
Abstract
Introduction:
Routine preoperative electrocardiogram (ECG) before shockwave lithotripsy (SWL) is frequently performed despite recommendations against its use in asymptomatic patients undergoing low-risk surgical procedures. This study assesses whether routine preoperative ECG before SWL is useful in patients at low risk for cardiac complications.
Materials and Methods:
A retrospective study of SWL at our center (2003–2013) reviewed all cardiac-related preoperative cancellations, intraoperative complications, postoperative admissions, and emergency department presentations in patients at low risk for cardiac complications. Patients received SWL with sedation and continuous five-lead ECG monitoring.
Results:
Of 30,892 referrals, preoperative ECG triggered 13 (0.04%) cancelations in low-risk patients (1 with new atrial fibrillation and 12 with ischemia/previous infarction). Of these patients, 1 had a subsequent abnormal cardiac work-up and 11 underwent uncomplicated SWL without cardiac intervention (2 had unknown history). Of 27,722 treatments, 5 (0.02%) were stopped prematurely in low-risk patients because of arrhythmia (3 had normal preoperative ECG, 1 had abnormal ECG, and 1 did not complete ECG). Three patients developed an arrhythmia with sedation and 2 patients were admitted postoperatively because of cardiac complications (1 for atrial fibrillation and 1 for hypertension), of whom all had normal preoperative ECG. No patients presented to our emergency department with cardiac complications after SWL.
Conclusions:
In patients at low risk for cardiac complications, preoperative ECG triggered very few cancellations and did not predict early termination of treatment or cardiac complications after SWL. These findings suggest that in low-risk patients, routine preoperative ECG has little effect on treatment or complication rate and should be omitted.
Introduction
Shockwave lithotripsy (SWL), although noninvasive, is associated with perioperative cardiovascular complications, of which transient cardiac arrhythmias are the most common. 1,2 Rare cases of persistent cardiac arrhythmia, myocardial infarction, malignant hypertension, aortic aneurysm rupture, vein thrombosis, and cardiovascular collapse causing death have been reported. 1,2 For this reason, and to monitor patients for other possible complications while under intravenous sedation and analgesia, patients undergo continuous cardiac monitoring during SWL.
The American College of Cardiology has concluded that a preoperative electrocardiogram (ECG) for asymptomatic patients undergoing low-risk surgical procedures, classified as having a risk of major cardiac event or death of <1%, has no benefit and has recommended against it.
3
The Choosing Wisely
The benefit of ECG before SWL in low-risk patients has not been studied. As such, preoperative testing before SWL is not standardized and practice varies widely. A survey from our institution found that 48.7% of urologists practicing in the United States and 63% in Canada perform baseline ECG before SWL based on an age cutoff in low-risk patients. 6 At our center, at the request of our anesthesia colleagues, all patients more than the age of 40 years have an ECG before SWL. This study aims to determine whether a routine preoperative ECG before SWL in patients at low risk for cardiac complications is useful in predicting occult cardiac disease, which would have otherwise been missed, or predicting cardiovascular complications.
Materials and Methods
A retrospective study of patients referred for SWL for urolithiasis at our center for a 10-year period from January 2003 to December 2013 was performed. The hospital ethics review board approved the study protocol. Patients received SWL treatment on a fixed lithotripter with the Philips Lithotron Ultra from 2003 to 2010 (17,228 treatments) and with the Storz Modulith SLX-F2 from 2010 to 2013 (10,494 treatments) under intravenous sedation with continuous five-lead ECG monitoring under the care of an anesthesiologist. We reviewed the prospectively collected database of preoperative cancellations and intraoperative complications. All admissions to hospital and visits to our emergency department within 48 hours were also evaluated. Charts were reviewed for clinical data, cardiac risk classification, and to identify cardiovascular complications, including new persistent arrhythmia, malignant hypertension, myocardial infarction, aneurysm rupture, major vessel thrombosis, and sudden death. Bleeding was not included as a cardiovascular complication. ECGs were considered abnormal if they had atrial fibrillation, bundle branch block, left ventricular hypertrophy, premature ventricular complexes, pacemaker rhythm, Q-wave changes, or ST-segment changes. 7
Only patients who were classified as low risk for cardiac complications were included in the analysis. Low-risk status was defined based on a modified Revised Cardiac Risk Index (RCRI) that predicts a <1% risk of major cardiac event. 8 Low-risk criteria included no history of arrhythmia, ischemic heart disease, congestive heart failure, cerebrovascular disease, insulin use for diabetes, and serum creatinine >2.0 mg/dL (>177 μmol/L) (Table 1). Patients were excluded from the study if clinical history could not be obtained to classify the nature of the event or risk classification.
