
Abstract
Introduction:
Reducing fluoroscopy time (FT) during percutaneous nephrolithotomy (PCNL) is an opportunity for stewardship of ionizing radiation in stone patients. We present our initial results of a radiation reduction protocol (RRP) used during PCNL with fluoroscopy-guided access by the urologist.
Materials and Methods:
Retrospective chart review of all PCNL cases performed between January and October 2017, divided in two groups: pre-RRP (group 1) and post-RRP (group 2). Fluoroscopy was performed using low-dose and pulsed mode. Measures implemented to reduce FT include (1) one-spot images, (2) reliance on tactile feedback, and (3) using shorter segments of live fluoroscopy. The primary outcome was FT.
Results:
Eighty-nine PCNL procedures were performed in 89 patients, 45 in group 1 and 44 in group 2. Overall median (interquartile range) age, body mass index (BMI), and stone burden (largest axial diameter) was 56 (45–66) years, 31.3 (27–37.4) kg/m2, and 27.7 (19–41) mm, respectively, and were comparable in both the groups. The median (range) FT in group 1 and group 2 was 240 (56.0–916.0) and 65.5 (13.0–561.0) seconds (p < 0.0001), respectively. There was no correlation between FT and increasing BMI and stone burden. Overall stone-free rate was 57% (58% and 57% in group 1 and group 2, respectively, p = 0.5995), with 10 patients (11%) undergoing ancillary procedures. Overall and major (Clavien 3a+) complications occurred in 10 (11%) and 5 (6%) cases, respectively, in the overall cohort.
Conclusion:
FT in PCNL can be significantly reduced by adapting simple techniques and being increasingly vigilant of its usage, thereby reducing radiation exposure to the surgeon and the patient.
Introduction
The prevalence of stone disease in the United States continues to grow, affecting ∼1 in 11 Americans. 1 Percutaneous nephrolithotomy (PCNL) is the preferred surgical treatment option for large or complex stone burden. Most urologists in North America who obtain their own access and perform PCNL learned to do the procedure using fluoroscopy, which provides information on the renal anatomy, proper positioning of surgical devices, and measurement of the remaining stone burden. Fluoroscopy is a form of ionizing radiation, and its cumulative effects can potentially lead to the development of solid or hematologic malignancies, skin injury, or accelerate degenerative processes such as cataracts. 2
There has been increasing vigilance and interest in lowering ionizing radiation dose in the surgical management of stone disease, particularly during PCNL. Indeed, the “ALARA” principle in fluoroscopy (As Low As Reasonably Achievable) has become a guiding principle to most endourologists treating stone disease. In one study, the estimated mean radiation dose to a patient undergoing a PCNL with a mean fluoroscopy time (FT) of 12 minutes is 7.3 mSv and to the physician is 12.7 μSv. 3 Patient's body mass index, quantitative stone burden, nonbranched stone configuration, and number of percutaneous tracts have been shown to correlate with increased radiation dose. 4
Although it is important to reduce the radiation for the patient undergoing the PCNL, it is of even more importance to reduce the radiation dose to the urologist who is performing several PCNL procedures over time. Although several strategies have been proposed in the literature to help reduce radiation dose, one very practical way to reduce occupational radiation exposure is reducing total FT. 5,6
We have implemented a radiation reduction protocol (RRP) to reduce FT in each step of the PCNL procedure and have as a result become increasingly aware of our FT during PCNL. The objective of this study was to show that the FT in PCNL can be significantly reduced through simple techniques implemented throughout key steps of the procedure and that this can be safely achieved without compromising perioperative outcomes.
Materials and Methods
Patient selection and evaluation
The study received an institutional review board approval (study no. 2017H0393) on October 30, 2017. We performed a retrospective chart review of a prospectively maintained database of all PCNL cases performed between January 1, 2017, and October 30, 2017. The cohort was divided in two groups: group 1 (pre) and group 2 (post) based on the cutoff date of June 1, 2017, when our new RRP was implemented. Inclusion criteria were age >18 years and PCNL performed between the above dates. Simultaneous bilateral procedures were excluded. All patients underwent a noncontrast CT before surgery. Access was obtained by the urologist in almost all cases using an 18-gauge needle (Cook Medical, Bloomington, IN) aimed at the calix of interest and advanced at end-expiration when the kidney is immobile under fluoroscopic guidance. The tract was dilated using a Bard (Bard Medical, Covington, GA) balloon (24F or 30F) and the nephrostomy access sheath placed over the balloon. PCNL was then performed using a conventional 24F rigid nephroscope. The ShockPulse-SE (Olympus, Center Valley, PA) was the most commonly used lithotripter. Most patients had a 7F ureteral stent and a Foley catheter placed at the end of the procedure.
