
Abstract
Objective:
To determine whether transurethral resection of the prostate (TURP) is safe and effective in patients under ongoing therapeutic oral anticoagulation (OAC) or antiplatelet drug (APD) therapy.
Patients and Methods:
We analyzed data on 276 consecutive TURP patients under ongoing APD therapy with acetylsalicylic acid (n = 130) or clopidogrel (n = 16) or ongoing OAC with phenprocoumon (n = 57), without stopping or bridging the medication, compared to 73 TURP patients without APD/OAC.
Results:
Outcomes of patients under acetylsalicylic acid were comparable to the controls. Under ongoing OAC therapy TURP patients tended to need slightly longer bladder irrigation (median 24 hours vs 22 hours, p = 0.06), needed longer transurethral catheterization (median 42 hours vs 24 hours, p = 0.031), were threefold more likely to have postoperative urinary retention (18% vs 6%, p = 0.04), had slightly longer hospital stays (median 4 days vs 3 days, p = 0.008), and tended to need more blood transfusions (9% vs 1%, p = 0.09), compared to controls. TURP patients under ongoing APD therapy with clopidogrel needed slightly longer bladder irrigation (median 24 hours vs 22 hours, p = 0.006), received more blood transfusions (19% vs 1%, p = 0.017), and had more rehospitalizations (19% vs 3%, p = 0.039). The significant functional improvement 1, 3, and 12 months after TURP was similar in all groups.
Conclusions:
Ongoing APD therapy with acetylsalicylic acid does not significantly impact TURP outcomes in terms of bleeding complications. Patients under ongoing therapeutic OAC with phenprocoumon or APD with clopidogrel can safely undergo TURP with an increased risk of bleeding complications, blood transfusions, and longer hospitalization.
Introduction
Transurethral resection of the prostate (TURP) is the current standard for treating men with bothersome moderate-to-severe lower urinary tract symptoms due to obstructive benign prostatic hyperplasia (BPH) after failure of medical treatment. 1 Patients requiring TURP are elderly, more prone to comorbidities, and are often under oral anticoagulation (OAC) or antiplatelet drug (APD) therapy 2 and, therefore, more likely to suffer from bleeding complications.
There are different options for addressing this issue. If OAC/APD therapy is not mandatory, it can be stopped. If it is necessary for a limited time, TURP can be postponed until that time has expired. However, in some patients stopping OAC/APD therapy is associated with an unacceptable increasing risk of heart complications (e.g., in case of coronary artery disease: threefold; coronary stenting: 90-fold). 3 A third possibility for these patients on OAC is to bridge the OAC during the perioperative period with low-molecular weight heparin (LMWH), which might be advantageous during surgery but has no advantage postoperatively and after hospital discharge when OAC is reestablished. However, a main disadvantage of switching from OAC to LMWH and back is the risk of insufficient or overshooting anticoagulation. Data from implantation of cardiac rhythm devices or similar interventions show that patients are two- to threefold more likely to have bleeding complications under bridging than patients under ongoing OAC. 4,5
The purpose of our study was to compare the safety and effectiveness of bipolar TURP in patients under ongoing APD therapy with acetylsalicylic acid (Aspirin®) or clopidogrel (Plavix®) or OAC with phenprocoumon (Marcoumar®) with TURP in patients without OAC/APD.
Patients and Methods
Study population
We analyzed data on 276 consecutive BPH patients who underwent bipolar TURP at our institution between September 2007 and June 2015 (Ethics Committee approval: 2017–01387). Indications for surgery were based on the guidelines of the European Association of Urology. 1
At the time of surgery, 130/276 patients (47%) were under acetylsalicylic acid 100mg/d (Aspirin; A-group), 57/276 patients (21%) under ongoing therapeutic phenprocoumon (Marcoumar; M-group), and 16/276 patients (6%) under clopidogrel 75mg/d (Plavix®; P-group) and some of them additional acetylsalicylic acid. Of 276 patients, 73 patients (26%) without any OAC/APD therapy served as controls (C-group); this series represents the bipolar TURP group of a former randomized study comparing monopolar vs bipolar TURP. 6 Patients under OAC or APD took their medication before, during, and after surgery, without stopping or bridging their OAC/APD medication.
Patients with known prostate cancer were excluded from the study, but patients with incidentally detected prostate cancer in the resected prostate tissue were retained.
