
Abstract
Introduction:
The widespread use of diagnostic and therapeutic ionizing radiation raises concerns regarding excessive occupational and patient exposure. In this study, we test a novel fluoroscopic technique that has the potential to minimize radiation dose during urologic procedures.
Materials and Methods:
A prospective evaluation of all patients undergoing endoscopic urologic procedures in our institution was conducted. A “two-point technique (TPT)” is described in which the fluoroscope image intensifier (c-arm) is shifted between caudal and cephalad set points of the operative field. We wished to determine whether patient radiation exposure was lower with TPT than with a non-structured conventional technique, referred to as the cognitive fluoroscopic technique (CFT), in which the manipulation of the c-arm was at the discretion of the user. We obtained all clinical, radiographic, and fluoroscopic data of patients in the study period and used unpaired nonparametric statistical analysis of univariates entered stepwise into a logistic regression model.
Results:
A total of 106 endoscopic urologic procedures from January 2016 to November 2018 were reviewed. Forty-four (41.5%) cases were performed using TPT and 62 (58.5%) using CFT. The mean fluoroscopy time of TPT vs CFT was 71.1 (±60.8) seconds vs 104.5 (±91.6) seconds, respectively (p = 0.04), and the mean radiation dose on TPT vs CFT was 11.6 (±10.6) mGy vs 20.3 (±24.3) mGy, respectively (p = 0.03). TPT was an independent predictor of reduced operative room (OR) time and fluoro time (p < 0.05), while body mass index, age, and operator were not.
Conclusion:
The “TPT” helps reducing radiation dose and fluoroscopic time during endoscopic urologic procedures. The TPT is useful to lower radiation exposure to patients and OR staff.
Introduction
With the advances in percutaneous and endoscopic surgery, the implementation of continuous fluoroscopy for guidance during these procedures has increased the utilization of ionizing radiation today. This is of significant concern due to potential long-term exposure of patients and staff alike. In urology, the mean fluoroscopy time during ureteroscopy has been reported as high as 144 seconds per case with multiple efforts directed to limit radiation exposure. 1 Still, patient radiation dose exposure during these procedures lies between 2.5 and 100 mGy. 2
According to the Occupational Safety and Health Administration (OSHA), the retrospective annual whole-body ionizing radiation exposure should not exceed 10 to 15 rem/year (100–150 mGy/year), while prospectively, this limit was set to 5 rem (50 mGy) in any 1 year and to 3 rem during any calendar quarter. 3 The outcomes of consistently crossing this limit by health care providers and patients requiring multiple and/or recurrent diagnostic and therapeutic procedures are unknown below a limit of 100 mSv (10 rem) and not proven to be associated with a higher cancer risk 4 ; however, this could be underestimated, as reflected by the report of Berrington de González, et al. 5 In their study, it was shown that in the United Kingdom, about 0.6% of the cumulative risk of cancer to age 75 years could be attributable to diagnostic X-rays. This is equivalent to about 700 cases of cancer per year. In 13 other developed countries, estimates of the attributable risk ranged from 0.6% to 1.8%, whereas in Japan it surpassed the 3%. Additional deleterious effects are today proven, such as the 40- to 100-fold higher rate of cataract formation and other ophthalmic pathology reported in health care workers who use C-arm fluoroscopy, compared with control populations. 6 –8
In an attempt to minimize unnecessary occupational radiation exposure, newly developed “low-dose–high-quality image” X-ray tubes have been developed as well as techniques to limit radiation utilization. Such maneuvers include lowering the frame rate, minimizing electronic magnification, collimation, image “hold” and “store,” increasing the distance from the beam, surgeon control of the C-arm, and providing real-time feedback on usage time. 1,9 –11 Pulsed fluoroscopy, for example, may reduce fluoroscopy time and radiation dose by 76% and 64%, respectively, compared with continuous fluoroscopy. 12 Other measures, such as the “freehand puncture technique” for percutaneous nephrolithotomy and “zero-dose fluoroscopy” for ureteroscopy, have been proposed as effective methods to reduce or eliminate X-ray delivery to patients and care providers and follow the well-known A.L.A.R.A. (as low as reasonably achievable) principle. 1,13,14
We here describe the novel “two-point technique” (TPT) for urologic endoscopic procedures, which may help limit the time of and exposure to ionizing radiation. We conducted a comparative evaluation of clinical outcomes in the endoscopic management of urinary calculi, upper urinary tract urothelial tumors, and ureteral strictures using the TPT vs the conventional, nonstructured, cognitive fluoroscopic technique (CFT).
Materials and Methods
After internal review board approval at the sponsoring institution, all the fluoroscopically guided endoscopic procedures in the department of urology from January 2016 to November 2018 were prospectively evaluated.
