
Abstract
Purpose:
There has been an increase in the number of staghorn calculi that form in the absence of infection (metabolic staghorns). It is unknown why some large metabolic calculi form as solitary or multiple separate, nonbranching caliceal stones, whereas others develop as staghorn stones forming a cast of the collecting system. We sought to compare these two groups of metabolic stone formers (SFs) in an attempt to shed light on these disparate stone-forming phenomena.
Materials and Methods:
From January 2017 to September 2018, 190 patients underwent percutaneous nephrolithotomy for stones >2 cm. We identified 86 (45%) patients with a metabolic stone, defined as ≥80% calcium oxalate monohydrate or dihydrate and/or calcium phosphate. Exclusion criteria included stones composed of cystine, >20% uric acid, or any infectious element (struvite or carbonate apatite). Metabolic staghorn and nonstaghorn SFs were compared with respect to medical comorbidity, 24-hour urine parameters, stone and urine microbiology, stone compositions, and intraoperative findings. Statistical differences were assessed using chi-square analysis, Fisher's exact test, and Student's t-test.
Results:
In total, 25 (29%) staghorn and 61 (71%) nonstaghorn SFs were included for analysis. The groups were statistically similar in age, sex, body mass index, and medical comorbidity. Staghorn SFs had larger stone burdens (p < 0.0001), but did not require more punctures (p = 0.783). Staghorn SFs were more likely to have hyperoxaluria (p = 0.041) and higher mean 24-urine oxalate levels (p = 0.040). There were no other significant differences in 24-hour urine profiles, rates of metabolic abnormalities, stone compositions, stone or urine cultures, presence of collecting system obstruction, or pelvicaliceal anatomy.
Conclusions:
Although potentially driven by urinary oxalate, whether a metabolic stone will form into a staghorn configuration or not does not appear significantly influenced by standard determinants of stone development, including metabolic profile, cultures, hydronephrosis, and pelvicaliceal anatomy, among others. Further work is needed to elucidate the physicochemical factors that govern the pathogenesis of this increasingly prevalent entity.
Introduction
Although no consensus definition exists, a “staghorn” stone refers to any complex, branched calculus that grows to occupy multiple portions of a collecting system. By contrast, most stones commonly form within a minor or major calix and exhibit concentric-type growth. Traditionally, staghorn stones have been predominantly characterized as infection stones—composed of a mixture of magnesium ammonium phosphate (struvite) and/or calcium carbonate apatite. Although cystine or uric acid (UA) stones can also form staghorns, metabolic stones composed of calcium phosphate (CP) or calcium oxalate (CaOx) have been described to rarely grow in a staghorn configuration. 1
Contrary to conventional teaching, numerous reports suggest a contemporary shift in the composition of staghorn calculi favoring an increase in the prevalence of metabolic stones. 2,3 Recognition of such a trend is clinically impactful as the composition of these stones potentially influences medical management and surveillance, identification and amelioration of risk factors, and surgical decision-making. Whether or not increasing in prevalence, metabolic staghorn stones exist and present a challenging clinical situation. What is not known, however, is why some metabolic stones form in a branching, staghorn pattern, whereas others in a spherical or oval shape. We sought to compare these two groups of metabolic stone formers (SFs) in an attempt to shed light on these disparate stone-forming phenomena.
Materials and Methods
After institutional review board approval, we retrospectively reviewed the cases of all patients who underwent percutaneous nephrolithotomy (PCNL) for a renal stone >2 cm from January 2017 to September 2018. Recognizing that smaller stones attached to papillae may not have had time to follow one growth pattern or the other, we limited our review to large stones >2 cm. In total, 190 patients were identified, of whom 86 (45%) had a metabolic stone. These were defined as ≥80% CaOx monohydrate or dihydrate and/or CP. Stones composed of cystine, >20% UA, or any infectious element (struvite or carbonate apatite) were excluded from analysis.
Metabolic SFs were subsequently divided into two groups: (1) staghorn SFs and (2) nonstaghorn SFs. In this study, staghorn stones were defined as those occupying the renal pelvis and at least two calices in a branching configuration. Data available for evaluation included patient-related, stone-related, metabolic, microbiological, and intraoperative factors. Specifically, SFs were compared with respect to age, sex, medical comorbidity, 24-hour urine parameters, history of previous stone operation, stone and urine cultures, stone composition, number of calices punctured, collecting system anatomy, and presence of hydronephrosis.