Evaluated data and follow-up
Data evaluated preoperatively included the following: Age, body mass index (BMI), International Prostate Symptom Score (IPSS), Quality of life (IPSL), prostate volume, cystoscopy, urinary flow rate and postvoid residual volume (PVR), routine blood parameters, including hemoglobin, thrombocytes, electrolytes, creatinine, and prothrombin time in relation to the normal population (Quick value), as baseline values.
TURP was performed under general (58%) or spinal (42%) anesthesia—the latter only in patients of the A- and C-group—by 19 different urologists (teaching institution), just 6 urologists performing 70% of the procedures. Perioperatively patients received antibiotic prophylaxis consisting of a single shot of trimethoprim/sulfamethoxazole or targeted antibiotic therapy depending on the result of a preoperative urine culture. For catheter-dependent patients, antibiotic prophylaxis was initiated the day before surgery.
As thromboembolic prophylaxis a weight-dependent dose of LMWH was administered during hospital stay in 91% of all APD and control patients but not the 57 patients under OAC. Perioperative parameters measured included duration of surgery and volume of peri- and postoperative irrigation fluid. All patients remained hospitalized for at least 1 day postoperatively.
Postoperative parameters assessed included duration of irrigation, volume of irrigation fluid, how long catheter was left in place, and blood parameters such as hemoglobin, sodium, and so on. The bladder catheter was removed no sooner than 24 hours after surgery, and as much as 4 hours after irrigation was stopped, the urine in the tube was free of relevant clots and the defined size of a main letter in the newspaper could be read through the draining urine tube.
The day after urinary catheter removal, urinary flow and PVR were evaluated. Patients were discharged if the PVR was less than 100 mL or less than half of the voided volume. If the PVR was elevated, patients were treated with a nonsteroidal anti-inflammatory drug (NSAID) for swollen residual prostate tissue or urethra and with distigmine bromide for impaired contractility of the detrusor muscle.
If the PVR exceeded 300 mL, patients were discharged with either a transurethral or suprapubic catheter; this was removed 2–4 weeks later if PVR was stable or had decreased.
In all other patients follow-up examinations with IPSS/IPSL, uroflowmetry, prostate specific antigen, and PVR levels were scheduled 1, 3, and 12 months postoperatively. The patients were asked for other complications such as urinary tract infections (UTI), bleeding, or cardiovascular events. If the history, IPSS, or uroflowmetry yielded suspicion for urethral stricture (US), bladder neck contracture (BNC), or significant residual adenoma (RA), a cystoscopy was performed.
Early complications were defined as UTI occurring within 30 days postoperatively, bleeding complications as much as 90 days postoperatively, and presentation at the emergency department for any reason related to the TURP. As late complications we defined US, BNC, and recurring lower urinary tract symptoms due to persisting RA occurring more than 3 months postoperatively.
Bleeding parameters were assessed during the postoperative hospital stay and after discharge if patients presented themselves at the emergency department or outpatient clinic. As bleeding complications, we counted: emergency presentation due to hematuria, need of continuous bladder irrigation, clot retention requiring evacuation, need of blood substitution, reoperation for transurethral coagulation, and removal of an organized clot.
Regarding thromboembolic events, patients were screened clinically during their hospital stay, and if there was a suspicion further examinations were triggered.
Complications were also stratified according to Clavien-Dindo classification.
Statistics
Statistical analysis was carried out using SPSS version 21 (IBM Corp, Armonk NY). Basic descriptive data were calculated as mean ± standard deviation (SD) or median and interquartile range (IQR). Tests for significance were chosen depending on data characteristics (Mann–Whitney U-test, t-test, Chi-square test, or Fisher's exact test); significance level was defined as p ≤ 0.05.
Results
Baseline characteristics of the cohorts
Preoperative data on the OAC/APD groups A, M, and P are compared with those of the control group-C in Table 1.
Preoperative Data
Shown parameters are median and interquartile range (IQR).
Shown parameters are percentage and affected patients/total number of patients.
Bold p-values mean significance.
BMI = body mass index; TRUS = transrectal ultrasound.
Median age of the A and M groups was significantly higher (pA = 0.002, pM<0.001) and the IPSS of the M group significantly lower (p = 0.036) than those of the controls. All three groups resemble the control group regarding BMI, IPSL, bladder capacity, length of the prostatic urethra, and prostate volume.
