
Abstract
Introduction:
Temperatures over 43°C—the threshold for cellular injury—may be achieved during ureteroscopic holmium laser lithotripsy. The time to reach and subsequently clear high temperatures at variable laser power settings and irrigation pressures has not been studied.
Methods:
A flexible or semirigid ureteroscope was placed within an 11/13 F ureteral access sheath inserted into a 250-mL saline bag simulating a normal-caliber ureter, renal pelvis reservoir, and antegrade irrigation flow. A thermocouple was placed adjacent to a 365 μm fiber fired for 45 seconds at 0.6 J/6 Hz, 0.8 J/8 Hz, 1 J/10 Hz, 1 J/20 Hz, and 0.2 J/80 Hz. Irrigation pressures of 200, 100, and 0 mm Hg were tested. Mean temperature changes were recorded with 6°C increase as a threshold for injury (as body temperature is 6°C below 43°C).
Results:
Semirigid scope: At 200 mm Hg no temperature changes >6°C were observed. At 100 mm Hg, changes >6°C occurred with 1 J/20 Hz within 1 second of activation and returned to ≤6°C within 1 second of cessation. At 0 mm Hg, changes >6°C occurred with all settings; within 1 second at power ≥10 W. Temperatures returned to ≤6°C within 5–10 seconds. Flexible scope: At 200 mm Hg, changes >6°C occurred at 1 J/10 Hz (15 seconds), 0.2 J/80 Hz (3 seconds), and 1 J/20 Hz (2 seconds). Temperatures returned within 6°C of baseline within 2 seconds. At 100 mm Hg, changes >6°C occurred in all but 0.6 J/6 Hz. Temperatures returned to ≤6°C in 5–10 seconds. At 0 mm Hg, all settings produced changes >6°C within 3 seconds, except 0.6 J/6 Hz (35 seconds). Temperatures returned to ≤6°C in under 10 seconds.
Conclusions:
High temperatures were achieved in our in vitro model in as little as 1 second at common irrigation pressures and laser settings, particularly with a flexible ureteroscope and power ≥10 W. However, with laser cessation, temperatures quickly returned to a safe level at each irrigation pressure.
Introduction
The holmium:yttrium-aluminum-garnet (Ho:YAG) laser is commonly used during ureteroscopy to treat urinary stones due to its ability to fragment nearly any stone with minimal risk of injury to the ureter. Newer, high-powered lasers allow for faster fragmentation or ablation of urinary stones, but this increased power adds increased risk of injury. Due to their photothermal mechanism of lithotripsy, Ho:YAG lasers can produce significant heat, risking thermal injury to the ureter even without direct contact between the laser fiber and the ureteral wall. 1 –5 The threshold for cellular thermal injury, 43°C, has been shown to be exceeded using conventional, relatively low power laser settings in bench-top models of a renal calix and a ureter. 2,5 The magnitude of heat production, and therefore the potential for injury during ureteroscopic lithotripsy, is impacted not only by laser pulse energy and frequency, but duration of laser activation and flow of irrigation. 5 To date, no studies have demonstrated the relationship between heat production and the variables under direct control of the urologist: laser energy, activation time and irrigation pressure. Our aim was to determine the time required to reach and subsequently clear intraureteral temperatures over 43°C at a variety of laser and irrigation settings using both a flexible and semirigid ureteroscope in a bench-top ureteral model.
