
Abstract
Percutaneous nephrolithotomy (PCNL) is the current gold standard for the treatment of large and complex renal stone disease. It is a complex procedure that requires skill and experience. The most challenging step and key requisite of a successful PCNL is establishing optimal access to the renal collecting system with imaging modalities. To increase safety and efficacy in this crucial step, and with ongoing advancements in current technology, several aids have been developed to assist the urologist and help accurately guide the needle to the target. The goal of this systematic review was to identify and discuss these innovations.
Introduction
In the last 40
The most challenging step of a successful PCNL is establishing optimal access to the renal collecting system 7 —even the universally adopted safe puncture through the papilla has been recently challenged. 8 Inadequate access may traumatize surrounding vessels, resulting in the aforementioned complications and significantly compromising the outcomes of the procedure. Noteworthy, in a recent Premier Healthcare Database study, Speed and colleagues concluded that access-related complications were higher when done by a radiologist compared with when performed by a urologist. However, only 17% of urologists in the United States obtain their own access. 9 This may be explained by a lack of training, among other reasons. 10
Previous literature reviews of innovation in PCNL did not exclusively look at intraoperative tools facilitating access. 11 –15 One of these reviews by Tailly and Denstedt noted that many of these new needle-guiding modalities were still in an experimental phase in 2016 14 ; an important focus of our review is to determine if any further research has evaluated their potential use in urologic clinical practice.
To reduce complication rates and improve outcomes of PCNL, it is imperative to develop assistive technologies that leverage and enhance urologists' existing skill and knowledge of PCNL. We sought to conduct a systematic review of available assistive technologies facilitating access in PCNL to inform urologists of existing resources.
Methods
Inclusion and exclusion criteria
For our inclusion criteria, we defined assistive technologies facilitating PCNL access as any form of hardware or software developed for or adopted to complement the needle access of the kidney in the PCNL procedure. Published studies with full text available in a journal or as a scientific abstract that met the aforementioned definition were included.
The above definition excludes new kidney stone removal techniques, preoperative planning, and non access-related innovations for PCNL. Furthermore, tools that were not explicitly developed for improving PCNL access but that may influence access, such as miniaturization of equipment, were not included.
Search strategy
A literature search was performed for all included studies published between October 1997 and December 2018, in the PubMed and Web of Science databases.
The inclusion criteria included studies matching the following key phrases in a computerized literature search: technology, technologies, software, guide, guided, robotic, assisted, alongside the key phrases (“Nephrolithotomy, Percutaneous”[Mesh]) AND access, or PCNL AND access. We further performed a crossreference search to include articles not found in the database search matching our criteria and search keywords.
Review methods and data synthesis
From these searches, 73 citations were retained from abstract screening. Two authors performed the study selection independently (D.-D.N. and J.W.L.). Disagreements were resolved by consensus with the senior author (N.B.). Titles and abstracts were used to screen for initial study inclusion. Full-text review were used if abstracts were insufficient to determine if the study met inclusion or exclusion criteria. Twenty-three studies were excluded, as they did not fit the inclusion criteria or were a match for the exclusion criteria, for a total of 50 studies. Figure 1 provides additional details on the selection process.
