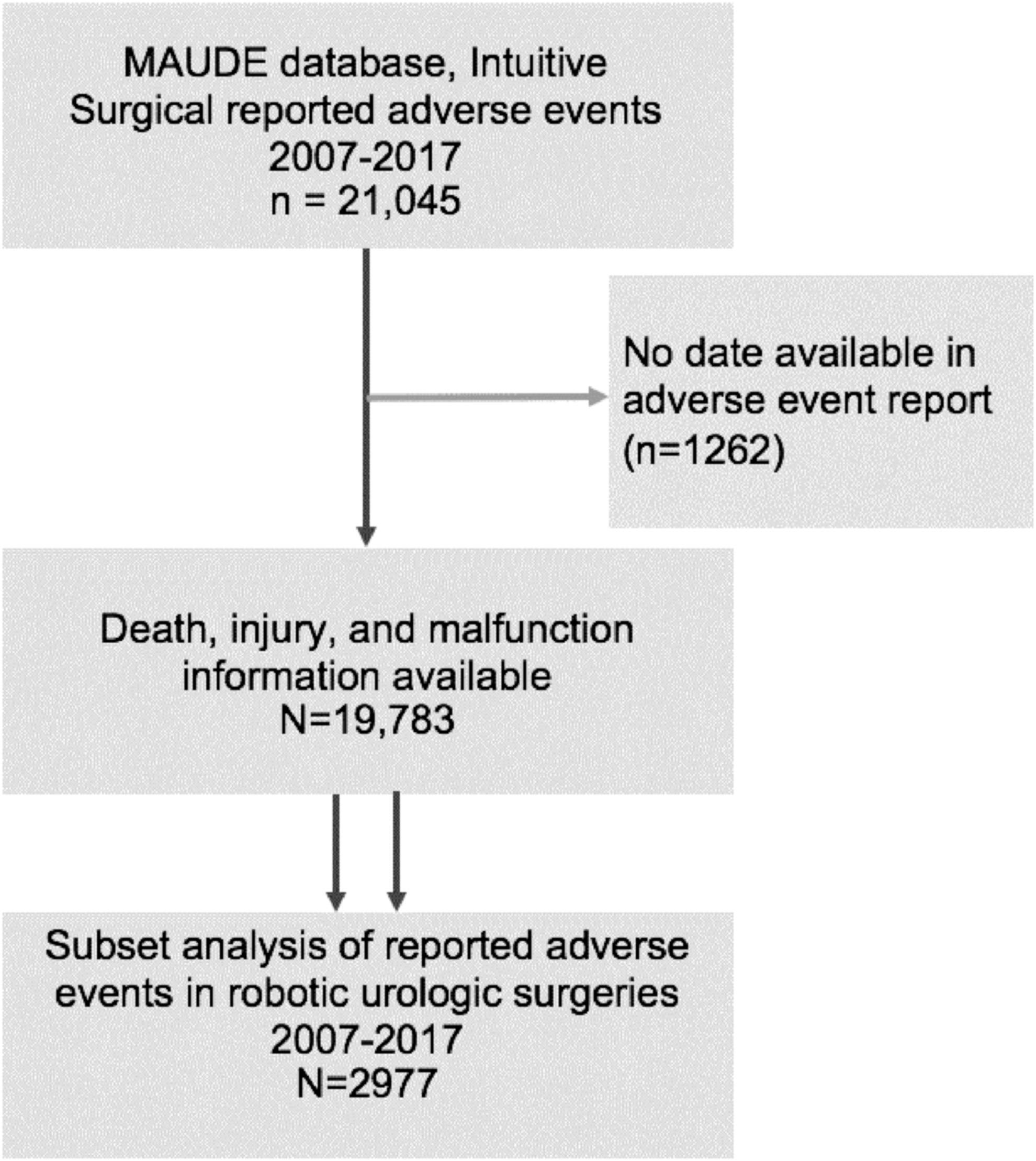
RAE consort diagram. RAEs in patients undergoing surgery with da Vinci Surgical Systems from 2007 to 2017 were identified in the MAUDE database. Reports with missing date or unspecified adverse event information were excluded. A separate subset analysis was then performed on RAEs in urologic surgeries. MAUDE = Manufacturer and User Facility Device Experience; RAEs = reported adverse events.