Cardiac Risk Classification
An additional sample of patients was analyzed to estimate the demographics and risk characteristics of the entire population of patients referred for SWL. Every 100th patient referred for SWL treatment from 2007 to 2013 was included in this sample for a total of 161 patients. Furthermore, as a quality control measure, we reviewed all troponin laboratory tests ordered at our hospital within 30 days of SWL treatment from January 2008 to December 2013 to determine whether any cardiac events during that time period were missed in our initial review.
Results
There were 30,892 referrals for SWL during the study period. A random sample of 161 patients who were referred for SWL treatment demonstrates that 84% of patients were low risk. Of the low-risk patients, 85% completed a preoperative ECG and 20% of these ECGs were abnormal. Patients were American Society of Anesthesiologists (ASA) class 1 (30%), 2 (43%), 3 (20%), and 4 (3%) with 7 (4%) patients' ASA class not recorded by the treating anesthesiologist.
Of 67 preoperative cancellations for cardiovascular reasons, 22 (32%) patients were low risk. Of these 22 low-risk cancellations, 9 were caused by hypertension and 13 were because of concerns raised by an abnormal ECG, including previously undiagnosed atrial fibrillation in 1 patient and an ECG suggesting ischemia or previous infarction in 12 patients. Of the 13 patients with an abnormal ECG, 10 had a normal subsequent cardiac work-up and 1 patient was discovered to have abnormal ejection fraction (Fig. 1). Eleven patients underwent uncomplicated SWL without cardiac intervention with two patients lost to follow-up.
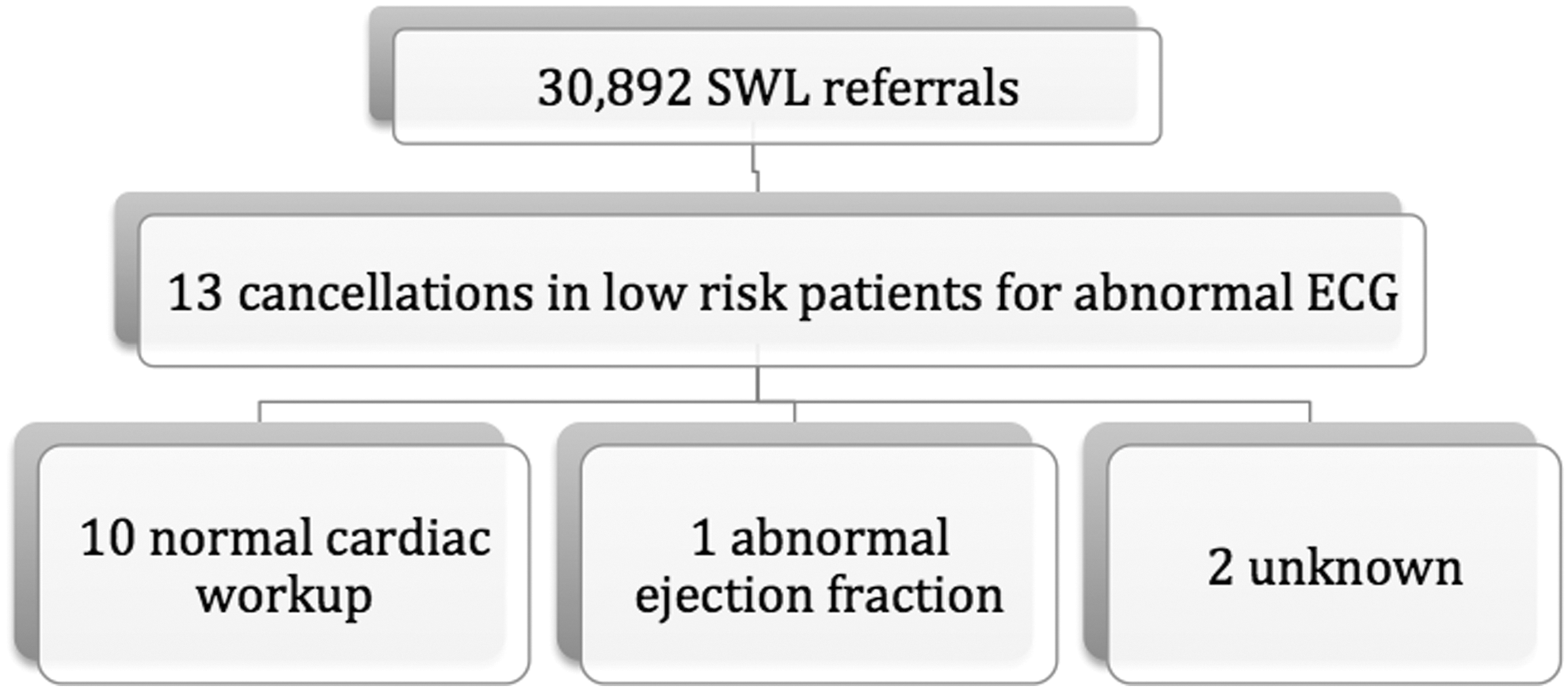
SWL cancellations for an abnormal ECG in low-risk patients. ECG = electrocardiogram; SWL = shockwave lithotripsy.
In one low-risk patient, a preoperative ECG showed occasional premature ventricular contractions and bigeminy and the patient then underwent SWL simulation without sedation. The treatment was cancelled and the patient was referred to an outpatient cardiologist because the five-lead ECG tracing during simulation showed similar changes (Fig. 2). The patient was started on a beta-blocker and an angiotensin-receptor blocker and subsequently underwent SWL with noted bigeminy during the procedure. Three low-risk patients developed arrhythmia after administration of sedation and SWL was not initiated, of whom all had a normal preoperative ECG.
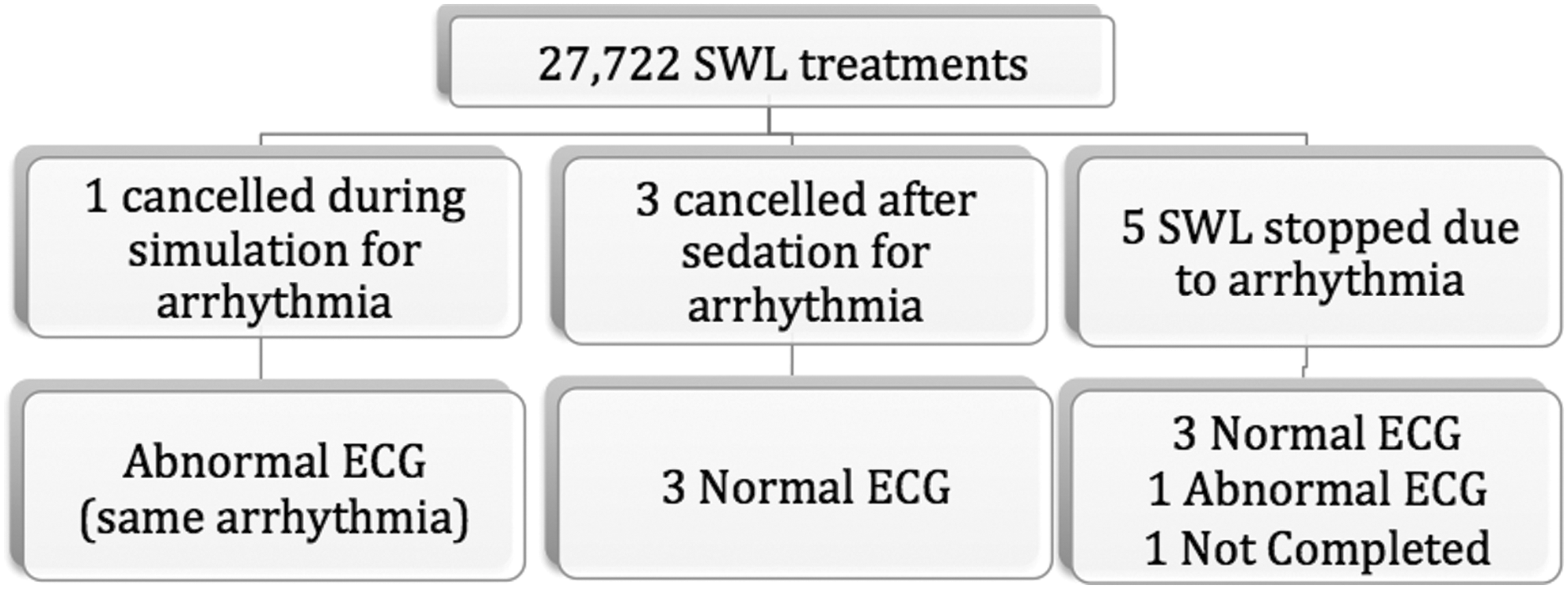
Intraoperative cardiovascular complications and corresponding preoperative ECG in low-risk patients undergoing SWL.