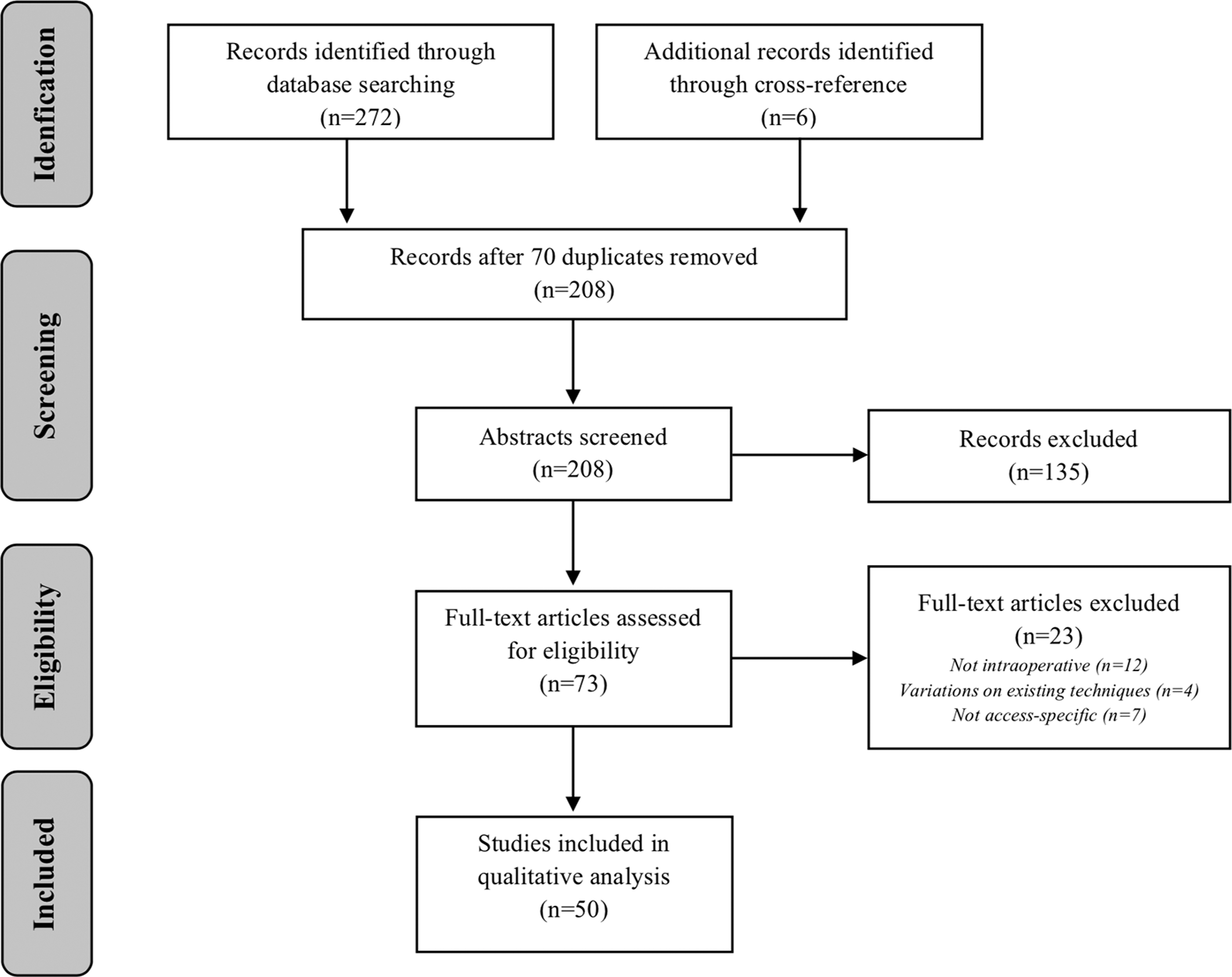
Article selection methodology.
These articles were subdivided based on the imaging modality (ultrasound [US], fluoroscopy, CT, electromagnetic tracking [EMT]), or a combination of multiple modalities. Robotic devices relying on imagery were included in the corresponding imaging modality. Purely robotic devices that did not rely on imaging were classified separately. For technologies and approaches with multiple articles, only the most recent or most relevant articles were cited in this review (which is why not all 50 studies retained are outlined in this review). Systematic and literature reviews were classified separately and not reported in this review, with key articles identified by these studies included in the crossreference search.
Results
US-based innovations
An overview of the technologies reviewed can be found in Table 1. In recent years, US guidance has increasingly been utilized as it provides real-time imaging, is relatively easy to use, allows for accurate visualization of surrounding organs, and reduces radiation exposure to the patient, surgeon, and staff. However, it presents with two major challenges that hinder its widespread adoption: (1) clear imaging of the kidney with accurate interpretation as well as (2) visualization of the needle and coordination of the needle hand with the imaging hand to advance the needle within the imaging plane into the chosen renal target. 16 The first challenge pertains to knowledge and additional learning, whereas the second pertains to practice and dexterity. Several groups have demonstrated that US-guided renal access for PCNL requires a learning curve of 20 to 60 cases. 16,17 With that said, most intraoperative assistive tools seek to tackle the second more technical challenge of US-guided PCNL access.