Fluoroscopy/fluoroscopy reduction protocol
A General Electric 99 OEC C-arm (General Electric Healthcare, Boston, MA) was used for all cases. Fluoroscopy technicians varied for each case; however, most had some experience with our PCNL procedure. No foot pedal was used. Fluoroscopy was performed using low-dose (50% reduction in milliamperage, variable peak kilovoltage (KVP) depending on body habitus) and pulsed mode (four frames per second) whenever feasible. Specific measures implemented to reduce FT during key steps in PCNL are outlined in Figure 1. These included using more “one-spot” images instead of “live” fluoroscopy and an increased reliance on tactile feedback. Examples include gently advancing the wire down the ureter to the bladder until it cannot advance further (at this point taking a one-spot image at the bladder to confirm its appropriate position), or positioning the balloon by tactile feedback first, then using short live-fluoroscopy segments to make the final critical adjustments. With increasing experience, sometimes the initial puncture through the renal capsule and into the collecting system can also be felt. Shorter segments of live fluoroscopy were used, particularly for the initial needle puncture for renal access, and final critical positioning of the balloon dilator and the nephrostomy access sheath.
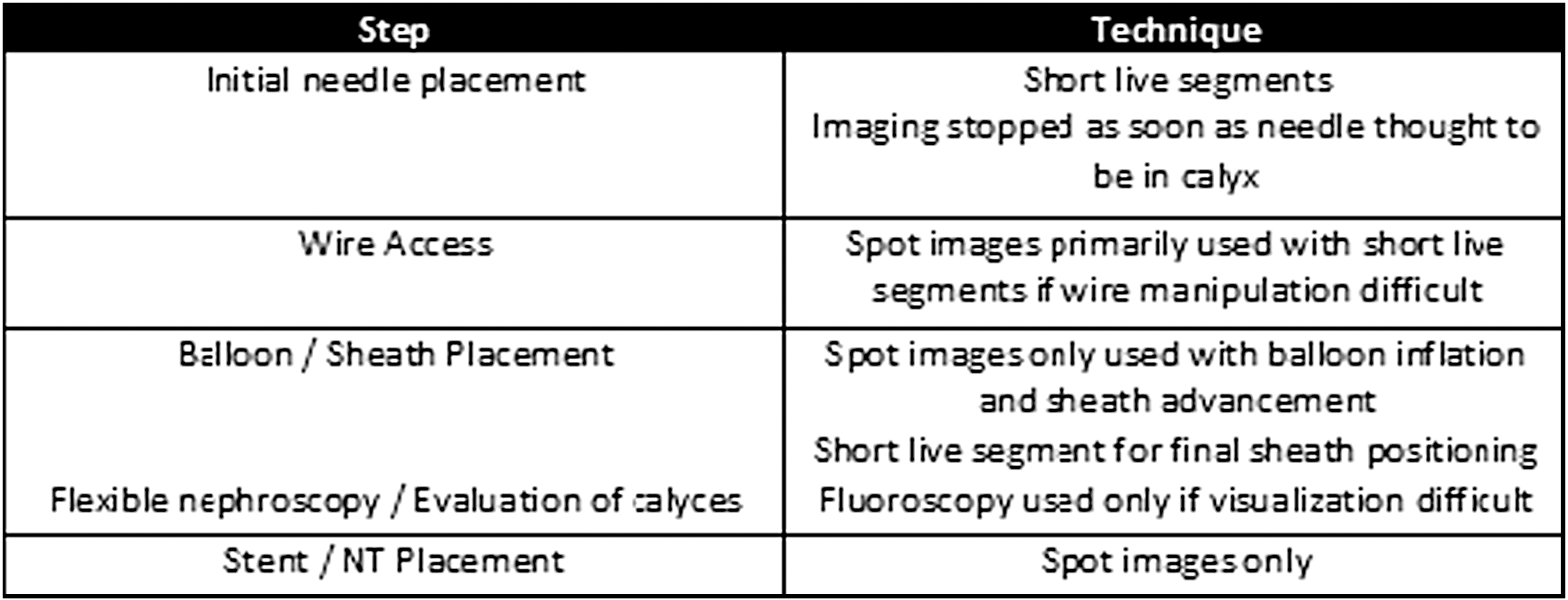
Specific steps with technique to reduce fluoroscopy time.
Statistical methods
Patient demographics, stone characteristics, and perioperative outcomes were summarized using descriptive statistics and compared between group 1 and group 2. Categorical variables were compared between groups using either a chi-square test or Fisher's exact test, and continuous variables were compared with a two-sample t-test/Wilcoxon rank sum test, where appropriate. An analysis of covariance model was used to evaluate the difference in FT between group 1 and group 2, after accounting for associations between FT and body mass index (BMI) and stone burden. All data analyses were performed using SAS 9.4 (SAS Institute, Inc., Cary, NC).