During 562 (2%) of the 27,722 SWL treatments, patients developed an arrhythmia that required continuation of treatment with cardiac gating. Despite this gating, five (0.02%) low-risk patients developed arrhythmia intraoperatively, resulting in the treatment being stopped prematurely (Fig. 2). These arrhythmias included sustained supraventricular tachycardia in four patients and complete heart block in one patient. In these five patients, preoperative ECG was normal in three, abnormal in one, and not completed in one patient.
Three low-risk patients were admitted postoperatively because of cardiovascular complications (Fig. 3). One patient had persistent atrial fibrillation and a normal preoperative ECG. Two patients were admitted with hypertension, one had a normal preoperative ECG, and the second had an abnormal ECG with Q-waves in lead II; however, SWL was initiated without further testing. No patients presented to our emergency department with cardiovascular complications within 2 days after SWL. There were no episodes of myocardial infarction or sudden death during the study period.
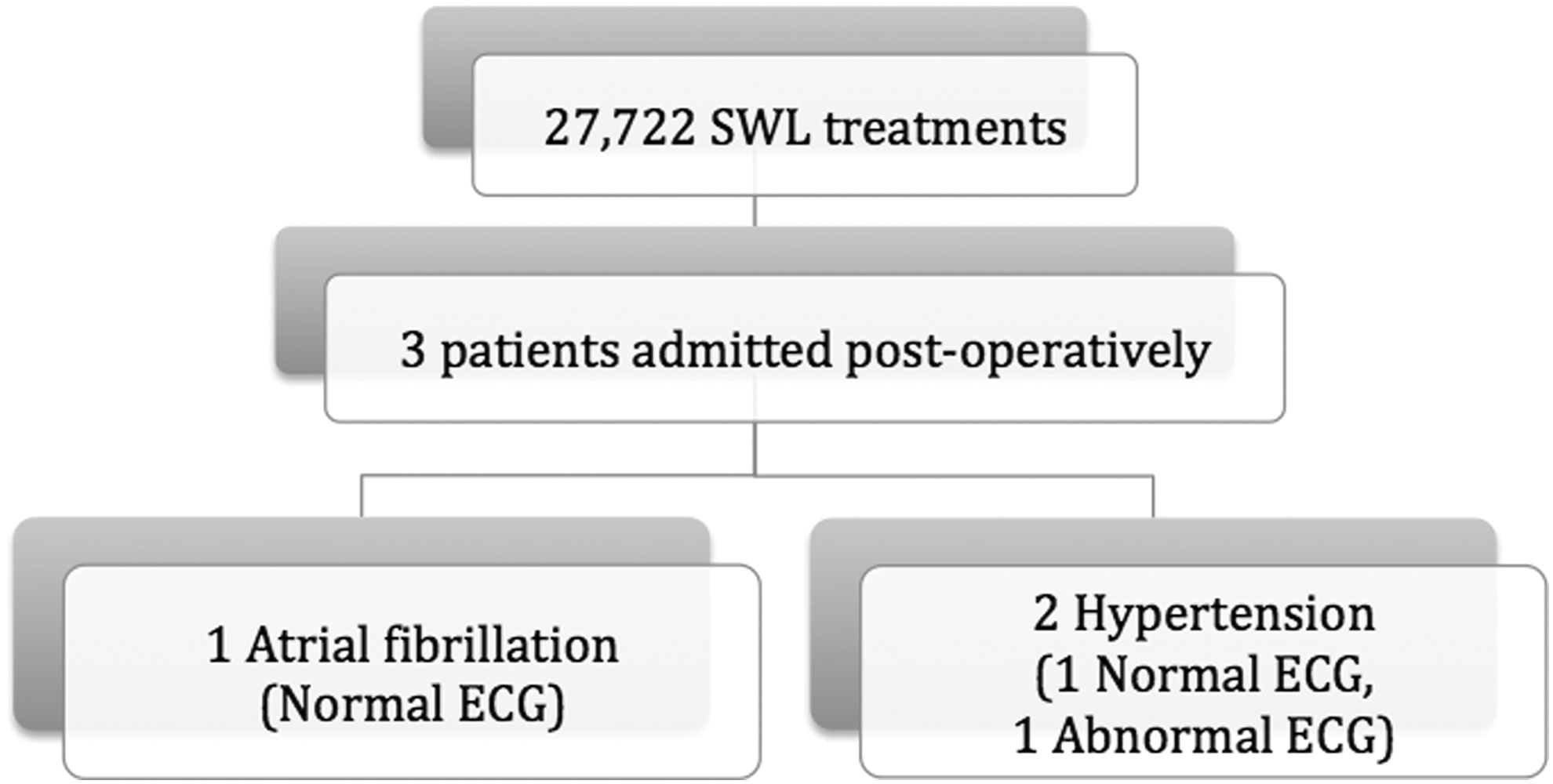
Postoperative cardiovascular complications and corresponding preoperative ECG in low-risk patients undergoing SWL.
Review of all troponin laboratory tests performed at our hospital within 30 days of SWL treatment for a 5-year period (2008–2013) revealed 11 tests were performed. Three troponin tests were within 24 hours of treatment, three were within 24 to 48 hours of treatment, and five were within 48 hours to 30 days of treatment. All troponin levels were within the normal range.
Discussion
With the first-generation lithotripters, SWL was performed by synchronizing shockwaves with the refractory stage of the cardiac cycle, called gating. 1 Without gating, arrhythmia occurred in up to 80% of cases. 1 In the newer generation lithotripters, arrhythmia is reduced but still occurs in up to 30% of cases and has been recorded with all types of lithotriptors: electrohydraulic, electromagnetic, and piezoelectric. 9 Common arrhythmias include ventricular and atrial extrasystoles and less frequent arrhythmias include sinus bradycardia and asystole hypotension. 9 –12 Cardiac arrhythmias typically resolve with brief interruption (2–5 minute) of the procedure, 11 change of position, 13 after switching to an ECG-gated delivery, 1 and have been reported to resolve in some cases with intravenous atropine or lidocaine. 11,14 As most arrhythmias arising during treatment are benign and self-resolving, we only recorded cases that resulted in gating or termination of treatment.