Methods
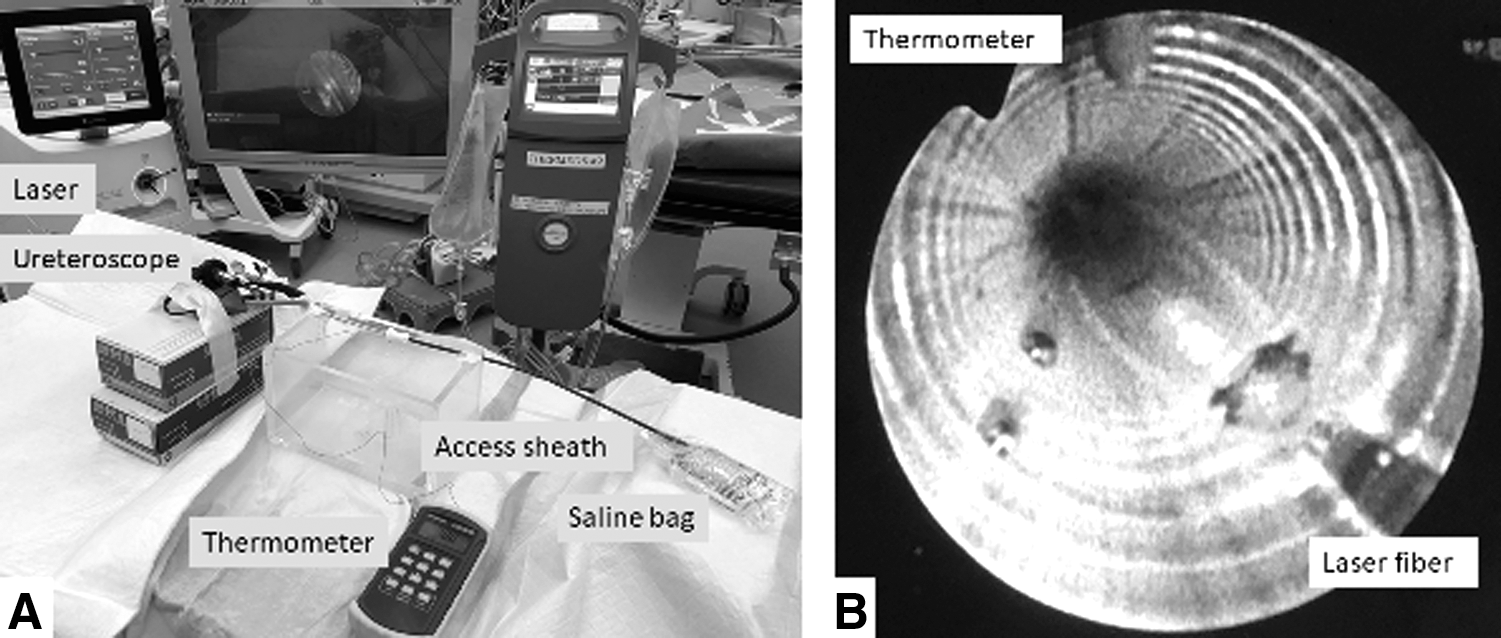
A digital flexible ureteroscope (Lithovue; Boston Scientific, Marlborough, MA) or a 33 cm, 6.4F semirigid ureteroscope (OES Pro; Olympus, Tokyo, Japan) was placed 15 cm into a 36 cm, 11/13F ureteral access sheath (Navigator; Boston Scientific) to simulate the ureteroscope position for a mid-ureteral stone. To simulate the reservoir effect of the renal pelvis and calices, the proximal end of the access sheath terminated in a full 250-mL saline bag (Fig. 1A). Room temperature 0.9% saline irrigation was delivered through the working channel of the ureteroscope at pressures of 200, 100, and 0 mm Hg using a programmable fluid management device (FluidSmart; Thermedx, Cleveland, OH). Flow rate at these irrigation pressures was calculated by timed capture of irrigation exiting the distal end of the access sheath into a graduated receptacle. A wire thermocouple (Omega Engineering, Norwalk, CT) was placed within the ureteral model 3 mm adjacent and parallel to the tip of a 365 μm laser fiber, which was initially passed through the working channel of the ureteroscope until the tip could be seen within the ureteral model lumen using the optics of the ureteroscope (Fig. 1B). A 120 W Ho:YAG laser (Pulse 120H; Lumenis, Yokneam, Israel) was used to deliver laser energy at settings of 0.6 J/6 Hz, 0.8 J/8 Hz, 1 J/10 Hz, 1 J/20 Hz, and 0.2 J/80 Hz for 45 seconds each. The system was allowed to equilibrate with each new irrigation pressure for 30 seconds before each run, with the exception of those runs with no pressure. For those runs, irrigation was delivered at 200 mm Hg for 30 seconds to allow the model to fill, then the irrigation arrested by a stopcock and laser firing immediately commenced. Two runs per laser energy setting, irrigation pressure, and ureteroscope type combination were completed. Mean temperature change from baseline was recorded at 1-second intervals during laser activation and for 15 seconds after cessation. Six degree Celsius above the baseline temperature was chosen as the threshold for potential ureteral injury as 43°C is 6°C greater than normal body temperature of 37°C.
Results
At an irrigation pressure of 200 mm Hg, none of the tested laser energy settings generated a temperature increase 6°C or more over baseline using a semirigid ureteroscope (Fig. 2A). Using the flexible ureteroscope, laser settings of 1 J/20 Hz and 0.2 J/80 Hz surpassed the 6°C threshold within 2 seconds of activation and reached a maximum of 14°C and 9.5°C above baseline, respectively. Laser settings of 1 J/10 Hz also surpassed 6°C above baseline after 15 seconds of continuous activation, and maximum temperature increase was 7°C above baseline. After stopping laser activation, all three settings returned to below the 6°C threshold within 2 seconds (Fig. 2B).