Overview of PCNL Access Technologies Reviewed
ANT-X = Automated Needle Targeting with X-ray; AR = augmented reality; CT = computed tomography; DARRT = direct alignment radiation reduction technique; EMT = electromagnetic tracking; MAG = mini access guide; PAKY = percutaneous access to the kidney; SAVN = surgical approach visualization and navigation; VR = virtual reality.
Projection of the puncture tract
The low echogenic profile of the needle tip makes puncture tract visualization and needle observation a challenge. This may prolong procedures (i.e., multiple attempts until an adequate puncture is obtained) or result in procedure failure or complications (e.g., puncture of vessels). 18
Already in 2007, Mozer and colleagues suggested using computerized methods to project an US-generated puncture tract onto the fluoroscopic images. 19 Retaining the idea of projecting the tract, recent innovations have completely removed the need for fluoroscopy when employing US-guided access. These computer-assisted visualization systems display the needle trajectory on the US monitor. Although each device possesses different specifications and design, the underlying principle is the same: a system tracts the spatial position of the needle in relation to the US probe and projects an estimated trajectory of the needle on the US screen display.
In this review, we identified ClearGuideOne (Clear Guide Medical, Baltimore, MD) and SonixGPS (UltraSonix, Richmond, BC, Canada) as the main commercialized tools offering such projections of the puncture tract in urology. ClearGuideOne employs a dual lens camera optically tracking the external portion of the needle, 18 whereas SonixGPS employs multiple position sensors, including one embedded in the transducer and another in the needle (Fig. 2). 20 –22 UProbe-2 (Sonostar Technologies CO, Guangzhou, Guangdong, China), a more recent innovation, integrates within a single probe a needle trestle and the system used to project the puncture tract while wirelessly connecting to intelligent terminals. 23

Ultrasound guidance systems: Clear Guide One (left and middle) and SonixGPS (right).
Outcomes of ClearGuideOne
In a randomized crossover bench-top trial comparing to conventional access, Thomas et al. concluded that ClearGuideOne significantly reduced the total procedure time from 192.9 to 94 seconds and the time to hit the target from 121.6 to 62.5 seconds in their combined dataset. The overall success rate in reaching the target under 5 minutes was significantly better (81.7% vs 98.6%, p < 0.001) with the add-on of this novel technology, regardless of the level of experience. This add-on potentially reduces the learning curve and can possibly motivate urologists with less US experience to obtain their own renal access during PCNL. 18
Limitations of ClearGuideOne
A limitation of ClearGuideOne is that needles smaller than 20-gauge may deflect inside the patient creating a discrepancy between the calculated and actual needle path. Needle trajectory mapping is also affected by fluid or fingers obstructing the camera's view (reducing the accuracy). 18
Outcomes of SonixGPS
In a 2014 study, Li et al. observe a mean puncture time of 7.73 minutes and a total procedure time of 72 minutes with 50 patients when using SonixGPS, as opposed to the puncture time of 12.42 minutes and procedure time of 86 minutes for the conventional US with 47 patients. 20 A follow-up study in 2017 by the same group obtained a mean puncture time of 6.62 minutes and a mean procedure time of 73 minutes on 37 patients with the SonixGPS technology. 21 Similarly, Li and coworkers obtained a mean puncture time of 5.5 minutes on 25 patients. 22 SonixGPS demonstrates reduced puncture time, slightly faster procedure time, decreased attempts for successful puncture, and decreased blood loss in the case match study comparison to conventional US access. 21
Limitations of SonixGPS
The needle beam alignment and calibration, necessary for proper functioning of SonixGPS, requires further training and involves an extra step compared with conventional US. Lack of dual optical tracking also makes SonixGPS a less friendly approach compared with ClearGuideOne for urologists less experienced with ultrasonography. 20 –22
3D ultrasound
The underlying technology behind real-time 3D US is based on the principle of stacking multiple transverse sections through the use of 2D array transducers, or through automated motion of a regular transducer with translation, tilting, or rotation. Although the concept of stacking cross-sections into volumes is not new, the volume reconstruction following data acquisition used to be a major technical barrier. Recent technological advances now enable relatively fast 3D volume reconstruction, thus enabling the surgeon to gain depth perception during PCNL at the expense of a slower refresh rate compared with traditional US. 24
In an animal study on beagles, Hongzhang and coworkers demonstrated that the use of 3D US significantly decreased the time (7.3 seconds vs 21.4 seconds, n = 16) and number of puncture attempts (1 vs 2.1, n = 16) needed to puncture the renal collecting system compared with standard 2D US. 25
Contrast-enhanced US
Cui and associates demonstrated a 100% puncture success rate (n = 45) with the use of intracavitary contrast-enhanced US (ICCEUS). 26 The use of a contrast agent, consisting most commonly of an IV injection of microscopic gas bubbles, increases the amount of backscatter and thus allows for a final image with increased contrast. The use of contrast allows for an increased acuity with organ edge or lesion detection, but the advantage of contrast-enhanced US over noncontrast-enhanced US for PCNL has not been determined.