In-depth analysis of robotic urologic surgeries was performed on RAEs from 2007 to 2017, specifically, prostatectomy, cystectomy, partial nephrectomy, and radical nephrectomy. Specific bodily injury and malfunction information was obtained from report text. A total of 2977 RAEs in urologic surgeries met the aforementioned criteria and were included for analysis.
Results
Baseline trends in overall RAEs in robotic surgery
The total number of surgeries utilizing da Vinci Surgical Systems has steadily increased each year, with a nearly 10-fold increase in surgeries performed robotically from 2007 to 2017 (Fig. 2). Instrument or robot malfunctions comprised the overwhelming majority of RAEs during that time period, comprising 84.9% of all RAEs (Fig. 3). Bodily injury was the second most common RAE (8.2%), whereas death was the least common reported outcome (1.3%).
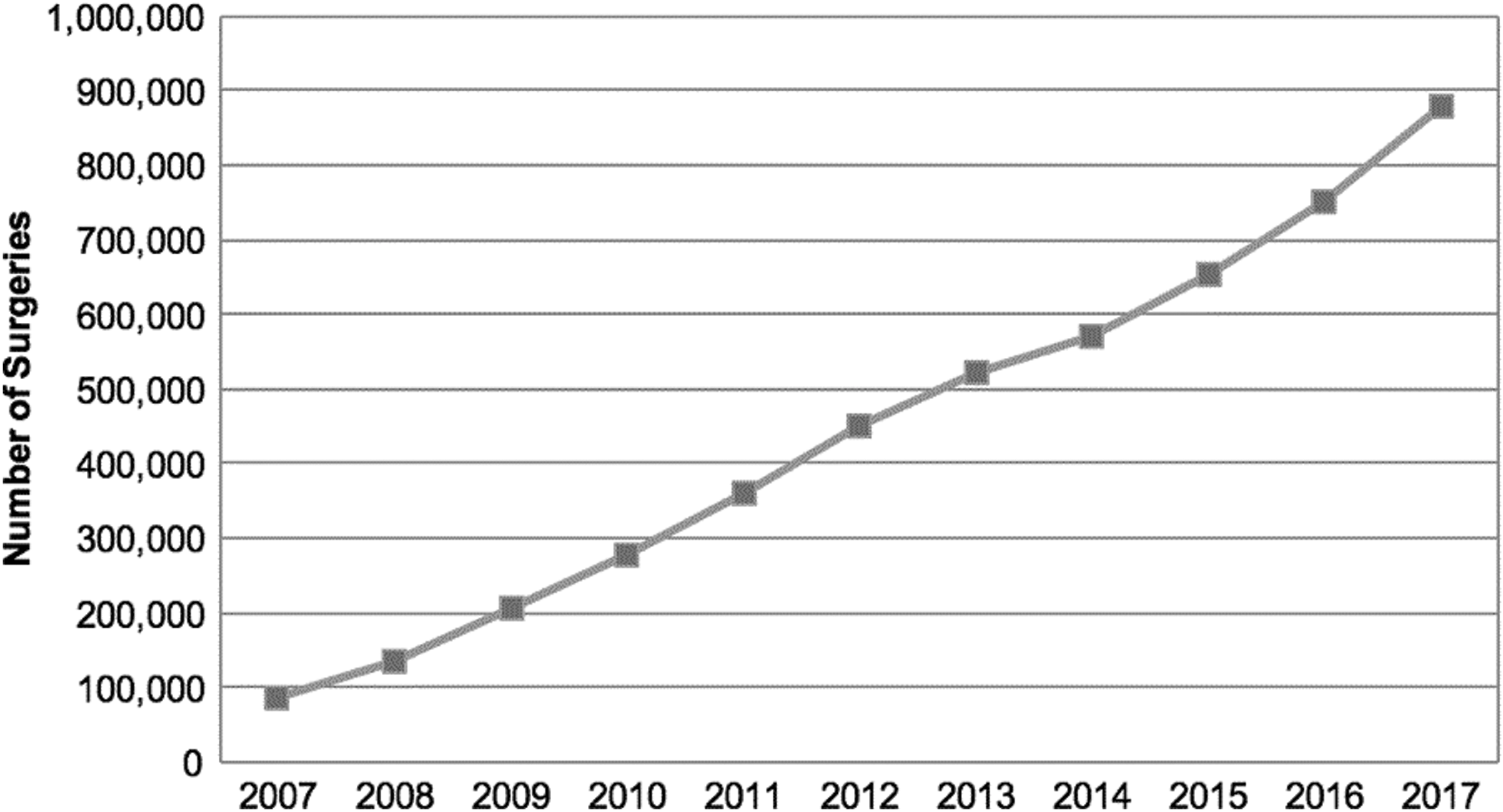
Total number of surgeries using da Vinci Surgical Systems by year. Total volume of robot-assisted surgeries by year was obtained from Intuitive Surgical, Inc.'s Annual Reports.