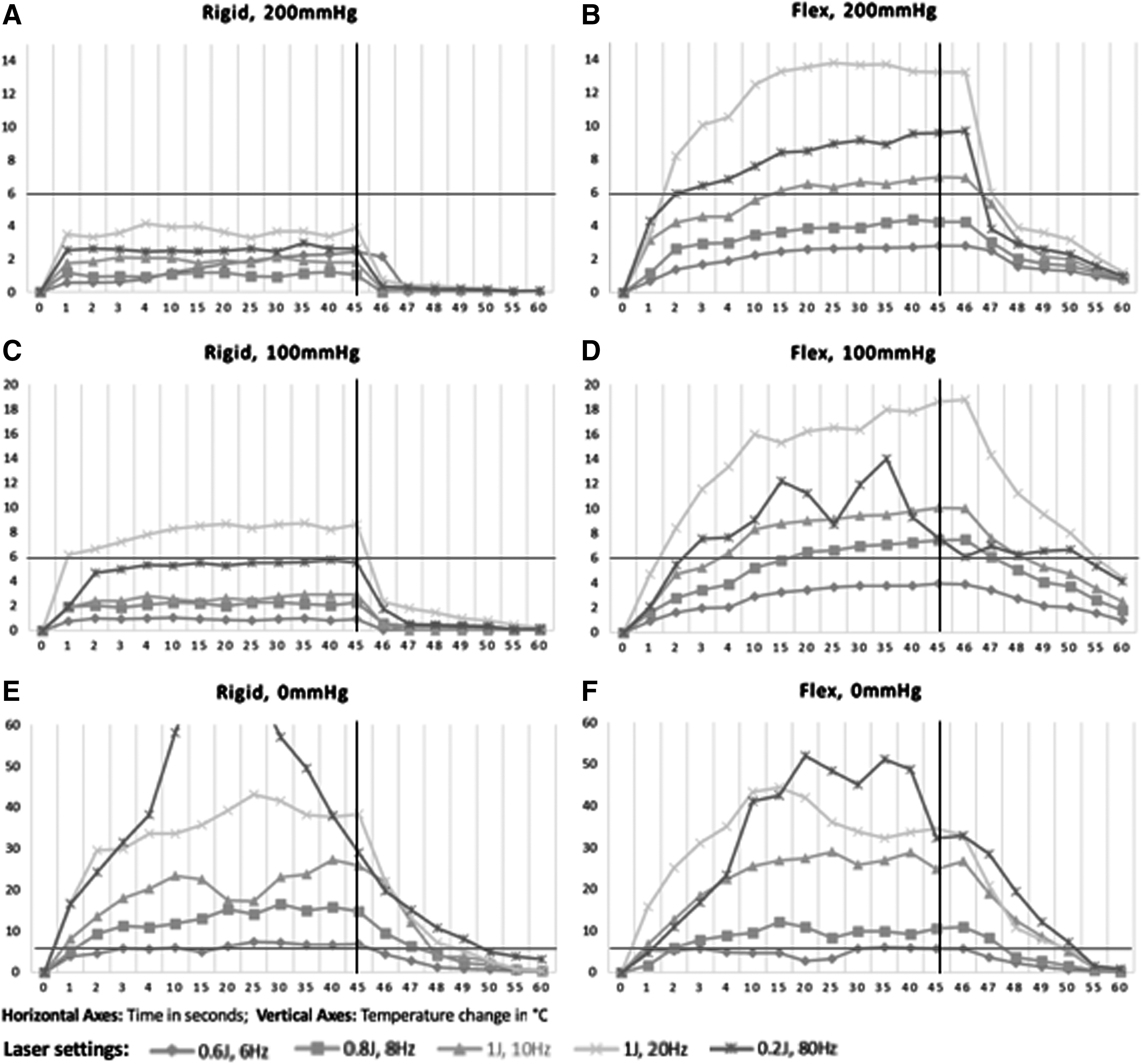
Mean temperatures produced during holmium:yttrium-aluminum-garnet laser firing in a ureteral model at various laser settings, irrigation pressures, and ureteroscope types. Semirigid ureteroscope irrigation pressures of
At an irrigation pressure of 100 mm Hg in the semirigid scope, 1 J/20 Hz was the only laser setting to produce a temperature rise over 6°C. This occurred within the first second of activation and reached a maximum of 9°C above baseline. The temperature returned to near baseline levels within 2 seconds after laser cessation (Fig. 2C). In the flexible scope, all laser settings other than 0.6 J/6 Hz produced temperature rises at least 6°C over baseline. This occurred within 4 seconds of laser activation at 1 J/10 Hz, 0.2 J/80 Hz, and 1 J/20 Hz. At 1 J/20 Hz, the maximum temperature rise over baseline was 19°C which required 10 seconds to return below the 6°C threshold after laser cessation (Fig. 2D).