As expected, the preoperative blood results at the day before surgery showed a therapeutic Quick value in the M group. The other blood results, as well as the rate of preoperative catheter dependency, type of obstruction, and type of preoperative drug therapy, were equally distributed among the different groups.
Perioperative complications
Peri- and postoperative data are shown in Table 2. The median operation time ranged from 68 to 72 minutes, with a median resected prostate tissue mass of 21 g to 23 g with no significant differences between the four groups. An incidental prostate cancer was found in 15% (42/276) of the patients.
Peri- and Postoperative Data
Shown parameters are median and interquartile range (IQR).
Shown parameters are affected patients/total number of patients and percentage.
PVR = postvoid residual volume.
Bold p-values mean significance.
The transurethral bladder catheter was left in place significantly longer in the M group (median 42 hours vs 24 hours, p = 0.031); duration of the continuous irrigation was longest in the P group (median 24 hours vs 22 hours, p = 0.006) without producing a higher volume of irrigation fluid. The M group also showed a trend toward a longer irrigation time (median 24 hours vs 22 hours, p = 0.055) with a similar volume of irrigation fluid.
The main focus of this study was bleeding complications and bleeding parameters. The three OAC/APD groups had the following bleeding complications: 19 patients (9.4%) had clot retention, 9 patients (4.4%) needed a blood transfusion, 10 patients (4.9%) were readmitted due to bleeding, and 6 patients (3%) underwent a reoperation due to bleeding (Table 3). The three groups did not differ significantly with regard to loss of hemoglobin measured 6 hours postoperatively and at discharge. There were no thromboembolic complications within 3 months postoperatively.
Bleeding Parameters
Shown parameters are median and interquartile range (IQR).
Shown parameters are affected patients/total number of patients and percentage.
Bold p-values mean significance.
The clot retention rate was more than two times higher in the M and P groups compared with the C group. The Quick value of patients in the M group presenting with a worse bleeding complication was as expected in the therapeutic range (median 22%; range 15% −26%).
The rate of transfusion in the P group (19%) was significant (p = 0.01) and in the M group (5%) slightly (p = 0.08) higher than in the C group (1%). The rates of hospital readmission and reoperation due to bleeding were not significantly higher in the M group than in the C group (9% vs 3% and 5% vs 0%), whereas in the P group they were significantly (19% vs 3%; p = 0.04) and not significantly (6% vs 0%) higher than in the C group.
Urinary retention after postoperative catheter removal occurred in 26 patients, with a higher rate in the M group than in the C group (18% vs 6%, p = 0.044); 4 patients had an elevated PVR ≥100 ml. These 30 patients received either a transurethral bladder catheter (n = 26) or kept the existing suprapubic bladder catheter (n = 4). In 11 patients the catheter was effectively removed during hospital stay, 16 patients were discharged, and the removal of the catheter was effective in 16 patients after a median 7 days (2–17 days). Two patients kept their suprapubic bladder catheter due to hypo-contractility of the detrusor muscle and symptomatic elevated PVR.
Functional outcome and follow-up
Pre- and postoperative functional results such as IPSS/IPSL, Qmax, and PVR are shown in Figure 1. All groups showed a significant amelioration of the different parameters from pre- to postoperatively. The 12-month postoperative IPSS of the A group (5 vs 2, p = 0.009) and the 3-month postoperative PVR of the M group (20 mL vs 10 mL, p = 0.04) were higher than those of the C group.