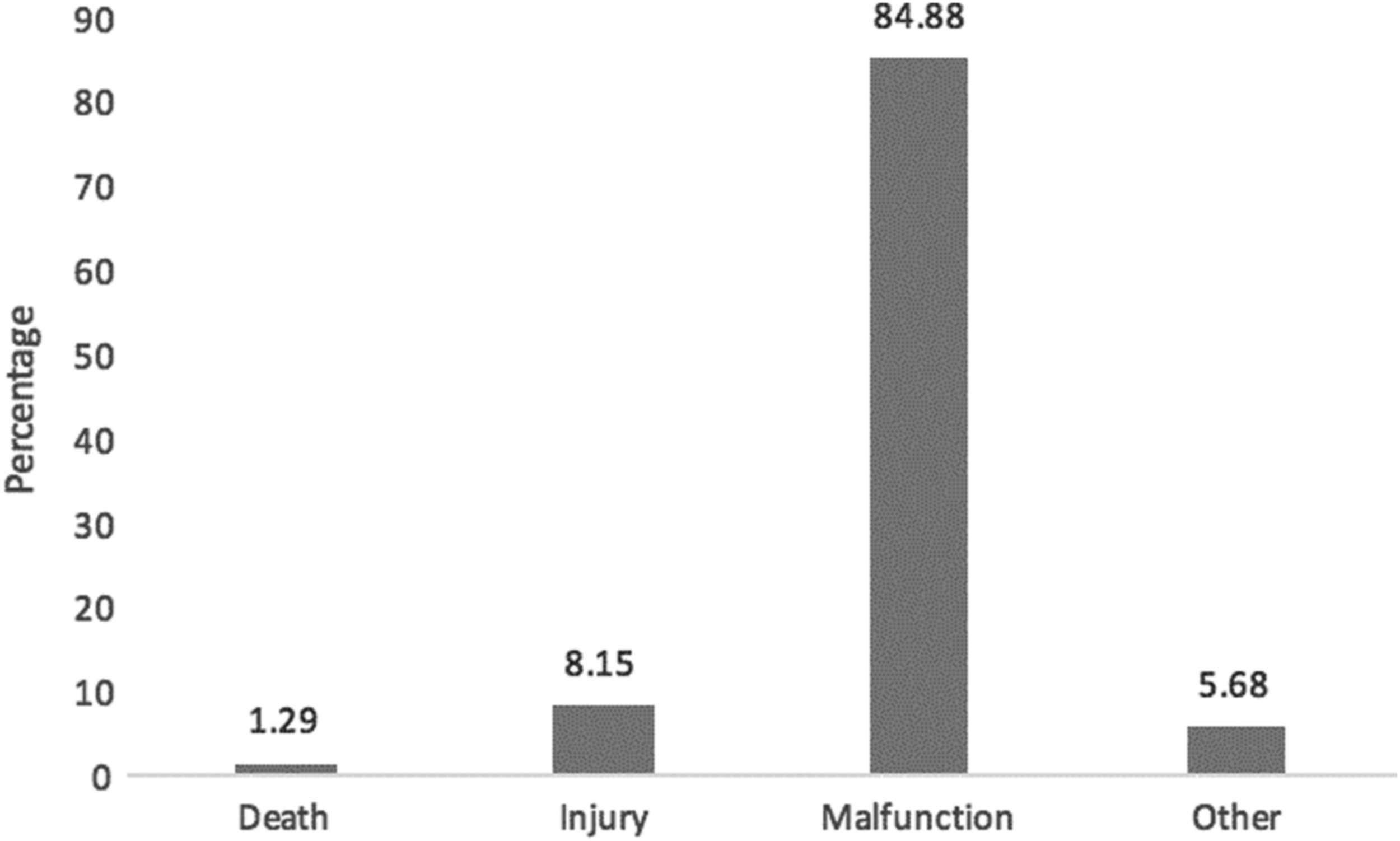
Classification of RAEs by type of event. Instrument or robot malfunctions comprised the majority of RAEs (84.9%). Injuries comprised 8.15% of RAEs, whereas death was the least common reported outcome (1.3% of RAEs). RAEs that did not include death, injury, or instrument or robot malfunction comprised 5.7%.