With no irrigation inflow through the semirigid ureteroscope, all laser settings produced temperature rises greater than 6°C over baseline. The threshold was surpassed in under 1 second at higher power settings but remained at ∼6°C over baseline for the duration of the run at 0.6 J/6 Hz. Settings of 0.2 J/80 Hz produced a maximum temperature increase over 60°C after about 20 seconds of activation. Following laser cessation, temperatures dropped below the 6°C threshold within 5 seconds (Fig. 2E).
Using the flexible scope and 0 mm Hg irrigation inflow, all laser settings produced temperature rises greater than 6°C over baseline with higher power settings climbing to an excess of 20°C above baseline within the first 4 seconds. Settings of 0.2 J/80 Hz produced a maximum temperature increase over 50°C after about 20 seconds of activation. Following laser cessation, temperatures dropped to or below the 6°C threshold within 5 seconds (Fig. 2F).
Mean irrigation flow rates at the three pressure settings for each ureteroscope are listed in Table 1.
Measured Irrigation Flow Rates at Various Pressures Applied Through Flexible and Semirigid Ureteroscopes with 365 μm Laser Fiber in the Working Channel
Discussion
High-powered lasers have created new opportunities for the treatment of urinary calculi. Not only can these newer lasers deliver high energy per pulse to quickly fragment hard stones, but they can also produce high frequencies that enable the urologist to “dust” a stone rather than fragment it and potentially obviate the need for basket extraction of larger fragments. 6 The heat production that comes hand in hand with the photothermal mechanism of lithotripsy of the Ho:YAG laser was well described nearly two decades ago. 7 However, it is only in recent years that Ho:YAG lasers with the ability to deliver high energy, high frequency, and potentially high heat have become clinically available for lithotripsy.
Thermal injury to tissue can occur at any temperature above 43°C, 8 however, the degree of injury is dependent on both temperature and time of exposure. The time of exposure for any given temperature to produce irreversible damage can be estimated; over small intervals it generally follows that for every degree above 43°C, the time required for injury is reduced by 50%. 9 For example, tissue lethality requires 120 minutes of exposure at 43°C, but only 7 seconds at 53°C.
This is the first bench-top study to investigate clinically practical parameters of ureteroscope type and irrigation pressure on the rate of heat production and subsequent dissipation during Ho:YAG laser activation. Additionally, we created a unique bench-top ureteral model designed to mimic the filling of the renal pelvis and antegrade outflow of irrigation that is experienced clinically. We found that traditional low-power laser lithotripsy settings, such as 0.6 J/6 Hz and 0.8 J/8 Hz, can produce temperature elevations equal to or in excess of 6°C within our ureteral model. However, the risk for injury at these settings under average clinical conditions is minimal. Even with moderate irrigation pressure (100 mm Hg) and low flow in a flexible ureteroscope, 0.8 J/8 Hz required at least 15 seconds of continuous activation to reach the minimum threshold for injury. Assuming the use of physiologic irrigant at 37°C and the principles described by Sapareto and Dewey, 9 exposure time for injury in this scenario would be ∼10 minutes. The use of irrigation at temperatures <37°C would further prolong the exposure time for any potential thermal injury. These requirements for extreme circumstances of laser activation and irrigation to create thermal injury are in agreement with several large series demonstrating the de novo stricture rate after ureteroscopic Ho:YAG laser lithotripsy to be <2%. 10 –13 Notably, these reports utilized settings similar to the lower power settings tested in this study, with total power output of 3.6–10 W with rare escalations to 15 W.