Anesthesiologists at our center request a preoperative ECG on all patients more than the age of 40 before SWL because of the potential arrhythmias that may occur during treatment. Preoperative ECG testing in low-risk surgery may not predict occult cardiac disease and does not prevent perioperative morbidity in the vast majority of patients. For cataract surgery, Schein et al. estimated that routine preoperative medical testing costs $150 million annually in the United States, and showed that routine testing including ECG did not increase surgical safety. 15,16 Starting in 2007, and reconfirmed in 2014, the American College of Cardiology/American Heart Association has recommended that routine ECG not be performed for asymptomatic patients undergoing low-risk surgery (Level of Evidence: B). 3,17 We performed a survey of urologists in the United States and Canada and determined that almost 50% of respondents routinely perform ECGs in low-risk patients before SWL. 6
A low-risk procedure is defined as having a risk of a major adverse cardiac event (MACE), including death and myocardial infarction of <1%, where this risk is calculated based on the risk of surgery and patient comorbidity. 3 For noncardiac surgery, the perioperative MACE can be estimated using validated risk-prediction tools such as the RCRI. 3,8 With an RCRI score of 0, patients have an MACE risk of 0.5%. 8 We classified patients as low risk by using the RCRI criterion, which predicts a <1% risk of major cardiac event. We further modified the RCRI and decreased the risk further by excluding patients if they had a history of arrhythmia. Arrhythmia history would increase the need for gating and treatment time and, therefore, preoperative ECG in this group is useful for treatment planning and patient scheduling. In addition, patients with a history of cardiac revascularization with percutaneous coronary intervention or coronary artery bypass grafting were not considered low risk, regardless of timing and lack of symptoms, as at least one study has shown that a history of ischemic heart disease is correlated with postoperative myocardial infarction, regardless of revascularization. 18 This modified criterion is stricter than the RCRI and, therefore, decreases the risk in the low-risk group. 8
Furthermore, although patients with routine preoperative ECG showing Q-waves are high risk under the RCRI criterion, for this study our modified criterion considered patients with preoperative Q-waves to be low risk to simulate the risk stratification of patients if routine preoperative ECG was not completed. The procedural risk scoring was considered to be low given that SWL is not intraperitoneal, intrathoracic, or suprainguinal vascular surgery. 8 SWL is further justified as being low risk given the low rate of cardiac complications.