Fluoroscopy-based innovations
Fluoroscopy-guided PCNL with the patient in the prone position is a well-established modality generally preferred by urologists for obtaining percutaneous access for PCNL. In a 2017 internet-based survey, access was achieved under fluoroscopic guidance by 75% of members of the Endourological Society. 27 Fluoroscopic approaches present a set of challenges such as the visualization of a 3D structure using a 2D image and exposure to radiation. Innovations facilitating fluoroscopy-guided access to the kidney thus seek to facilitate image interpretation and puncture precision (reducing the number of attempts needed to gain optimal renal collecting system access).
Computer-assisted targeting
Computer-assisted fluoroscopy innovations are built upon existing techniques, such as triangulation and the bullseye technique, while taking away the challenges of visualizing the puncture tract and stabilizing the needle while puncturing.
Using the principle of triangulation, Zarrabi and associates developed a lightweight and portable mechanical gantry paired with computer-assisted targeting. 28 After obtaining one image at 0° and another at 20° with the fluoroscopic C-arm, they relayed the images to a software where the surgeon can select the targeted calix. The software then outputs the settings to which the gantry should be set to perform the optimal PCNL puncture tract. Once the needle is placed on the adjusted gantry, the needle is advanced by the urologist at the depth indicated by the device. Zarrabi and colleagues' main goal was to demonstrate the possibility of targeting the kidney and possibly intended to pair this innovation with automatic needle drivers, as they were aware of the existence of such devices. In porcine and plastic models, accurate puncture was obtained in 15 and 10 minutes, respectively, with 100% success rate in both. As C-arm fluoroscopy only required two images, radiation exposure was significantly reduced (no specific exposure times presented). Despite the low cost of their approach (1500$, and a custom Python script for the algorithm), no further studies have been done on their custom technique.
Similarly, but using the bullseye technique, Oo et al. developed the Automated Needle Targeting with X-ray (ANT-X). 29 ANT-X (Fig. 3) employs image coregistration software to automatically align the puncture needle to the desired calix using the bullseye technique. The surgeon selects the desired calix and places a skin stab incision over the area where the needle gantry ring with a mounted needle will be positioned. Once the images are obtained, ANT-X integrates them with the real-time position of the needle and automatically aligns it. The surgeon then proceeds to gain access by pushing the stabilized and positioned needle. Fluoroscopy with C-arm at 0° is used to gauge the depth of puncture. On the porcine model, ANT-X reduced radiation exposure by 26% compared with the free-hand technique and required 3.15 minutes. In the human trial, obtaining percutaneous access was successful on first attempt in 3.05 minutes.
