
Abstract
Purpose:
Palliative transurethral resection of the prostate (pTURP) in metastatic prostate cancer (mPCa) is reported to be rarely applied in clinics. We prospectively evaluated the ability of pTURP to achieve tumor control in patients with mPCa.
Patients and Methods:
A prospective study of patients with mPCa from 2011 to 2018 was conducted. The patients were divided into two groups: a pTURP + androgen deprivation therapy (ADT) group and an ADT group. Castration-resistant prostate cancer (CRPC)-free survival and cancer-specific survival (CSS) were analyzed as research endpoints between the groups using a Kaplan–Meier estimator.
Results:
A total of 188 patients with mPCa were enrolled in the study from our center, of which 110 patients were in the pTURP + ADT group, and 78 patients were in the ADT group. The basic clinical characteristics were comparable between the groups. There were no reoperations or severe complications in the pTURP + ADT group. The median follow-up was 29 months. The median CRPC-free survival was significantly increased when the 7-month prostate-specific antigen (PSA) was <4 ng/mL (34 vs 6, p < 0.01) and bone metastasis was ≤5 (25 vs 10, p < 0.01) but not in the pTURP + ADT group (16 vs 12, p = 0.267). The 3-year CSS was higher in the pTURP + ADT group than that in the ADT group (95.9% vs 64.9%, p = 0.004), as well as when the 7-month PSA was <4 ng/mL compared to ≥4 ng/mL (90.7% vs 36.6%, p < 0.01) and when bone metastasis was ≤5 compared to >5 (82.2% vs 63.2%, p < 0.01). In subgroup analysis, pTURP + ADT could significantly improve patients' CSS when PSA ≥65 ng/mL, Gleason Score (GS) ≥8, and bone metastasis ≤5.
Conclusions:
We used our center-based cancer database to analyze survival in patients with mPCa undergoing pTURP. In the study population, pTURP + ADT was indicated to benefit CSS and shown to be safe. Moreover, we suggest that mPCa patients with PSA ≥65 ng/mL, GS ≥8, and bone metastasis ≤5 may perform pTURP before ADT.
Introduction
Prostate cancer (PCa) is the most commonly diagnosed solid malignancy and the second leading cause of cancer-related death in males in the United States. 1 Due to the cost of the prostate-specific antigen (PSA) test and the poverty rate in China, more than 65% of patients are diagnosed with metastatic PCa (mPCa) at the time that they first visit a doctor, leading to poor prognosis. 2,3 According to the EAU guidelines, androgen deprivation therapy (ADT) is the standard treatment for patients with mPCa. 4
Due to the aggressiveness of cancer cells, bladder outlet obstruction (BOO) and hematuria are usually presented as important clinical manifestations in patients with mPCa. Palliative transurethral resection of the prostate (pTURP) has been proved to be effective for relieving BOO based on short-term clinical outcomes in recent years. 5 However, the use of pTURP to prolong survival is controversial due to a lack of sufficient evidence. 6 As a form of cytoreductive surgery, pTURP is theoretically believed to lower the tumor burden of local lesions, which might result in a better prognosis.
In this study, we present a prospective study comparing the short-term oncologic outcomes in patients receiving a combination therapy of pTURP and ADT with those in patients receiving ADT alone. To our knowledge, this is the largest prospective study in this research field.
Patients and Methods
Data of patients with mPCa who were treated in our center were prospectively collected from July 2011 to June 2018 in this study. We treated part of the patients with pTURP due to the indications of BOO or hematuria before ADT (pTURP + ADT group, bicalutamide was taken the day after pTURP, and Leuprorelin was injected 2 weeks later to avoid flare up), and the others received ADT alone (ADT group). pTURP was performed by an experienced doctor. A bipolar electrode system was used and the procedure was as the same as TURP for benign prostate hyperplasia to relieve BOO.
The inclusion criteria for all the patients were as follows: (1) newly diagnosed PCa with more than two bone metastasis (positive on bone scan or MRI, and confirmed by CT three-dimensional reconstruction) at the time of diagnosis; (2) asymptomatic of bone lesions, but with BOO or severe hematuria; (3) no visceral metastasis; and (4) no prior radiation of bone lesions and systemic therapy for PCa. All four criteria should be met at the same time for inclusion.
Follow-up in both groups was composed of regular visits (every 1–3-month) with PSA testing and clinical examination. Further radiologic assessments, including pelvic MR or bone scan were performed when necessary (rising PSA, symptomatic patients, doctor's discretion). Docetaxel was chosen as the second-line treatment for patients with castration-resistant prostate cancer (CRPC) before abiraterone or enzalutamide.