Despite 20% of preoperative ECGs in low-risk patients being abnormal, only 13 low-risk patients had SWL cancelled because of abnormal ECG, suggesting that the preoperative ECGs seldom prompted further action by the anesthesiologist. Of these 13 patients, only one had a subsequent abnormal cardiac work-up, and all patients with follow-up underwent uncomplicated SWL without cardiac intervention, indicating that the ECG did not detect clinically significant occult cardiac disease.
The value of preoperative ECG has also been questioned for intermediate or high-risk patients with known coronary artery disease. 17 Furthermore, revascularization surgery is not always indicated before surgery in high-risk patients if the patient is asymptomatic, 17 and a randomized trial has shown no long-term benefit to revascularization in patients before vascular surgery. 19,20 The added benefit of preoperative ECG in low-risk patients undergoing SWL is, therefore, easily questioned.
In the 10-year experience at our center only one low-risk patient, showed possible benefit from preoperative ECG. This patient underwent cardiac intervention with medications before treatment, which may have decreased the perioperative cardiac risk.
Arrhythmias can result in early termination of treatment and, in rare circumstances, cause cardiac complications requiring further intervention. 21 In one of the largest series reporting side effects of gated SWL that included 600 patients, only five episodes of arrhythmia were identified, resulting in the termination of one treatment. 14 Of these five patients, four had a normal ECG, and one had changes suggestive of mild ischemia. 14
Although the etiology of arrhythmia during SWL is unclear, it is likely caused by interference with myocardial conductivity. 11 There may be a relationship with medication, but the majority occur naturally without underlying cardiac disease. 9 A study from our center demonstrates that positional changes reduce recurrence, which likely points toward shockwaves having a direct or indirect interference on cardiac conductivity. 13 In a retrospective cohort study by Skinner and Norman, there was no correlation with cardiac risk or medical comorbidity, and arrhythmias were more likely to occur in younger patients with right-sided treatment. 22 However, given the low rate of cancellation or complication caused by treatment-induced arrhythmia in low-risk patients, in addition to constant ECG monitoring during the case, this study suggests that obtaining a preoperative ECG would change management in very few patients and should not be routinely performed.
Not performing preoperative ECG in low-risk patients would be cost saving. From 2014 to 2015, 2738 SWL procedures were performed at our center, and reducing preoperative ECG in low-risk patients from the current rate of 85% to 0% would save 2327 ECGs per year with a cost savings of $49,804, assuming an estimated overall cost of $21.40 per ECG. This does not include the cost savings associated with additional tests and unnecessarily cancelled SWL treatments.
This study has limitations including its retrospective design that may result in bias in data collection and missed events. Only patients wherein clinical history could be obtained to classify the nature of events and risk classification were included in the study. The review of troponin results demonstrated that no in-hospital cardiac events were missed in our review for the past 5 years. However, patients with postoperative cardiovascular events who presented elsewhere after discharge would have been missed. This would include patients who had a late postoperative complication. This study does not include patients who had an ECG work-up before SWL and were subsequently not referred for treatment because of an abnormal ECG.
Conclusions
Considering patients at low risk for cardiac complications, an ECG before SWL triggered few cancellations and did not predict arrhythmia during sedation, early termination of treatment, or postoperative cardiac complications. These findings suggest that in low-risk patients, a routine preoperative ECG has little effect on treatment course or complication rate and should be omitted. As a result of this study, these changes have made our center more efficient and represent substantial cost savings.
Footnotes
Author Disclosure Statement
No competing financial interests exist.