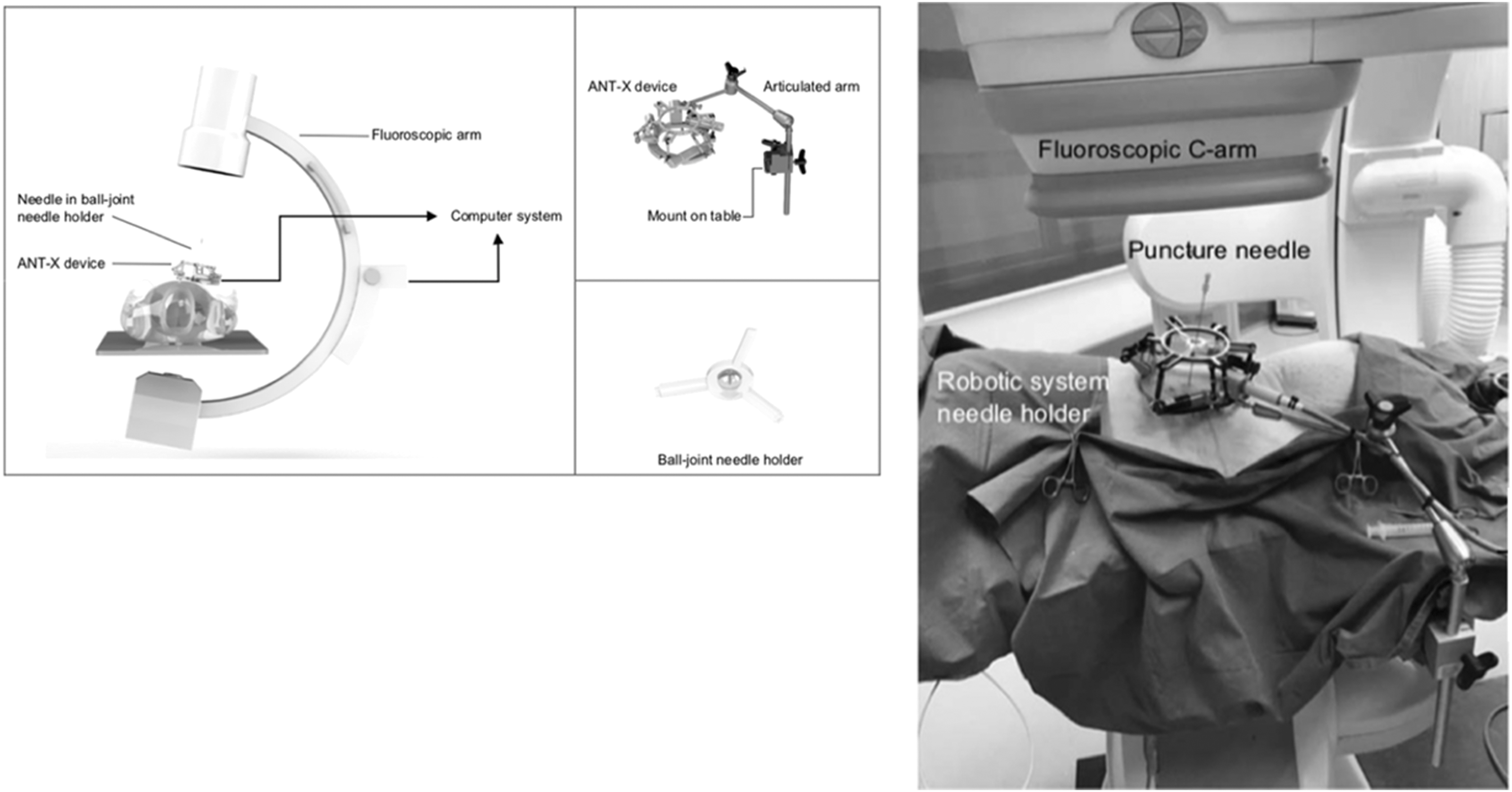
Computer-assisted targeting: ANT-X schematic (left) and porcine model setup (right). ANT-X = Automatic Needle Targeting with X-ray.
Limitations of computer-assisted targeting
Limitations of this system include accounting for respiratory movements; although the system can obtain access in less than a minute during respiratory suspension, obstacles such as a rib might require that respiratory suspension be halted and alignment be restarted. This procedure also relies on fluoroscopy with its inherent radiation exposure.
Laser-assisted targeting
This approach employs nonsurgical lasers that emit a beam from the fluoroscopic C-arm system. This beam targets the puncture site. The urologist then aligns the needle with the beam to gain percutaneous access.