The first research end point was the occurrence of CRPC, which was defined as CRPC-free survival. CRPC was defined as follows: (1) testosterone <50 ng/dL and (2) biochemical progression (three consecutive rises in PSA 1 week apart resulting in two 50% increases over the nadir, and a PSA >2 ng/mL) or radiologic progression (the appearance of new lesions: either two or more new bone lesions on bone scan or a soft tissue lesion) according to guidelines. 4 And the second research end point was the occurrence of death due to PCa, defined as cancer-specific survival (CSS).
Continuous variables were presented as the median with interquartile range. Clinical baseline data were compared by t test and chi-square test. Standard survival-analysis methods were used to analyze time-to-event data (time to CRPC, and time to cancer-specific death) with Kaplan–Meier estimates for survival curves and Cox proportional-hazards models to estimate relative risk factors, including age, PSA at diagnosis, Gleason score, number of bone metastases, pTURP, and subsequent treatment. SPSS 22.0 for Windows (SPSS, Inc., Chicago, IL) was used for all statistical calculations and analyses. Statistical significance was considered as a p value less than 0.05.
Results
A total of 188 patients with mPCa were treated in our center. Among them, 110 patients underwent pTURP before ADT, which was defined as the pTURP + ADT group, and 78 patients underwent ADT alone and were classified as the ADT group. The patients' clinical and operative characteristics are shown in Table 1. All the characteristics were comparable between the groups, including age, BMI, median PSA, PSA level ≥65 ng/mL percentage, Gleason Score ≥8 percentage, and bone metastasis ≥5 percentage (p > 0.05). In the pTURP + ADT group, the mean operative time was 38.87 ± 16.11 minutes, the resection volume was 42.24 ± 7.15 g, and the hospital stay was 5.29 ± 0.75 days. There were no reoperations or other complications such as hematuria, urethrostenosis, and urinary incontinence.
Patients' Clinical and Operational Characteristics
ADT = androgen deprivation therapy; BMI = body mass index; GS = Gleason Score; IQR = interquartile range; PSA = prostate-specific antigen; pTURP = palliative transurethral resection of the prostate; SD = standard deviation.
At a median follow-up of 29 months (Table 2), the median CRPC-free survival was 16 and 12 months in the pTURP + ADT and ADT groups, respectively, with no significant difference (p = 0.267). However, the 3-year CSS showed a significant difference between the pTURP + ADT and ADT groups (95.9% vs 64.9%, respectively, p = 0.004) (Fig. 1). In multivariate Cox-regression analysis, pTURP + ADT was also associated with better CSS (hazard ratio = 0.374, p < 0.05) when including other factors such as age, PSA at diagnosis, Gleason score, bone metastasis number, and subsequent treatment (Table 3).

Patients' Follow-Up Information
CRPC = castration-resistant prostate cancer.
Multivariable Survival Analysis
Age: ≥70 vs <70.
PSA at diagnosis: ≥65 vs <65.
Gleason score: ≥8 vs <8.
Bone metastasis: >5 vs ≤5.
HR = hazard ratio.