Higher power laser settings produce more dramatic temperature elevations. The shorter length and larger working channel of the semirigid ureteroscope results in over three-fold increased flow relative to the flexible ureteroscope, maintaining safe temperatures at all tested laser energies with irrigation pressure of 200 mm Hg. At moderate irrigation pressures of 100 mm Hg, 1 J/20 Hz produced high temperatures, but this was limited to a maximum of 8°C above baseline, which would require roughly 30 minutes of exposure to produce injury. Using the flexible ureteroscope, high-power laser fragmentation and dusting settings created temperature elevations over 6°C even with high irrigation pressure. Settings of 1 J/20 Hz and 0.2/80 Hz created rapid temperature increases, surpassing the 6°C threshold in the first 2 seconds. However, each setting quickly plateaued at levels, which under usual conditions, would require exposure times in excess of 5 minutes for significant injury. At moderate irrigation pressure however, 1 J/20 Hz reached maximum temperature elevations above baseline with the potential for thermal injury after only seconds of exposure. Fortunately, these temperatures were achieved only after 10 seconds or more of continuous laser activation.
In both ureteroscopes with no irrigation pressure, the higher power laser settings quickly created temperature elevations in excess of 20°C over baseline, where there is potential for subsecond exposures to induce tissue injury. Temperature decreases to below the threshold for injury following laser cessation were delayed at least 5 seconds or more, emphasizing the safety role of irrigation during laser use. Interestingly, 0.2 J/80 Hz was observed to create higher maximum temperatures than 1 J/20 Hz in this zero irrigation pressure setting, despite the 4 W higher power in the latter. The etiology of this phenomenon is unclear, but suggests that increased caution regarding potential thermal injury is advised if high-frequency settings are used in no or low irrigation scenarios.
Our results add to the existing data on the thermal properties of Ho:YAG laser lithotripsy. Using a glass test tube submerged in a 37°C bath as a caliceal model, Hein and colleagues 4 demonstrated temperatures as high as 68°C when using high-power laser settings of up to 100 W without irrigation. In a similar bench-top set-up, Aldoukhi and associates 2 demonstrated maximum temperatures of 69.8°C without irrigation and 40 W of laser energy. They went on to further test their findings in vivo using pigs and found peak temperatures 15°C higher than in their bench-top model and observed tissue charring of the calix and renal parenchyma on gross pathologic exam. 1 Before this, the heat sink effect of the highly vascular renal parenchyma was hypothesized to be protective against the generation of high temperatures. As the authors suggest, it is likely that the heat generated by high-power Ho:YAG lasers accumulates quickly and overwhelms any heat sink effect of the renal parenchyma. Reduced irrigant flow in vivo likely contributed to the observed higher temperatures relative to their bench-top model.
The potential for urinary system injury is likely worse in the ureter relative to a renal calix as there is less surrounding vasculature to provide any possible heat sink, the narrow lumen reduces the flow of irrigation, and increases the risk of circumferential injury and subsequent stricture formation. This has been illustrated by Molina and colleagues, 14 who demonstrated thermal spread of at least 1 cm from the tip of a 365 μm laser fired at 10 W for just 3 seconds in a sheep ureter. Additionally, it is tempting to limit or stop irrigation during ureteroscopic lithotripsy to decrease stone migration proximally up the ureter and away from the laser. Our group has previously demonstrated that high-power laser settings can create high temperatures in a bench-top model and that judicious use of irrigation can mitigate heat production. 5 The current study builds off this work by employing an improved ureteral model which is more representative in caliber (11/13F vs 15F), includes a ureteroscope for delivery of irrigation and obstruction of its outflow, and adds a small-volume reservoir to mimic the natural filling of the renal pelvis and antegrade flow of fluid observed clinically. Additionally, in the current study, we emphasize irrigation pressure rather than flow, as pressure is the variable directly manipulated by the operating urologist during ureteroscopy.
Although smaller diameter fibers are often used during ureteroscopy, we chose to use a 365 μm fiber as its larger diameter restricts the flow of irrigation through the ureteroscope more than a small 200 or 272 μm fiber 15 and thus provides the most conservative extrapolation to clinical scenarios. However, if the urologist decreases the flow of irrigation to reduce stone movement or urinary system pressure, the size of the fiber is less significant. Additionally, 365 μm or larger fibers are the referenced fiber size in many reports on the safety of ureteroscopic laser lithotripsy. 10 –13 For some centers there may even be an incentive to use larger fibers as they are more durable 16 and thus may represent a cost saving relative to smaller fibers. Although there is controversy over whether larger fibers create more or less heat than smaller fibers, what differences exist between fiber sizes appear relatively subtle relative to the impact of irrigation. Hein and colleagues 4 tested 272 and 940 μm laser fibers in a test tube model and found the smaller fiber generated higher temperatures, although no statistical analysis of the difference is reported and the measured energy output for each fiber did not appear equivalent. Butticè and colleagues 3 observed more rapid temperature elevation during laser activation in a kidney model using a 272 μm compared with a 200 μm fiber, however, maximum temperature was not different between the two fibers. Importantly, any difference between the fibers was lost when continuous irrigation was applied.