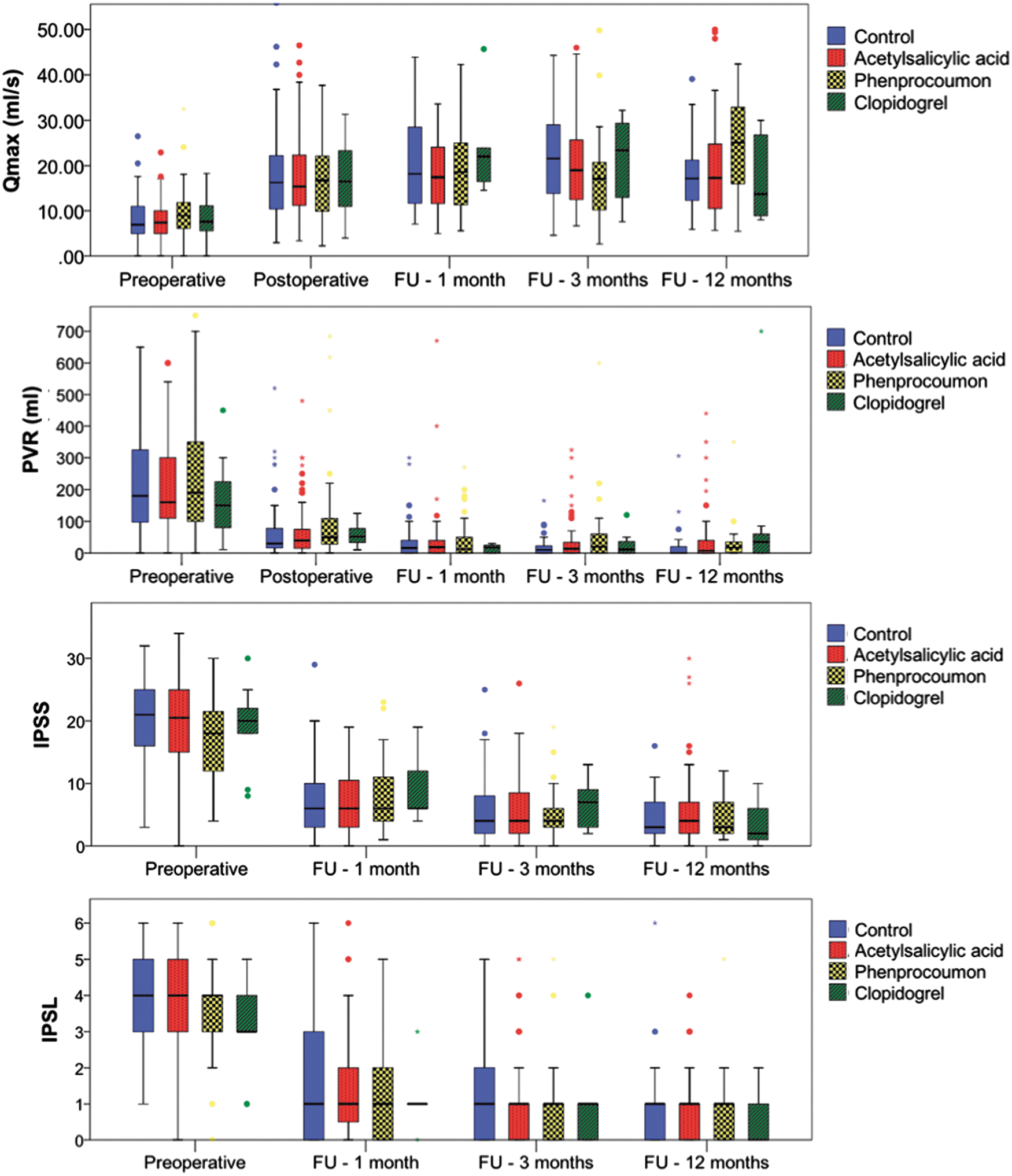
Functional results: Boxplots indicating the functional results of the analyzed parameters between the four groups.
Late complications are shown in Table 4. No differences were found regarding frequency of BNC and RA. US was more common in the P group than in the C group (20% vs 0%, p = 0.022), and the M group showed a trend toward a higher US rate (7% vs 0%, p = 0.077).
Late Complications (> 3 Months Postoperatively)
Shown parameters are affected patients/total number of patients and percentage.
Bold p-values mean significance.
The late reoperation rate, that is, operations not due to bleeding complications, was elevated in the P group (25% vs 8%, p = 0.027). Two patients had BNC, and one patient each was reoperated due to RA or US.
The complication rates were also stratified according to Clavien-Dindo and are shown in Table 5. Regarding the different grades of complications (maximal Clavien-Dindo III), we found comparable rates throughout all groups and all grades, but the overall complication rates were significantly higher in the M group with 43 complications in 63% of the patients (36 patients) vs 49 complications in 44% of the patients (32 patients) of the C group, p = 0.034.
Complications According to Clavien-Dindo
Bold p-values mean significance.
BNC = bladder neck contracture; RA = residual adenoma; US = urethral stricture.
Discussion
To our knowledge, we present the largest consecutive series of TURP patients from a single institution receiving ongoing OAC/APD. The OAC/APD was not paused or bridged during surgery. Their data were compared with data of TURP patients without OAC/APD.