Pelvicaliceal system (PCS) anatomy was defined by and stratified into one of the four types according to the Sampaio classification system, which has been previously described. 4 In brief, type A1 systems feature two major calices, one from each the upper and lower poles with drainage of the mid-pole region dependent on one or both of them. A type A2 PCS is similar with the exception that mid-pole calices cross each other—therefore, those draining into the upper pole major calix are more inferior within the kidney than the minor calices that drain to the inferior pole system. In a type B1 system, the mid-pole drains through a separate major calix, independent of the upper and lower pole groups. Type B2 features mid-pole minor calices that drain directly into the renal pelvis.
We routinely perform 24-hour urine tests (Litholink, Chicago, IL) in all patients within several weeks of stone treatment, before initiation of dietary modifications and/or medications. Appropriateness of specimen collections was determined by weight-based 24-hour urine creatinine levels (male: 18–24 mg/kg/day; female: 15–20 mg/kg/day). Only properly collected specimen results were included in the analysis. Metabolic abnormalities based on urine testing were defined as follows: hypercalciuria (>250 mg/day in men, >200 mg/day in women), hyperoxaluria (>40 mg/day), hypocitraturia (<450 mg/day in men, <550 mg/day in women), hyperuricosuria (>0.80 g/day in men, >0.75 g/day in women), hypomagnesuria (<30 mg/day), and hypernatriuria (>150 mmol/day).
Statistical analyses were performed using SPSS version 22.0 (SPSS, Inc., Chicago, IL). Patient characteristics were summarized with descriptive statistics. Differences in categorical variables were assessed using chi-square analysis and Fisher's exact test, and continuous variables using Student's t-test. Statistical significance was defined as a p < 0.05 and all tests were two-tailed.
Results
Overall, there were 25 (29.1%) metabolic staghorn SFs and 61 (70.9%) metabolic nonstaghorn SFs. The mean age of the cohort was 57.6 years; 54.7% were men. The two groups were statistically similar with respect to age (p = 0.900), sex (p = 0.872), body mass index (p = 0.536), and medical comorbidity. There were no differences in rate of collecting system obstruction (p = 0.337), PCS anatomy (p = 0.914), history of stones (52.0% vs 57.4%, p = 0.648), or history of a stone operation (34.8% vs 37.7%, p = 0.804). Among patients with a history of stones, the growth pattern of previous stones was known for 6 staghorn SFs and 21 nonstaghorn SFs. In the staghorn SF group, one patient had a previous staghorn, four had nonstaghorn stones, and one had a history of both. By comparison, in the nonstaghorn SF group, 2 patients had had a staghorn stone, 17 previously had nonstaghorn stones, and 2 had a history of both types. There was no difference in the presence of stone(s) in the contralateral kidney at the time of PCNL (21.7% vs 19.6%, p = 0.833), all of which were nonstaghorn stones. Staghorn SFs had larger mean stone burdens (43.6 mm vs 27.0 mm, p < 0.001), but did not require more percutaneous punctures (p = 0.783). Patient characteristics and perioperative factors are further given in Table 1.
Patient Demographics and Intraoperative Factors
BMI = body mass index; PCS = pelvicaliceal system; / = numerator/denominator; ± = mean ± standard deviation.
Stone composition
The breakdown of stone composition between the two cohorts was equivalent (Fig. 1). The majority of staghorn and nonstaghorn stones were predominantly (≥80%) CaOx—92.0% (23/25) vs 86.9% (53/61), respectively (p = 0.712). CP predominant (≥80%) stones were in the minority—4.0% (1/25) vs 4.9% (3/61), respectively. There were similar numbers of mixed CP/CaOx stones (1/25 vs 5/61, p = 0.667). UA-containing (≤20%) stones accounted for 24.0% (6/25) of staghorn and 9.8% (6/61) of nonstaghorn stones (p = 0.099).