Two such novel laser applications have been proposed to reduce radiation and time needed to perform renal collecting system puncture for PCNL. 30,31 Although both the direct alignment radiation reduction technique (DARRT) and surgical approach visualization and navigation (SAVN) system rely on the bull's eye principle, the main difference is that with DARRT, the laser always emits straight down from the center of the fluoroscopy (Fig. 4). 30 With SAVN, the direction of the laser beam is adjusted after data processing from an initially acquired fluoroscopy image on which the target could be selected with a cursor. 31 Both the DARRT and SAVN technique were able to significantly reduce fluoroscopy time during renal puncture, however, only with SAVN could the total puncture time and number of attempts be reduced as well. 30,31

Laser-assisted targeting: DARRT. DARRT = direct alignment radiation reduction technique.
EMT-based innovations
The previously mentioned approaches use 2D images to map puncture tracts and do not provide real-time 3D information. This reduces the precision of the generated route and does not account for patient respiratory movements that often must be arrested. Electromagnetic system-based innovations solve these limitations. This approach has been tested on porcine models, 32,33 and more recently in a human subject proof-of-concept study in 2017. 34
Real-time 3D tracking
An electromagnetic field is generated and establishes a tracking volume in the operating room. The surgeon then places a ureteral catheter with an Aurora EMT system sensor (Northern Digital, Inc., Waterloo, Ontario, Canada) (Fig. 5) at its tip in the desired puncture site through ureteroscopy. Software gathers and processes information on the orientation of the catheter and relays it to a monitor. The selected calix is then punctured using a needle with an electromagnetic sensor on its tip, allowing the surgeon to visualize the needle in relation to the catheter detected by the EMT sensor system. The access is thus guided in real-time by images observed on the monitor and can be combined with various software that can generate trajectories and audio support, such as an increasing pinging sound when the needle tip is close to the tip of the catheter. 32 –34

Electromagnetic guidance systems: Aurora EMT (left) and custom ultrasound+electromagnetic guidance setup (right). EMT = electromagnetic tracking. This image was taken from the following article published in European Urology (with permission to use provided by one of the authors):
Lima et al. reported that all 10 punctures performed on patients were successfully completed at the first attempt without X-ray exposure that could be used to place the catheter; instead, the surgeons relied on the endoscopic view as well as US. The median time to successful puncture starting from insertion of the needle was 20 seconds. 34 In a series of 12 patients reported in 2018 by the same group, the median time to successful puncture starting from insertion of the needle was similar at 22 seconds and access was achieved at the first attempt without any X-ray exposure. 35
Limitations of EMT-based innovations
This approach was performed in a highly selected population and requires further experimentation, such as in obese patients (potentially reducing the precision of the EMT) and patients with large stone burden (making the catheter placement more difficult). This technique also requires the endoscopic placement of a catheter to mark the puncture site of interest, further lengthening the procedure.
CT-based innovations
The use of CT for preoperative imaging and access site planning is commonly used in PCNL. On the other hand, it is quite rare to use it to gain access to the kidney during the procedure, as it delivers much higher doses of radiation to the patient as compared with fluoroscopy. Innovations in cone beam CT technology attempt to deliver 3D imaging suitable for the management of complex cases while minimizing delivered doses of ionizing radiation.
Cone beam CT
The cone beam CT, commercially known as the Uro Dyna-CT (Siemens, Munich, Germany), works on the principle of simultaneously projecting both length, width, and depth information to the imaging detector while a gantry rotates around the patient. A traditional CT is limited to a single transverse slice per rotation and thus needs multiple rotations to get volumetric imaging. Compared with traditional CT, the simultaneous imaging of multiple depth levels in Uro Dyna-CT allows for volume acquisition with a single gantry rotation—thus greatly minimizing the amount of radiation delivered with only a slight compromise to image quality. 36
Needle guidance
Uro Dyna-CT imaging can be used in conjunction with the Syngo iGuide (Siemens), a needle guidance technology. It provides real-time path, position, length, and angulation information to enhance needle guidance during PCNL. Ritter and coworkers have explored the use of Uro Dyna-CT with Syngo iGuide on 27 patients. 37 With a median radiation dose of 6113.1 micrograys meters squared (μGym 2 , range 1081.6–7957 μGym 2 ), they achieved an 88% PCNL access rate with 24 of the 27 punctures being successful. Comparatively, the median fluoroscopy dose is of 96.9 μGym 2 (range 13.4–840.8 μGym 2 ).