Bleeding complications in the OAC/APD groups were clot retention in 9.4%, blood transfusions in 4.4%, rehospitalization in 4.9%, and reoperation due to bleeding in 3%.
Comparing our study with other studies is difficult because their data are usually heterogeneous or they performed surgery during paused or bridged OAC/APD, or used a different resection technique, or did not consistently operate during ongoing OAC/APD.
Descazeau and colleagues 7 published a series of 206 TURP patients with similarly distributed OAC/APD therapies as ours, but in whom the OAC patients and those under clopidogrel were bridged with LMWH during TURP and compared their results with those of 406 TURP patients not under OAC/APD. They found clot retention rates of 13% vs 4.7%, transfusion rates of 1.9% vs 1.0%, late hematuria in 15.0% vs 8.4%, longer hospitalization stays of 6.4 vs 4.7 days, and thromboembolic events in 2.4% vs 0.7% of patients. Like our series, their OAC/APD patients had about a threefold higher clot retention rate than controls, a twofold higher transfusion rate (our series fourfold higher), and a twofold higher late hematuria rate.
Ong and colleagues 8 retrospectively analyzed 107/293 patients under OAC/APD and found the highest bleeding complication rates in patients whose OAC was bridged with LMWH (44%), followed by patients under ongoing APD (17%), not receiving OAC/APD (8%), with paused APD (4%), and with paused OAC (0%).
In a retrospective analysis, Taylor and colleagues 9 found a ninefold higher bleeding complication rate in the first 28 days postoperative in TURP patients receiving OAC/APD vs patients without OAC/APD.
However, the aforementioned studies are not really comparable to ours because of their heterogeneous data and their use of bridging/pausing strategies for OAC/APD.
Our A group did not differ significantly in TURP outcomes from our C group; we conclude therefore that TURP can be performed safely under ongoing acetylsalicylic acid. Our data contrast with those of Wenders and colleagues, 10 which showed slightly longer hospitalization and catheter times and a threefold higher reoperation rate under acetylsalicylic acid than without APD.
Compared to the control group, our M group had a twofold higher catheter time, a threefold higher urinary retention rate after catheter removal, and slightly longer hospital stays, but did not differ significantly in hemoglobin decrease. The blood transfusion (9% vs 1%, p = 0.086) and reoperation (5% vs 0%, p = 0.082) rates were in trend slightly higher.
Almost three decades ago, Parr and colleagues 11 published a small study with 13 patients (12 TURP, 1 TUR of the bladder) under ongoing warfarin therapy. Of their patients, 31% (4/13) needed blood transfusions and 8% (1/13) recatheterization due to clot retention.
Chakravarti and MacDermott 12 reported results on 12 TURP patients whose warfarin therapy was bridged with intravenous heparin. Compared to our M group, they had a similar transfusion rate (8% vs our 9%), but a higher rehospitalization rate due to bleeding (25% vs our 9%) and a longer hospitalization time (median 6.7 days vs our 4 days).
Is bridging OAC with LMWH during TURP really safer than operating under ongoing OAC? Dotan and associates 13 compared 20 OAC TURP patients whose OAC was bridged with LMWH vs 20 TURP patients without OAC and found a twofold higher transfusion rate (20% vs 10% n.s.) and longer catheter (3.2 days vs 2.1 days, p < 0.01) and hospitalization times (4.2 days vs 2.1 days, p < 0.001) in the bridged group. Comparing these data to our M group we find a lower transfusion rate (9% vs 20%), shorter catheterization time (1.74 days vs 3.2 days), and similar hospital stay (4 days vs 4.2 days).
Taking the described literature, as well as other similar TURP outcomes from studies in the urologic literature, 7,8,12 –14 into consideration the results of TURP under bridged OAC therapy compared to ongoing OAC therapy suggest similar results. Of course this needs to be confirmed by a prospective randomized trial.
Our data showing acceptable bleeding complications justify performing TURP under ongoing OAC therapy, thus avoiding the risks and expenditure of bridging procedures (fluctuation in coagulation and costs of additional doctor visits).