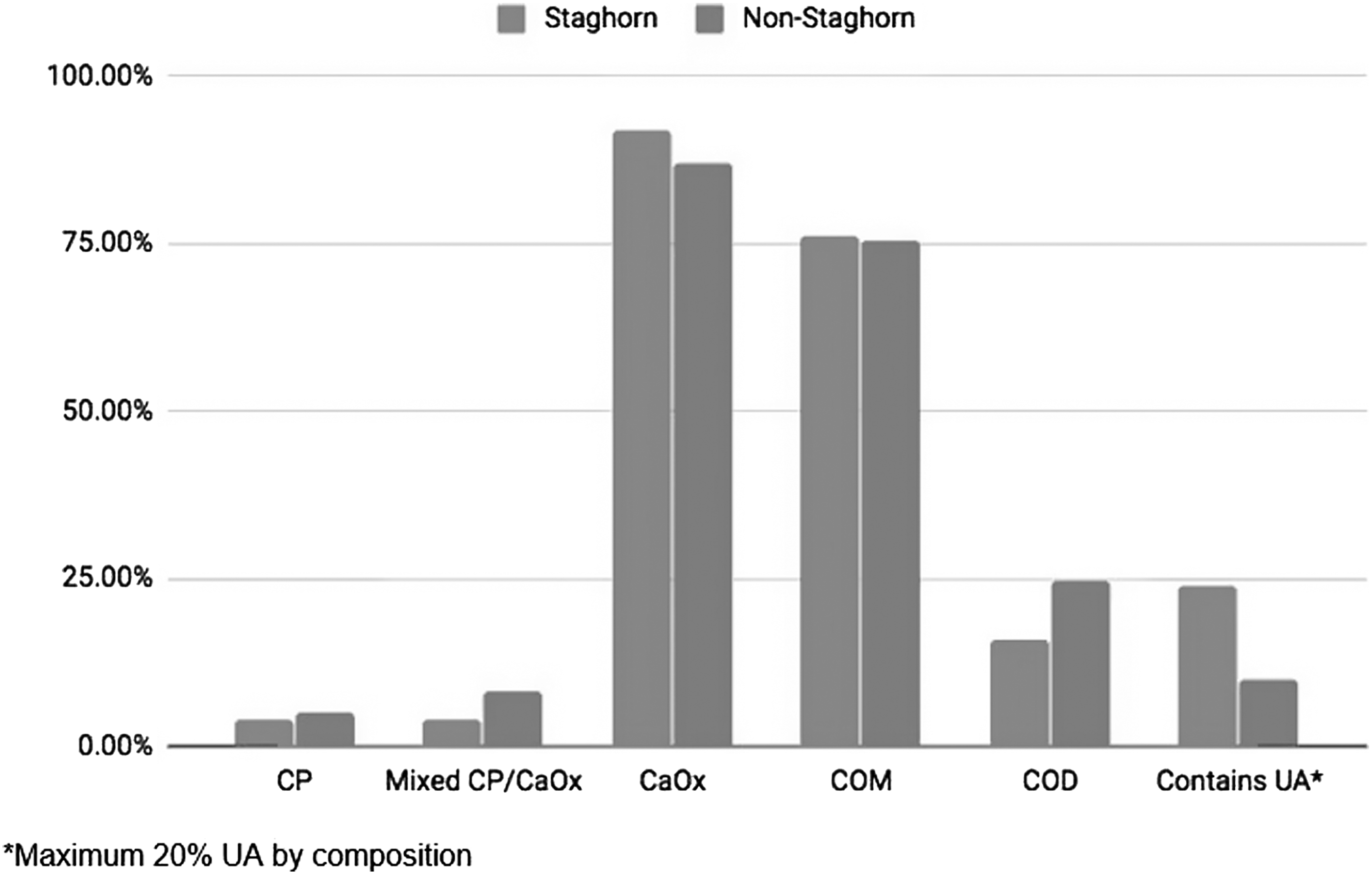
Breakdown of predominant stone compositions by group. *Maximum 20% UA by composition. UA = uric acid.