Limitations to CT-based innovations
Despite innovations in CT dose reduction, the much higher doses and cost of the Uro-Dyna CT compared with fluoroscopy limits its use in the management of complex cases.
Combination of imaging modalities-based innovations
Certain PCNL access innovations combine multiple imaging modalities.
Preoperative MRI, intraoperative US and optical tracking guidance
For PCNL access, Zhang and associates explored the possibility of using preoperative MRI and fusing the image with intraoperative US slices. This fusion generates an image that is used by the surgeon to guide the robot to the insertion point. Once the needle is aligned, the robot autonomously performs the puncture in accordance with the surgical planning. The US probes and needle end are marked with reflective material such that the position of the instruments can be optically tracked by a third device relaying the information to the US screen. Kidney deformation due to breathing are accounted for and minimized, thanks to a gating method. In human trials, the root mean square target registration error was 3.53 mm (the procedure was not performed). On phantoms, adequate percutaneous puncture was obtained, on average, in 266 seconds by urologists. 38,39 In a more recent work, the same group added robotics to their technique. 40 Robot-assisted needle insertion can facilitate percutaneous procedures by increasing accuracy and consistency; in the above case, the setup demonstrated improved precision and shortened duration. However, an important limitation of this technique is the incorrect needle positioning information caused by the bending of the needle shaft when entering soft tissue.
US and electromagnetic guidance
Chau and associates trialed a magnet-based tracking system for US-guided kidney punctures, where the US probe, as well as the needle, is fitted with a magnet. When used in a magnetic field, the estimated needle trajectory can be visualized by the US probe. In a preliminary clinical study, they demonstrated that needle puncture was successful in 100% of times, with only 3 out of 18 cases needing two puncture attempts. 41 In a similar combination of US and electromagnetic guidance, Ungi and colleagues used tracked US snapshot guidance together with an electromagnetic field to coordinate the US and the needle relative to the kidney model to increase the success rate of US-guided renal access (Fig. 5). 42 With the use of this additional hardware and software, the number of attempts, as well as needle insertion time, was significantly reduced. The authors reported that an additional cost of 10,000$ for hardware would be necessary to upgrade an existing US machine and that the software needle for calibration, synchronization, and image processing was freely available at the time of the project.
Real-time virtual sonography: US, electromagnetic, and CT guidance
Hamamoto et al. used the HI VISION Ascendus (Hitachi-Aloka Medical Ltd., Tokyo, Japan). It consists of the main US unit, magnetic location detector unit, magnetic field generator, and magnetic sensor. The magnetic sensor, attached to the US probe, captures the location, direction, and rotation of the US transducer within the magnetic field, instantaneously transferring this information to the main unit for cross-sectional, multiplane image reconstruction. Real-time virtual sonography (RVS) achieves this by combining real-time US with preoperative CT volume data and displaying them side by side on the same monitor. In 30 consecutive patients divided into two groups, RVS-guided renal puncture was effective and reported a lower incidence of bleeding-related complications compared with conventional US percutaneous access. 43
Nonimaging-based innovations
Innovations not relying on imaging are developed to facilitate steady needle positioning and insertion.
Needle support
Although mainly studied with fluoroscopy, needle trestles/support can be used in virtually any manual approach as it holds the needle in place and allows for precise readjustment.
As an example, Chowdhury et al. developed a rudimentary, cheap, and portable mini access guide (MAG). 44 The MAG consisted of a radiolucent cylinder with two aligned tubes for maneuvering the puncture needle. Using fluoroscopy and the bullseye technique, the apparatus reduces fluoroscopy screening time from 39 to 21 seconds, puncture time from 80 to 55 seconds, and aids novice residents when learning the puncture technique. Given the improved speed and accuracy of the MAG, this technique shows potential in reducing direct radiation exposure to the surgeon's hands. A similar tool applying the exact same principles, the “Locator” was developed by Lazarus and Williams and consisted of two articulated arms with two spherical joints that held the needle in place (Fig. 6). 45

Needle support systems: MAG (left) and The Locator (right). MAG = mini access guide.