Rate of overall RAEs as a function of time
With the exception of 2012 to 2014, the rate of RAEs has remained fairly stable over time, despite the annual increase in the number of robotic surgeries (Fig. 4). Adjusting for case volume underscored these data trends. From 2007 to 2011, there were <360.0 events per 100,000 surgeries per year. This number increased to 486.9 events per 100,000 surgeries in 2012, and peaked in 2013 and 2014, with 1121.6 events and 1081.6 events per 100,000 surgeries per year, respectively. The rate substantially declined in 2015, reaching 226.7 events per 100,000 surgeries, and continued to decline in 2016 and 2017. Interestingly, 2017 reflects the lowest RAE rate in the past decade (62.6 events per 100,000 surgeries).

da Vinci Surgical Systems rate of RAEs. Rates of events per 100,000 surgeries were calculated using the case volume reported per year. The overall rate of events per 100,000 surgeries peaked in 2013 and 2014 (1121.6 events and 1081.6 events per 100,000 surgeries, respectively), and reached the lowest rate in the past decade in 2017 (62.6 events per 100,000 surgeries). A peak in reported deaths (12.0 per 100,000 surgeries) and injuries (70.4 per 100,000 surgeries) was seen in 2012. Instrument and robot malfunctions peaked in 2013 and 2014, both with >1000 events per 100,000 surgeries. The year 2017 reflects the lowest rate of death (0.8 per 100,000 surgeries), injury (11.2 per 100,000 surgeries), and reported instrument or robot malfunctions (50.5 per 100,000 surgeries) in the past decade.
The rate of reported instrument or robot malfunctions peaked in 2013 and 2014 with 1033.5 events and 1027.4 events per 100,000 surgeries, respectively, and declined to 50.5 events per 100,000 surgeries in 2017, the lowest value in the past decade. The rate of reported injuries also peaked in 2012 with 70.4 per 100,000 surgeries and declined to 17.6 and 17.8 in 2015 and 2016, respectively, reaching the lowest rate in the past decade in 2017 (11.2 per 100,000 surgeries). Finally, the rate of reported deaths peaked in 2012 with 12.0 deaths per 100,000 surgeries and declined to 0.8 deaths per 100,000 surgeries in 2017, the lowest rate in the past decade.
RAEs in robot-assisted urologic surgeries
Of the 2977 total RAEs in urologic surgeries from 2007 to 2017, RAEs were highest in prostatectomies (74.0% of RAEs), followed by cystectomies (17.2%) and partial nephrectomies (8.3%) (Table 1). Radical nephrectomies comprised the lowest number of RAEs (0.4%).
Reported Adverse Events in Urologic Surgeries 2007 to 2017
Bold values indicate statistical significance.
A total of 2977 RAEs occurred during this timeframe. Data were analyzed by injury type, malfunction type, year, and type of urologic surgery. Instrument or robot malfunction comprised the majority of RAEs (85.5%), followed by injury (12.2%) and death (2.3%). RAEs were overwhelmingly from prostatectomy (74.0%), followed by cystectomy (17.2%). RAEs peaked in 2013 and 2014, and reached the lowest value since 2007 in 2017, despite an annual increase in robotic urologic surgeries.