Metabolic parameters
Results of 24-hour urine testing were available in 18 (72.0%) and 48 (78.7%) staghorn and nonstaghorn SFs, respectively (p = 0.50). Table 2 provides an overview of the 24-hour urine test findings and metabolic abnormalities of the two groups. Staghorn SFs had higher mean 24-hour urine oxalate levels (46.56 vs 36.96, p = 0.040). All other 24-hour urine parameters were similar between the groups. The relative frequencies of various metabolic abnormalities were also statistically similar among the cohorts, including hypercalciuria (44.4% vs 27.1%, p = 0.112), hypocitraturia (38.9% vs 45.8%, p = 0.558), and hyperuricosuria (16.7% vs 16.7%, p = 0.815), among others. However, hyperoxaluria was the lone statistically different derangement occurring more frequently in staghorn SFs compared with nonstaghorn SFs (61.1% vs 33.3%, p = 0.041). There was no significantly different mean serum calcium level (9.0 mg vs 9.2 mg, p = 0.267).
Metabolic Evaluation Based on 24-Hour Urine Testing a
Patients with available 24-hour urine results: 18/25 (72.0%) staghorn vs 48/61 (78.8%) nonstaghorn, p = 0.50.
CaOx = calcium oxalate; CP = calcium phosphate; SS = supersaturation; UA = uric acid.
Microbiology
The two groups had similar proportions of positive stone cultures (4.0% vs 3.3%, p = 0.869), positive preoperative urine cultures (8.0% vs 8.2%, p = 0.976), and positive urine cultures within 12 months before operation (11.1% vs 29.0%, p = 0.274). Although positive stone cultures were uncommon, Escherichia coli was obtained from the one positive metabolic staghorn stone; Enterococcus faecalis and Streptococcus anginosus from the two positive metabolic nonstaghorn stones, respectively.
Discussion
Staghorn calculi have long been associated with the presence of infectious-related elements, including struvite and/or calcium carbonate apatite. By historical accounts, numerous investigators have reported that infection stones comprise a majority of staghorn calculi, ranging from 59% to 68% of cases. 5 –7 In fact, the 2005 American Urological Association (AUA) Guidelines support this claim. The Guidelines panel went on to state that metabolic stones, composed of CaOx or CP, only rarely grow into a staghorn configuration. 1 However, the findings of several recent studies suggest that the occurrence of metabolic staghorn stones is not only more common than once believed, but may be on the rise.
Mandel and colleagues 8 examined trends in kidney stone composition among patients in the United States National Veterans Administration system with new stone events between 1983 and 2003. From 1989 forward, they found a rise of up to 5.9% in the incidence of metabolic stones with a concomitant 2.6% decrease in infection stones. In 2011, Viprakasit and colleagues 2 reviewed their institutional cohort of staghorn patients reporting a large proportion of metabolic stones (29/52, 56%). In their sample, the majority of metabolic staghorns stones (16/29, 55%) were composed predominantly of CP. This is in contrast to our cohort of 25 metabolic staghorn patients, of whom only one patient had a CP composition. The majority of staghorn stones (23/25, 92%) in our study were predominantly CaOx, similar to our nonstaghorn cohort of metabolic SFs. At the 2017 AUA annual meeting, Haden and colleagues 3 presented their institutional experience with staghorn calculi from 2010 to 2015. Reviewing the cases of 71 patients who underwent PCNL for a complete staghorn, the authors reported that most patients had stones of metabolic composition. Specifically, 61% (44/71) of staghorns were metabolic stones. Similar to the cohort of Viprakasit and colleagues, most of these were composed of CP (52%), followed by CaOx (18%), UA (18%), and cystine (12%). This purported shift in staghorn stone compositions has been tied to a number of theories. Viprakasit and colleagues speculated that patient delay in seeking care until the development of a large stone burden or undertreatment of patients with metabolic stones (based on regional practice patterns) may contribute to the higher reported incidences. Others have cited contemporary trends in obesity, metabolic syndrome, and insulin resistance in the United States and their known associations to metabolic stone disease. 2,9 –12
Notwithstanding a possibly changing staghorn landscape, it remains unclear why some metabolic SFs develop oval or spherical stones, whereas others form branching staghorn calculi. Natural history studies demonstrate that undertreated and untreated metabolic caliceal stones that progress exhibit concentric-like growth. By comparison, staghorn stones follow a different pattern, progressively growing and branching to occupy the entire collecting system. 13,14 Although not specifically addressed in the literature, in our experience there is no crossover between these contrasting growth mechanisms within an individual stone. Whether an individual metabolic SF has the potential to grow both stone types metachronously remains to be determined.