Inclusion criteria were adult (i.e., age >18) males and females requiring ureteroscopy or any fluoroscopy-guided endoscopic urologic procedure. Percutaneous renal procedures were not included in this study. The cohort was divided into two groups: TPT and CFT. Demographic and clinical data were collected. Mean fluoroscopy time and dose and, secondarily, mean operative room (OR) time were measured and documented. All the TPT-guided procedures were performed by a single surgeon (M.E.). In the CFT group, multiple surgeons, except M.E., participated, implementing any nonstructured fluoroscopic technique. In these cases, the C-arm was handled at the discretion of the surgeon and the X-ray technician. This study had no patient randomization. The X-ray technicians assisting in the procedures were randomly assigned by the X-Ray department, as routinely done in the OR.
Description of the TPT
In TPT, the practitioner assigns a fixed cephalocaudal axis over which the C-arm is positioned at the beginning of the procedure and then shifted between two predetermined landmarks, called “points” (Fig. 1). First, two scout fluoroscopic images are taken and the limits of the field (caudal and cephalad) are set. Then, two physical marks are made on the C-arm's collar at the degrees' ruler corresponding with each point. These points are called “point 1” or “caudal,” which covers from the symphysis pubis to the ipsilateral sacroiliac joint, and “point 2” or “cephalad,” which extends from the upper limit of point 1, with a slight overlap, to the upper border of the 10th rib. The distance between the two points typically corresponds to 10° in the collar's ruler. At this point, instead of manipulating the whole machine or utilizing multiple articulations to adjust the image to the anatomic zone of interest, only the collar or “neck” of the fluoroscope is utilized to rotate the C-arm in the cephalocaudal direction and vice versa. Having these two points set, the surgeon can efficiently indicate to the X-ray technician which point should be shown in each step, either point 1 or 2, and in this way, the technician receives clear instructions of when to switch between the two marks on the C-arm's collar, thus limiting the amount of radiation to the minimum required for the specific step and indication (Fig. 2).
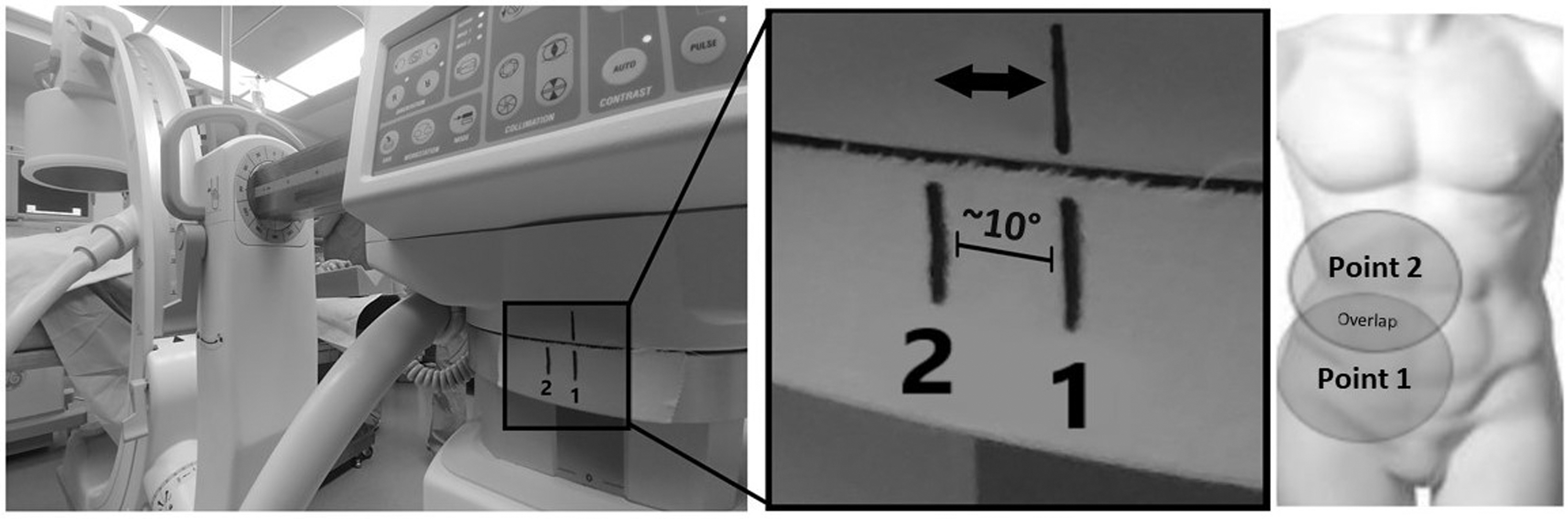
The TPT. Two scout images are obtained at the initiation of the procedure and fixed on the C-arm (center panel magnified), here labeled 1 for most caudal and 2 for most cephalad fixed points (right panel). The distance between point 1 and point 2 corresponds to ∼10° on the C-arm's collar. TPT = two-point technique.