DVT = deep vein thrombosis; GU = genitourinary; RAEs = reported adverse events.
Trends were then examined by year of surgery. The number of RAEs remained stable from 2007 to 2012, with <7% occurring per year (Table 1). Similar to overall rates of RAEs already discussed, there was a spike in the number of RAEs in urologic surgeries from 2013 and 2014, with nearly 30% of RAEs occurring during each of those years alone. RAEs decreased significantly in 2015 (7.3%), with a steady decline occurring since. The number of RAEs in 2017 (2.8%) was nearly identical to that in 2007 (2.8%), the lowest values seen throughout the time period analyzed, despite an annual increase in the number of robotically performed urologic surgeries.
Similar to RAE trends seen overall in all robot-assisted surgeries, instrument or robot malfunctions comprised the overwhelming majority of events (85.5%), followed by bodily injury (12.2%) and death comprising the smallest fraction (2.3%) (Table 1). There was no evidence of system or mechanical malfunction upon review of the listed events leading to the 69 reported deaths.
We then sought to perform a detailed analysis of the root causes of the types of RAEs in urologic surgeries and the consequences to the patient. Of the 364 reported injuries, an analysis of the RAE report showed that 61 (16.8%) were explained by foreign bodies becoming dislodged into the patient secondary to instrument malfunctions (Table 1). When surgical error occurred, the most common bodily injury reported was bowel injury (22.3%) followed by genitourinary (GU) injury (19.5%) and vascular injury (12.6%). Nerve injury secondary to patient positioning, compartment syndrome, skin burns, fistula formation, and deep vein thrombosis comprised the lowest percentage of RAEs (2.5%, 1.7%, 1.4%, 0.8%, and 0.6%, respectively).
Further analysis of instrument or robot malfunction reports was then performed. We found that of the 2544 RAEs caused by instrument or robot malfunction, only 25 cases (1.0%) were converted to open surgery, 32 cases (1.3%) were converted to laparoscopic surgery, and 20 cases (0.8%) were aborted (Table 1). Of the instrument and robot malfunctions, surgical system errors comprised the majority (21.8%), followed by malfunctions with prograsp forceps (16.3%), monopolar curved scissors (15.6%), Maryland bipolar (12.3%), and fenestrated bipolar (11.7%). Trocar malfunctions comprised only 3.3% of malfunctions. The lowest percentage of malfunctions was seen in the crocodile grasper (0.8%), tenaculum forceps (0.5%), and robotic harmonic instrument (0.4%).
Discussion
Robot-assisted surgeries are becoming increasingly prevalent in urology and other surgical fields, with a 10-fold increase in surgeries performed using da Vinci Surgical System in the past decade. Although robotic surgeries pose numerous potential advantages over open and laparoscopic approaches, robotic surgeries carry risk of surgical error in addition to instrument or robot malfunction. Among all robotically performed surgeries and in urologic surgeries specifically, instrument or robot malfunctions comprise the overwhelming majority of RAEs, followed by bodily injury and death in a small minority of RAEs. We found that in the past few years, there has been a substantial decrease in the rate of RAEs (deaths, injuries, and malfunctions) associated with robot-assisted surgeries, with rates of RAEs in urologic surgeries reaching the lowest values in the past decade, despite the increase in the number of robotic surgeries performed. Overall, our results suggest that safety and training in robotic surgery have improved among urologists. However, it is possible that increases in adverse events may occur in the future as additional surgical specialties incorporate robotic technology.