Regarding bleeding complications in our P group compared to controls, we found slightly longer irrigation times, comparable catheter times, a significantly higher rate of blood transfusions (19% vs 1%, p = 0.017), and a higher readmission rate (19% vs 3%, p = 0.039). This blood transfusion rate appears to be rather high. Regarding the patient in need of a blood transfusion, we found that two were under dual APD therapy (acetylsalicylic acid/clopidogrel) and one under clopidogrel alone. Patients under dual APD are usually being treated for severe heart disease with, for example, a newly implanted coronary stent requiring dual APD for 12 months. Such high-risk patients with different comorbidities usually receive blood transfusions earlier than other patients.
Since our P group is relatively small and received both single and dual APD with clopidogrel and acetylsalicylic acid, definitive conclusions are not possible. Provided our P group is considered to be representative, TURP under ongoing clopidogrel entails an increased rate of blood transfusion. This consequence needs to be balanced against an increased risk of stent occlusion with potentially lethal complications in these high-risk cardiac patients. 15 These considerations need to be discussed with the patient.
Pure data on TURP patients under ongoing clopidogrel therapy are scarce in the literature. In an analysis of patients under either acetylsalicylic acid or clopidogrel, pausing the clopidogrel perioperatively was associated with a clot retention rate of 13% and a transfusion rate of 1.4%. 7
Another question is whether laser techniques such as photoselective vaporization of the prostate (PVP) or prostate enucleation (holmium laser enucleation of the prostate, HoLEP, or thulium laser enucleation of the prostate, ThuLEP) can lower the bleeding risk in OAC/APD patients. As in TURP studies, the data are heterogeneous and assessed under different OAC/APD management regimens.
Chung and coworkers 16 report that use of the PVP technique in 151 patients under similar OAC/APD regimens as ours with paused warfarin but ongoing acetylsalicylic acid and clopidogrel was associated with a 3% rate of delayed bleeding complications within 30 days after discharge and a 2% rate of transfusions. For patients under acetylsalicylic acid, clopidogrel, and paused warfarin, the rates of bleeding complications and transfusions were 2% and 0%, 6% and 6%, and 5% and 0%, respectively.
Elzayat and colleagues 14 report that use of the HoLEP technique in a heterogeneous cohort of 81 patients (14 ongoing OAC, 33 OAC bridged with LMWH, and 34 paused OAC) resulted in an overall transfusion rate of 10%, a rate under ongoing OAC of 14%, under bridged OAC of 15%, and with paused OAC of 3%. Tyson 17 published 37 patients treated by HoLEP with excellent results and no transfusions.
Ruszat 18 reported excellent results in 71 patients receiving PVP under ongoing acetylsalicylic acid, 36 under ongoing phenprocoumon, and 9 under ongoing clopidogrel therapy with no blood transfusions or clot retention. However with only 61% patients having an international normalized ratio (INR) >2.0 ( = Quick <37%) at the time of surgery, it is questionable whether or not the OAC therapy was executed properly.
Spernat 19 reported no transfusions in 18 patients treated by PVP under ongoing clopidogrel therapy.
Regarding functional TURP results under ongoing OAC/APD as assessed by pre- and postoperative IPSS/IPSL, urinary flow, and PVR, all groups showed significant improvement (Fig. 1). Small differences between the OAC/APD groups compared to controls (IPSS of the M group and A group, IPSL of the A group at 12 months) do not appear to be of clinical significance. Therefore, we conclude that the functional outcome 12 months after TURP is not affected by presence or absence of perioperative APD/OAC.
Comparing our long-term results (Table 4) to those in the literature, our reoperation rate of 11.2% for all OAC/APD groups at 8 years (1.4% per year) postoperative is comparable to the 2.6% rate in the review of Madersbacher and Marberger. 20
We conclude that bipolar TURP can be performed safely in patients under ongoing APD with acetylsalicylic acid without risking increased bleeding complications. Patients under OAC with phenprocoumon or under APD with clopidogrel can also be operated on safely without stopping OAC/APD, while clopidogrel may increase bleeding complications and blood transfusions. These risks need to be discussed with the patient because they may be far outweighed by the risk of potentially lethal thromboembolic events entailed by stopped or paused OAC/APD.
Footnotes
Authors' Contributions
L.M., P.S., A.M., and H.D. designed the study. A.R., J.B., and H.D. drafted the article. Statistical analysis was carried out by A.R. and F.O. All authors have read and approved the final article.
Transparency Declaration
The lead authors (A.R. and J.B.) affirm that this article is an honest, accurate, and transparent account of the study being reported and that no important aspects of the study have been omitted.
Author Disclosure Statement
No competing financial interests exist.