Previous work on this subject both at our center and others have suggested increased irrigation and avoidance of prolonged laser activation as mitigating strategies to address high-power laser-generated heat. Stone retropulsion and increased renal pressures leading to increased rates of postoperative infectious complications limit irrigation as a solitary solution. Our results support limiting activation time provided there is some irrigation present. If irrigation is held, even a few seconds of lasing can create high temperatures when power is over 10 W. Limiting activation time by using short bursts of laser energy may not be adequate as a single strategy either. Our results suggest somewhat long intervals, 3–5 seconds of cessation, may be required to clear high temperatures. More significantly, multiple short exposures to elevated temperatures have been shown to be injurious to tissues when the interval between exposures is brief as the case may be during ureteroscopic laser lithotripsy. 17 Based on these results, if laser power over 10 W is to be used in the ureter, we suggest a combination strategy of (1) at least moderate irrigation, (2) limiting laser activation to 3–4 second bursts with 3–4 second pauses between to allow temperature normalization and (3) consideration of reversion to lower power settings if a prolonged procedure is expected. Finally, the use of cooled or nonwarmed irrigation can also be considered to add an additional margin of safety.
There are several limitations to recognize in this work. First, we report our results as temperature changes from baseline and acknowledge that a temperature elevation of 6°C will not equate to an intraureteral temperature of 43°C in vivo, except under a perfect set of circumstances. Intraureteral temperature is a complex result of the starting temperature of the irrigation, its flow rate, and any heating or cooling that may occur from contact with the patient's tissues. The use of continuous vs pulsed irrigation may additionally have unique impacts on laser-induced heating. Second, we recognize that the use of high-power laser settings during ureteroscopy is rare in contrast to their use in the bladder or the renal pelvis. However, as discussed above, newer lasers are not only more powerful, but they can generate high frequency. A relatively low pulse energy combined with a very high frequency results in the delivery of a large amount of power. As low pulse energy, high frequency stone ablation, or “dusting,” of stones continues to gain popularity, there may be urologists who use settings with power over 10 W in the ureter to try to avoid opening expensive disposable equipment such as a basket. The addition of new endoscopic technology, such as robot-assisted ureteroscopy, may also increase the urologist's confidence regarding aim and ability to maintain contact with the stone such that dusting within the ureter becomes more attractive. Additionally, our model does not incorporate a stone. Lithotripsy implies the presence of a stone and as the intended target of laser energy, the stone material will absorb laser energy that would otherwise contribute to heat production. Lee and associates 18 demonstrated that the force of ejected fragments from the stone surface is the primary contributor to stone retropulsion during lithotripsy and, thus, by the law of conservation of momentum, some laser energy must be converted to this mechanical energy, rather than heat. However, given the impact of irrigation flow demonstrated in this study and by others 1 –3,5 the limitation of flow by stone material may create a counterintuitive increase in laser-related heat production. Indeed, the presence of stone material has been demonstrated in another bench-top study to increase laser-generated heat by up to 12%. 4 Further study with stone material of varying size and composition is required. Finally, this is an in vitro bench-top study. Further study is needed in vivo to better demonstrate temperature generation, dissipation, and actual thermal tissue injury.
Conclusions
Temperatures over the threshold for cellular injury were achieved in our in vitro model in as little as 1 second at common irrigation pressures, particularly when using a flexible ureteroscope and laser settings ≥10 W. These high temperatures returned to a safe level within 5 seconds at each irrigation pressure. Judicious use of irrigation, limited activation time, and adequate time between laser activations may decrease the risk of thermal injury if high-energy laser lithotripsy is pursued in the ureter.
Footnotes
Acknowledgments
This work was supported in part by the Urology Care Foundation Research Scholar Award Program and AUA Southeastern Section. The content is solely the responsibility of the authors and does not necessarily represent the official views of the American Urological Association (AUA) or the Urology Care Foundation.
Author Disclosure Statement
B.W., D.W., E.C., C.P., J.L., R.T., K.B.: No competing financial interests exist; G.M.P. and M.E.L.: Consultant: Boston Scientific.
Funding Information
No funding was received for this article.