The number of RAEs for robotic urologic surgeries peaked in 2013 and 2014, and there has been a substantial decrease in reported deaths, injuries, and malfunctions since. In our analysis, we found an average of 76 days between event date and RAE filing date, suggesting that this decrease is not because of RAEs that have not yet been reported. Rather, this decrease in RAEs can be explained by a presumed increase in surgical skill with the robotic system by surgeons and staff, particularly as the case volume of robotically performed surgeries increases. In addition, proficiency with robotic surgery is now a focus for many training programs, with residents and fellows gaining more experience operating robotically during their training. Finally, our decade-long analysis includes the advent of several models of da Vinci Surgical System, suggesting that newer robot models with software and hardware upgrades may be able to better optimize surgeries and minimize previously seen errors. It is also possible that rates of MAUDE reporting in 2013 to 2014 were particularly high because of secular trends. Specifically, MAUDE reporting and lawsuits related to vaginal mesh also peaked in this time period. 7 In addition, high-profile medical malpractice cases occurred around this time. 8,9 These litigation cases may have contributed to the increased MAUDE reporting of da Vinci-related events during that specific time period.
Our detailed analysis of RAEs in urologic surgeries showed that surgical error resulted in the majority of injuries, the most common of which being bowel injury, GU injury, and vascular injury. Such injuries are well known to occur with open and/or laparoscopic approaches, and it cannot be discerned whether these complications were increased, or decreased, by the use of the robot. Our findings are also consistent with previous studies, showing that the majority of RAEs are the result of instrument malfunctions. 6 Interestingly, only a small minority of injuries were caused by foreign body dislodgment secondary to instrument malfunction. Fortunately, such malfunctions did not appear to significantly compromise patient safety. Robot malfunctions were mainly from the surgical system, prograsp forceps, and monopolar curved scissors. Robot malfunctions rarely led to conversion to open surgery, laparoscopic surgery, or procedure abortion, and there was no report of robot malfunction causing patient injury. These findings suggest that potential targets for quality improvement include increased surgical training specifically targeting prevention of bowel and GU injuries, as well as technological advances to prevent malfunction of the surgical system, with potential targets being the prograsp forceps and monopolar curved scissors. However, given that we do not know the frequency with which the prograsp forceps and monopolar curved scissors are used in each surgery, it is possible the higher incidence of RAEs citing those instruments is proportional to their level of use. In addition, it is possible that engineering hurdles have prevented technological advances with these instruments, or in the case of the sheath, the additional step of placing an insulating sheath may lead to more reporting errors or instrument failures. Larger studies examining surgeon skill level and technological advances and their correlation with patient injury and malfunction rate, respectively, are needed to validate these findings.
Our study is a long-term comprehensive analysis of all RAEs in robotic surgeries. Access to individual reports enabled a thorough analysis of RAEs in robotic urologic surgeries. In addition, the MAUDE database comprises all FDA reports received by mandatory and voluntary reporters, enabling access to all available RAEs. However, several limitations of this study result from the use of the MAUDE database. MAUDE is a passive surveillance system that relies entirely on third-party reporting. Thus, it is possible that RAEs are under-reported and variably reported. Reporting to the FDA may be done by different types of health professionals at each hospital, ranging from surgeons to nurses or surgical assistants, which may contribute to variable reporting. In addition, RAEs in the MAUDE database may be incomplete, inaccurate, unverified, biased, or untimely, thus potentially skewing our findings. In addition, surgeons are not individually identified in reports, preventing analysis of surgeon experience as a causative factor in RAEs. In addition, owing to variable information included in each report, we could not analyze trends in the various iterations of the da Vinci robot system, as the specific robot type was not always included in reports. Despite these limitations, MAUDE remains the most comprehensive reporting system of RAEs for robotic technologies.
Conclusions
Although robotic surgery is increasing in prevalence in numerous surgical fields, it is imperative to understand trends in RAEs to identify areas of potential surgical training and technological targets to prevent adverse patient outcomes. Our analysis of RAEs over the past decade suggests that overall there has been a decrease in all RAEs in robotic urologic surgeries and surgeries in all fields. Instrument or robotic malfunctions did not result in death and infrequently resulted in bodily injury. These findings suggest that over the past decade, there have been improvements in the safety and training in robotic surgery among urologists and possibly other surgical fields who adopted this technology during the same timeframe. Potential areas of improvement include surgical training to prevent bowel and GU injuries, and technological improvements in the surgical system, prograsp forceps, and monopolar curved scissors to help prevent the most common bodily injuries and malfunctions reported. Larger studies with long-term follow-up are needed to validate these findings.
Footnotes
Author Disclosure Statement
No competing financial interests exist.