Needle drivers
Needle drivers both support the needle while also advancing the needle following alignment by the urologist. An example of such a robot is the percutaneous access to the kidney with remote center of motion device (PAKY-RCM), a radiolucent, sterilizable needle driver developed at Johns Hopkins (Fig. 7). Mounted on the end of a robot arm, PAKY-RCM grasps, stabilizes, and advances a puncture needle into the kidney. When comparing standard manual access with fluoroscopy, the number of attempts and the amount of time needed to percutaneously access the kidney were comparable to those of standard manual techniques. Again, similarly to the MAG, direct radiation exposure to the surgeon's hands is reduced. 46 More importantly, this device has implications for automation down the road—it would serve as the arm of such a device.

Robotic surgery and virtual reality: PAKY-RCM (left) and iPad-guided PCNL (right). PAKY-RCM = percutaneous access to the kidney with remote center of motion device; PCNL = percutaneous nephrolithotomy.
Limitations of needle drivers
In urology, the PAKY-RCM alone has only seen very limited adoption since its invention 20 years ago. Its puncture time and the number of attempts required to obtain access have not managed to outperform the surgeon.
Virtual reality and augmented reality
Augmented reality and imaging coregistration
Rassweiler et al. present a novel way of utilizing augmented reality to assist the surgeon in performing PCNL punctures. 47,48 By aligning an iPad above the patient and coregistering the view of its camera with the view of the Uro Dyna-CT, Rassweiler et al. project virtual anatomical structures of the kidney on the patient to facilitate PCNL access (Fig. 7). Practicing on kidney phantoms, the augmented reality overlay technique improves puncture time from 81 to 65 seconds for trainees but increases puncture time from 58 to 82 seconds for experienced urologists. Radiation exposure was reduced in both groups by a factor of 3 for the trainees (7.8–2.6 μGym 2 ) and by a factor of 1.8 for the urologists (6.9–3.9 μGym 2 ). This technique is limited by the lack of depth information provided by a tablet camera and shows substantially higher puncture time among experienced urologists. However, the reduced radiation and improved puncture time among trainees demonstrates its potential as a teaching tool.
Discussion
In this review, we comprehensively identified technologies that can be used during the procedure to enhance the ability of urologists to obtain their own PCNL access. Despite most studies reporting preliminary data, there is no doubt that these innovations can facilitate PCNL access, as highlighted by the reduced puncture times and high success rates. We hypothesize that superior tract access may result in lower access-related complications, although more robust data are needed.
The next step is to evaluate the clinical outcomes and value of these devices. For example, their impact on complications and stone-free rates must be weighed against their cost. Additionally, as most innovations have only been tested by their creators, independent evaluation of the devices by new groups is warranted. Only after further reporting can we expect more widespread adoption of these technologies.
For tools used as adjuncts to existing techniques, such as laser targeting for fluoroscopy and trajectory projection in US, there is also potential for significant educational value. Trainees and novices might benefit from these tools, additionally to existing ones for surgical planning (which are outside of the scope of the current review), when learning how to obtain their own access.
There are also significant implications for automation of obtaining the access itself, with ANT-X being one of the first to do so. With advances in both hardware and software as well as significant improvement in the ability to image the kidney and stones, it can be expected that other automated puncture devices might surface in the next few years.
Considering the movement toward reducing radiation exposure in PCNL, US-based assistive innovations yield the most potential as they address an important barrier to the widespread adoption of this radiation-free approach: puncture tract visualization. In terms of value, these add-ons are possibly less costly than other alternatives such as EMT-based devices. Although they also nullify radiation exposure, EMT-based innovations might pose challenges with regard to cost and convenience. While automation is promising and possibly practice changing, current outcomes when compared with manual approaches might not be convincing enough when considering value. The combination of existing technologies and approaches should also be considered.
Conclusion
In the era of advancing technology and increasing precision in the field of surgery, PCNL access must yield to this reality. Fortunately, a tremendous amount of progress has been accomplished to obtain the perfect PCNL access. From imaging-based assistive innovations to EMT, many different technologies have been developed and tested to perfect PCNL access. Currently, these innovations are still in an experimental phase and further research is needed to demonstrate their added value in a clinical setting. With the current movement of lowering or eliminating radiation, it is likely that the US assistive innovations will be the most clinically relevant adjuncts to PCNL access.
Footnotes
Author Disclosure Statement
No competing financial interests exist.