Data
Patient demographics and perioperative outcomes were extracted from the patient charts. Preoperative demographic data collected included age, gender, BMI, prior stone surgery, anatomical abnormalities, laterality, number of stones, and quantitative assessment of stone burden based on largest axial and coronal diameter (or sum thereof if multiple stones). The presence of staghorn formation (defined as occupying >80% of the pelvicalyceal system) was also noted, as was location of the stones. Stone location was divided into five regions: renal pelvis, lower pole, upper pole, interpolar, and ureteropelvic junction. Intraoperative characteristics recorded were FT, number of access tracts, whether or not ureteroscopy was performed, and any complications. Follow-up imaging modality and timing were recorded, along with the assessment of stone-free status (defined as fragments ≥2 mm on any imaging modality) and stone composition. Ancillary procedures and any complications within 30 days were also recorded.
Outcome
The primary outcome of the study was FT. Secondary endpoints were stone-free rate, complications, and need for ancillary procedures.
Results
Eighty-nine PCNL procedures were performed in 89 patients, 45 in group 1 and 44 in group 2. Median (interquartile range) age and BMI of the entire cohort was 56 (45, 66) years and 31.3 (27, 37.4) kg/m 2 , respectively. Both groups were similar with respect to age (p = 0.6252), BMI (p = 0.0822), and stone burden (p = 0.4049). Full staghorns were present in 17 (38%) patients in group 1 and 10 (23%) patients in group 2 (p = 0.1225). Four (9%) patients in group 1 and seven (16%) patients in group 2 had anatomical abnormalities (e.g., horseshoe, duplex kidney, ileal conduit). Baseline characteristics are summarized in Table 1.
Baseline Characteristics Summarized by Group
BMI = body mass index; IQR = interquartile range; URS = ureteroscopy.
Perioperative outcomes are summarized in Table 2. The median (range) FT in group 1 and group 2 was 240 (56.0–916.0) and 65.5 (13.0–561.0) seconds (p < 0.0001), respectively. There was no correlation detected between FT and increasing BMI (group 1: R 2 = 0.08, group 2: R 2 = 0.02) or stone burden (group 1: R 2 = 0.01, group 2: R 2 = 0.08) (Fig. 2).

Association between fluoroscopy time and
Perioperative Outcomes Summarized by Group
Postoperative imaging was available for 79 (89%) patients: CT imaging was used in 27 (34%) patients, and a combination of kidney, ureter, and bladder radiograph and/or ultrasound was used in 52 (66%) patients. Overall stone-free rate was 57% (58% and 57% in group 1 and group 2, respectively, p = 0.5995), with 10 patients (4 and 6 in group 1 and group 2, respectively, p = 0.5151) undergoing ancillary procedures in the overall cohort. Overall complications occurred in 10 patients (3 and 7 in group 1 and group 2, respectively, p = 0.1675). These included severe colic after stent removal (1), acute kidney injury (ACI) (2), contralateral ureteroscopy for stone (1), fever/sepsis (3), bleeding requiring embolization (1), pleural injury requiring chest tube (1), and abdominal fluid collection requiring ventriculoperitoneal shunt exchange (1).
Discussion
PCNL using fluoroscopic guidance is associated with the highest amount of radiation of any endourological procedure. 7 The concern is the possible long-term effects of radiation exposure on the surgeon, medical staff, and the patient during the procedure, which is most commonly performed using fluoroscopic guidance. The “ALARA” principle in fluoroscopy has become a guiding principle to most endourologists treating stone disease. In this study, we were able to reduce FT in PCNL by 75% (240 seconds vs 65 seconds) by implementing simple effective measures including reducing segments of live fluoroscopy and an increased reliance on tactile feedback.
Factors associated with increasing ionizing radiation in PCNL include increased BMI, 4,8 higher stone burden, 4,8,9 nonbranched stone configuration (increasing difficulty to get wire down the ureter), 4 and a greater number of access tracts. 4,8,9 In addition, the effective dose rate was also determined to be higher for a left-sided PCNL compared with a right-sided PCNL (0.021 mSv vs 0.014 mSv). 10 In our series, there was a statistically significant difference in FT between the two groups even after accounting for associations between FT, BMI, and stone burden, suggesting that these measures can be effectively implemented in even more complex stone cases without compromising postoperative outcomes. Due to the small sample size of patients in each group, this study may have been underpowered to detect an association between FT and increasing BMI and stone burden. However, one plausible hypothesis is that even with increasing BMI and stone burden, the principles for obtaining PCNL access remain the same. Although the tract may be longer in patients with a higher BMI, the distance can be traversed with the needle rather quickly to reach the tip of the calix of interest. An increase in total stone burden may increase the total procedural time (increasing time of lithotripsy); however, the renal access and other fluoroscopy-dependent steps of the procedure can still be performed using the RRP. Few cases in the overall series have required multiple tracts (one in group 1 and four in group 2); however, these are too few cases to make any valid conclusions on whether multiple renal tracts increase the total FT. Although there is a tendency for an increased rate of complication in group 2 [7 (16%) in group 2 vs 3 (7%) in group 1], the sample size was likely too small to detect a difference. In addition, these are well-described complications of PCNL (e.g., bleeding, sepsis, pleural injury), and we do not believe that they are a direct result of the implementation of the RRP.