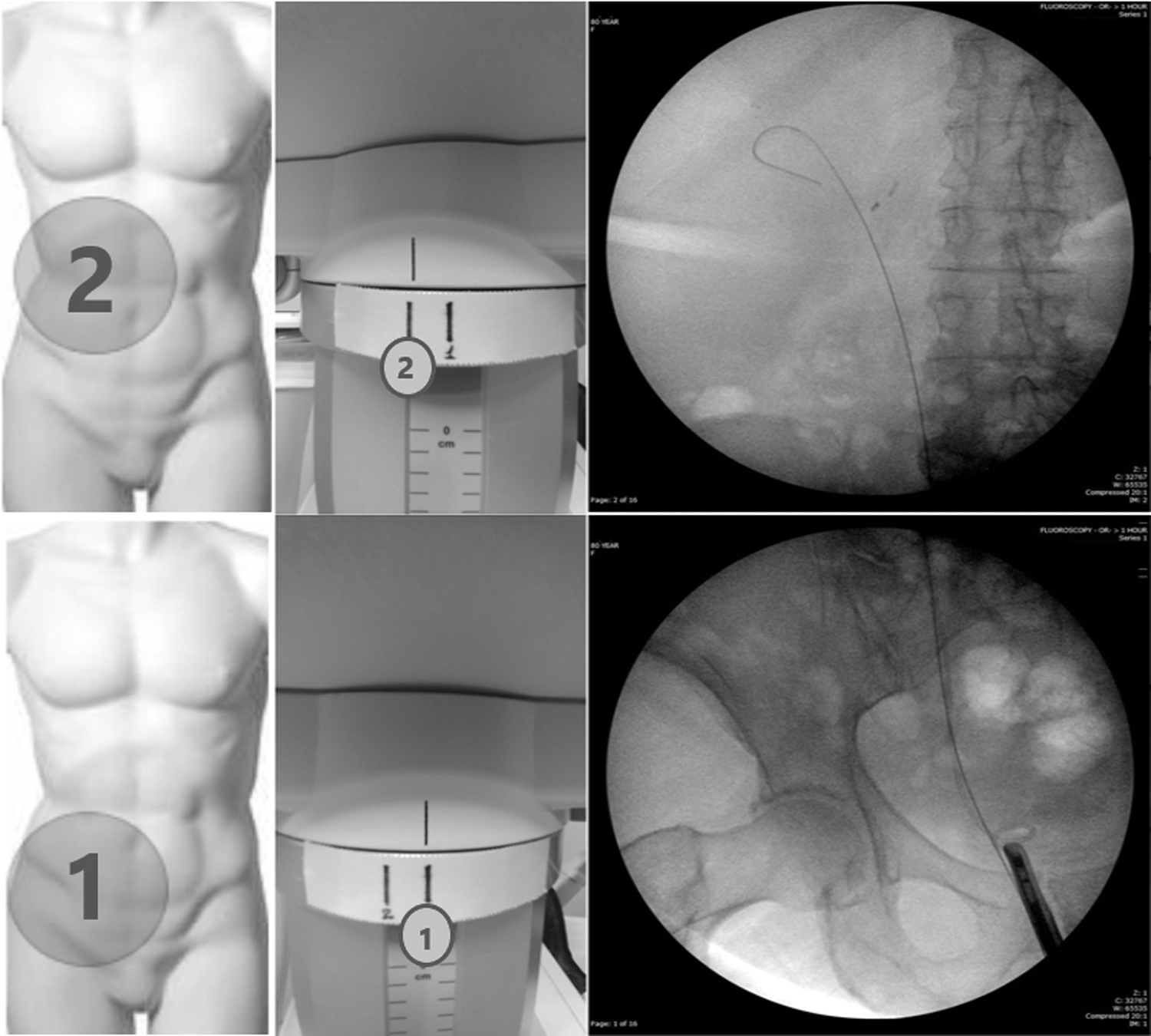
TPT—points of technique. The “point 1” or “caudal” (lower left panel) is set to extend from the symphysis pubis to the upper limit of the ipsilateral sacroiliac joint (lower right panel). The “point 2” or “cephalad” (upper images) correspondingly extends from the upper limit of “point 1” to the upper border of the ipsilateral 10th rib. The image intensifier is shifted between the points 1 and 2 by slightly rotating the C-arm at its collar (middle panels).
Statistical considerations
Statistical analysis of continuous variables was performed with Student's T-tests or, when nonparametric assumptions were made, Mann–Whitney U-tests (MedCalc software [Ostend, Belgium]). Significant univariates were entered into a linear regression model to determine predictors of radiation exposure.