Metabolic stones form by a number of mechanisms in association with various metabolic abnormalities. 15 Although having only 24-hour urine data available for 13 of 29 metabolic staghorn patients, Viprakasit and colleagues 2 identified elevated urinary sodium (69%), low urine volume (62%), hypocitraturia (46%), and hypercalciuria (46%) as the most common abnormalities in their cohort. By comparison, hyperoxaluria (61.1%), hypocitraturia (38.9%), hypercalciuria (44.4%), and elevated urinary sodium (44.4%) were most frequently seen in this study. Of note, metabolic staghorn SFs were more likely to have hyperoxaluria and significantly higher urine oxalate levels. It is well established that hyperoxaluria and hypercalciuria are important contributors to the development of metabolic stones in general, 16 but these findings may imply that oxalate is a driving factor for the development of larger stones in a staghorn pattern—greater severity of the metabolic abnormality may confer a greater risk of staghorn growth. Considering similar CaOx supersaturation between the two groups, it is unlikely that these metabolic factors alone drive staghorn formation.
The microbiological profiles of the two groups were similar with just three positive stone cultures across the entire cohort. This is not surprising as the development of metabolic stones is not traditionally associated with the presence of a urinary tract infection. E. coli was identified in the lone staghorn stone harboring bacteria. Only rarely producing urease, this common uropathogen is seldom implicated in the development of staghorn stones. 17 Viprakasit and colleagues 2 reported that 36% (5/14) of metabolic staghorn patients had a positive stone culture without specifying the organisms present. Furthermore, preoperative urine cultures were positive in 38% (11/29) of patients. Of interest, Haden and colleagues 3 found a relatively high rate of positive preoperative urine cultures (at least 36%) with E. coli being the most common isolate. Although observing a lower positive preoperative culture rate (8%), we too found E. coli to be the most common pathogen. Not overlooking the potential for gain-of-function mechanisms by classically nonurease-producing bacteria, 6 the relative infrequency of cultured bacteria in our study along with the known urinary milieu that propagates metabolic stone growth (as opposed to infection stones) limit the likely influence of these cultured organisms. We must also consider the possible role of other infectious or potentially lithogenic agents, including but not limited to nanobacteria and less common organisms that are more difficult to isolate by standard detection methods. 18,19
These findings demonstrate that metabolic staghorn growth is not influenced by anatomy, stone composition, bacteriology, or collecting system obstruction. It is apparent they initially develop in the presence of elevated urinary promoters common to all metabolic stones, although the relative influence of urine oxalate and calcium concentrations on staghorn-specific growth is unclear. Taken together, this suggests the presence of unknown or unmeasured factors that drive this growth pattern. The importance of uncovering this pathophysiology cannot be overstated. The relationship between infection staghorn stones and urease-producing bacteria was a practice-changing discovery. By the same logic, identification of the factors that predispose to metabolic staghorns holds the potential to alter our approach to screening, metabolic work-up, surgical management, surveillance, and prevention of further stone formation. Such implications are potentially significant, particularly in the face of rising incidences of metabolic staghorn stones.
This study is not without limitations. For one, we report on a relatively small number of patients because of the limited frequency of metabolic staghorn stones in clinical practice. Furthermore, all patients did not have 24-hour urine analyses, which may limit the strength of our metabolic profile comparisons. Relying on a retrospective review of cases, the factors available for evaluation are limited to those regularly collected in our practice, potentially omitting other variables that may hold significance. Of note, it is unknown whether patients with a history of stones had metabolic stones. However, to our knowledge this is the first study to critically evaluate metabolic staghorn stones in an attempt to identify the factors that predispose to their growth.
Conclusions
Metabolic staghorn SFs have higher levels of urine oxalate, but are otherwise similar to their nonstaghorn counterparts in terms of patient characteristics, stone composition, stone microbiology, and other metabolic parameters. Further work is needed to elucidate the unknown physicochemical factors that govern the pathogenesis of this increasingly prevalent, complex entity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.