The measures we have implemented are simple and can be easily applied to most PCNL cases. Several studies have explored other strategies to minimize radiation exposure and FT. These include a tighter collimation, 11 using low-dose and pulsed fluoroscopy, 5 the use of a laser-guided beam, 6 a designated fluoroscopy technician, 6 using air instead of contrast during retrograde pyelogram, 12 and the acquisition of as few images as possible during PCNL. In addition, it has been shown that patients with a preoperatively obtained access are usually associated with significantly less FT (36%), although this does require multiple procedures performed on the patient. 13 Interestingly, merely informing the surgeon of their FT can also impact radiation exposure, with a median reduction of total FT by 55% as shown in one study. 7 Any of these strategies, or a combination thereof, can potentially be beneficial to the patients and all medical personnel exposed.
Other techniques have been described to help facilitate access in PCNL in an attempt to further reduce FT usage. In a comparative analysis between endoscopic-guided access vs fluoroscopy-guided access in PCNL, patients undergoing endoscopic-guided access had significantly shorter FT (3.2 minutes vs 16.8 minutes). 14 The FT was similar in a retrospective study evaluating 55 consecutive endoscopic-guided PCNL, with a mean FT of 3.4 minutes. 15 Fluoroscopy may still be utilized extensively in endoscopic-guided access to advance the ureteroscope up to the kidney or to aim at the tip of the ureteroscope with the puncture needle during access. More recently, ultrasound has been described to gain access into the kidney, although the usage of fluoroscopy is still often required for key steps in the procedure. 16 Chu and colleagues demonstrated that the procedure can be performed using fluoroscopy only to confirm the position of the nephrostomy tube placement at the end of the procedure (FT = 17 seconds). 17 The FT for ultrasound-guided access can be quite prolonged (FT >200 seconds) in the learning phases 18 but can be significantly reduced with increasing user experience (FT = 33 seconds) 19 and may even be associated with some cost-savings. 20 In a feasibility study, Alsyouf and colleagues 21 demonstrated a >99% total FT reduction in PCNL cases performed using direct endoscopic visualization combined with ultrasound-guided access (FT = 8.8 seconds). Completely fluoroscopy-free ultrasound-guided PCNL has also been described. 22,23 Although ultrasound-guided access has its inherent advantages, it can be challenging to use ultrasound in several scenarios, including obese patients, 24 nondilated collecting system, 19 and upper pole punctures 19 (due to overlying ribs obscuring the image). Ultrasound-guided access can be difficult to implement in practices with a predominantly obese patient population. Usawachintachit and colleagues demonstrated that ultrasound-guided access was effective in only 45.7% of patients with a BMI >30 kg/m 2,24 which is less than the median BMI of the patients in our current series (32 kg/m 2 ).
The present study has several limitations. First, the study was retrospective in nature with a small sample size. Subjects received treatment in chronological order, and therefore, subjects in group 2 may have benefited from the surgeons' increased experience over time. Moreover, given the retrospective design, the follow-up imaging modality and timing were not standardized in this study. The radiation dose was measured indirectly by FT, and effective radiation exposure from the C-arm or measurements from a dosimeters could have been used for a more direct measure. Finally, this study evaluated FT in adult patients seen at a single institution with a high case volume for stone disease, which may limit its generalizability.
Future prospective studies should continue to explore ways in which FT, and ultimately the cumulative radiation dose, can be reduced during endourologic surgeries. This may include novel applications of technology and also implementing dose reduction protocols earlier on in residency training programs.
Conclusion
A RRP can be easily implemented through simple techniques and by increasing vigilance of FT usage in PCNL. This protocol significantly reduced FT by ∼75% in PCNL procedures and was performed without compromising perioperative outcomes.
Footnotes
Author Disclosure Statement
Dr. Bodo E. Knudsen is a consult for Boston Scientific, Bard, and Olympus. This research was completed without their participation, knowledge, or financial support, and data were acquired and processed by coauthors unaffiliated with any commercial entity. Dr. Michael W. Sourial and Dr. Andrew M. Todd have no disclosures.