Results
The original study population comprised 107 patients (undergoing 144 procedures), 96 of which had sufficient clinical and radiologic information for the analysis, resulting in a total of 106 studied procedures. These included ureteroscopic stone treatment (n = 49), ureteral or renal pelvis biopsy (n = 19), endoscopic upper urinary tract tumor resection/ablation (n = 14), diagnostic ureteroscopy (n = 10), Double-J stent exchange (n = 5), dilation of ureteral stricture (n = 7), and endopyelotomy (n = 2). Of the 106 procedures, 44 (41.5%) were performed under TPT and 62 (58.5%) using a CFT. The TPT and CFT groups were similar in age, height, weight, and body mass index (BMI) but not gender (Table 1). Patients undergoing TPT had more and larger stones, more proximal stones, and a higher rate of postoperative stent placement than the CFT group (Table 2).
Demographic Data
BMI = body mass index; CFT = cognitive fluoroscopic technique; TPT = two-point technique.
Preoperative Data
Stent exchange only with no additional procedures/manipulation.
Diagnostic ureteroscopy only with no additional procedures/manipulation.
Fluoroscopy time in TPT was lower than in CFT (71.1 ± 60.8 seconds vs 104.5 ± 91.6 seconds, respectively [p = 0.04]), and the mean radiation dose of TPT was less than that of CFT (11.6 ± 10.6 mGy vs 20.3 ± 24.3 mGy, respectively [p = 0.03]). The operative time was lower in the TPT group (46.6 minutes vs 65.8 minutes) (p < 0.05) as well (Table 3). On multiple linear regression analysis, TPT and ureteral dilation were independent predictors of fluoroscopy time and OR time (TPT, negative; and ureteral dilation, positive). In addition, TPT was an independent predictor of decreased OR time and fluoroscopy time (p < 0.05), while BMI, age, and operator were not.
Endpoints
Discussion
With the advent of new radiographic techniques, significant developments have been made in both diagnostic and therapeutic procedures. Along with the benefit of this technology, much understanding has occurred with respect to the consequences of radiation and secondary malignancies. 7 Urologists and their patients routinely encounter the risks of radiation as it is a frequently used and often necessary modality that helps provide care to patients. Limiting the side effects of radiation has led to development of the A.L.A.R.A. principle as well as various techniques in ureteroscopy to reduce radiation exposure. Our goal as clinicians should be to limit radiation use to only when necessary, delivering cost-effective treatment for our patients with the lowest risks and negative health consequences.
Interest in the use of a standardized technique to limit radiation in ureteral stent placement or exchange is apparent and has been recently proposed by Dellis et al. 15 In their protocol, they used fluoroscopy only to confirm wire placement and stent position. Additional fluoroscopy was not applied unless resistance was encountered. Over a 3-month period, a decrease was seen in fluoroscopy time (64 seconds vs 29 seconds, p < 0.001) and mean operative time (1068 seconds vs 690 seconds, p < 0.001); however, this limited utilization of fluoroscopy cannot be universally applied, especially in complex cases in which intermittent fluoroscopic monitoring is required. Other techniques such as reducing the frame rate, using pulsed fluoroscopy, optimizing collimation, and shielding with lead garments have already been proposed to reduce the radiation risks. 16
In our study, TPT decreased fluoroscopy time by 33% (71.1 seconds vs 104.5 seconds) and the mean radiation dose by almost half (11.6 mGy vs 20.3 mGy). In addition, our study demonstrates that such a standardized approach can probably shorten mean operative time.
Finally, we found that the concept TPT is well accepted by the X-ray technicians. They typically master the technique after two to three cases, becoming interactive with the OR team throughout the case and allowing for easier communication. Our technique automatically increases the awareness of the clinician to the fluoroscopy time and it is applicable wherever a fluoroscopic C-arm is available to oscillate between the two points, having no limitations with respect to height, BMI, or case complexity.
The TPT is a different approach dependent on the discretion of the user. Adoption of a two-point technique together with other radiation-sparing techniques can clearly have a synergistic benefit.
The limitations of our study include the relatively small sample size and clinical scenarios that may differ between surgeons who perform TPT and those who do not. Furthermore, the fact that all the TPT procedures were performed by an experienced endourologist may influence the radiation dose applied as well as the fluoroscopy time, indistinctively from the TPT. Nonetheless, in our study, on multiple linear regression analysis, operator was not found to be an independent predictor of decreased OR time or fluoroscopy time (p < 0.05). As such, we feel that the TPT is a basic approach that may be easily adopted to reduce patient and staff exposure independently of clinical considerations.
Conclusion
The implementation of a “two-point technique” may significantly lower the amount of ionizing radiation delivered during ureteroscopy. This decrease can benefit patients and clinicians who are consistently exposed. Similar standardized techniques can be developed and applied on different urologic and nonurologic surgical procedures with potential advantages.
Footnotes
Author Disclosure Statement
No competing financial interests exist.