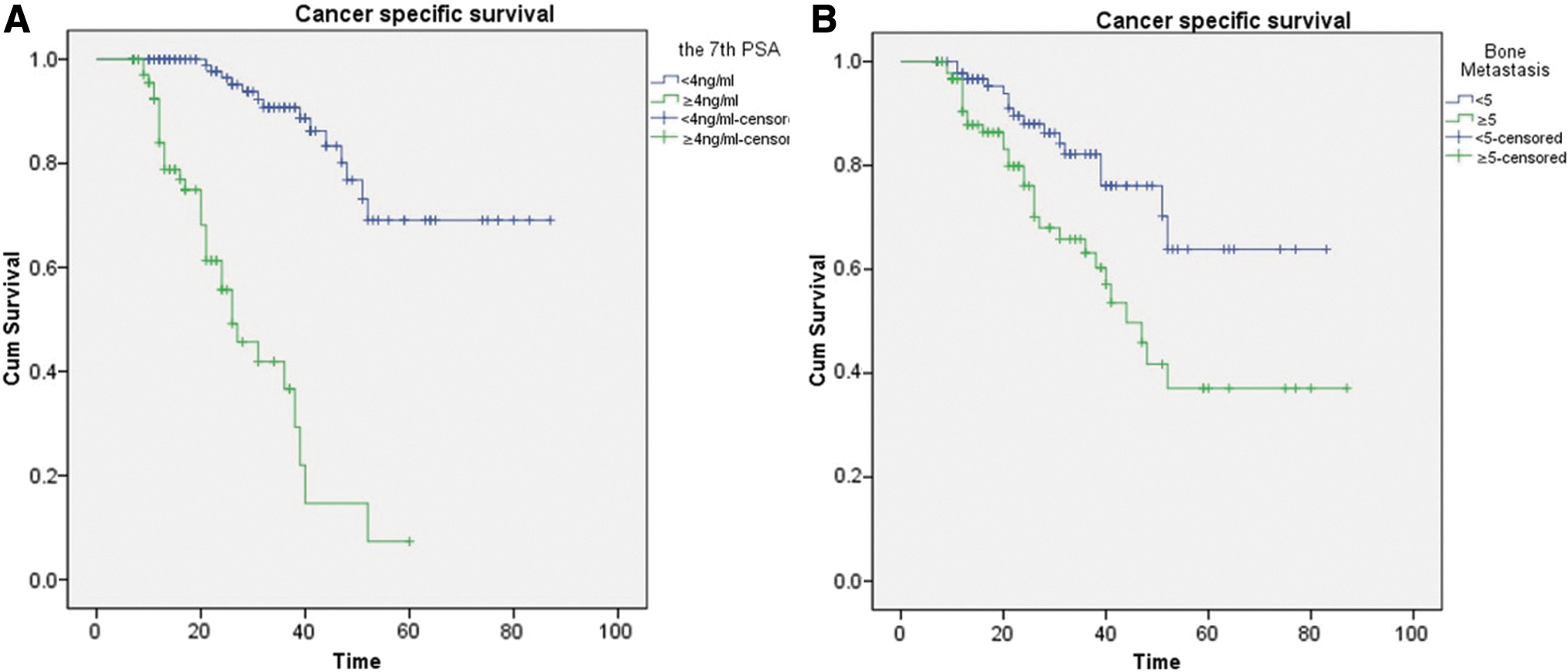
According to the EAU guidelines, the 7-month PSA level has great importance in predicting patients' prognosis. 4 We divided the 7-month PSA after ADT into two levels: <4 and ≥4 ng/mL. The median CRPC-free survival was significantly improved by 28 months (34 vs 6, p < 0.01) when the 7-month PSA was <4 ng/mL compared with ≥4 ng/mL. The 3-year CSS was 90.7% and 36.6% when the 7-month PSA was <4 and ≥4 ng/mL, respectively, with a significant difference (p < 0.01) (Fig. 2A). Furthermore, bone metastasis was reported to affect the prognosis when it was classified as ≤5 and >5 according to the guidelines. 4 The median CRPC-free survival was significantly improved when bone metastasis was ≤5 compared to when it was >5 (25 vs 10, p < 0.01). Meanwhile, the 3-year CSS also exhibited benefits between the two groups (82.2% vs 63.2, p < 0.01) (Fig. 2B).
Finally, we would like to analyze how pTURP affected survival in different subgroups. Results showed that pTURP + ADT could significantly improve patients' CSS in the subgroup of PSA >65 ng/mL (p = 0.011), Gleason Score (GS) ≥8 (p = 0.01), and bone metastasis ≤5 (p = 0.023) (Fig. 3).

CSS stratified by pTURP in subgroup of
Discussion
Prostate cancer is the most frequently diagnosed cancer in males in western countries. In China, the incidence is gradually increasing in some regions, such as Shanghai and Hong Kong. 3 However, due to the poverty rate in China, most patients who present with hematuria and lower urinary tract obstruction are diagnosed with PCa in the late stage at the time they first visit a doctor. It has been reported that the mortality-to-incidence rate ratio (MR/IR) in China is 0.63, which is significantly higher than that in North America (MR/IR = 0.13), where the incidence of PCa is high. 7 Thus, the problem we face in China is how to diagnose and treat such a large amount of mPCa patients with a poor prognosis.
Primary ADT has been the standard treatment for mPCa for over 50 years. 8 Combination therapy, including ADT and other agents such as abiraterone acetate or docetaxel, has been proved to be of benefit in overall survival (OS) when compared with ADT alone, 9 –11 indicating that combination therapy is promising in the future. The treatment of primary tumors in newly diagnosed metastatic disease is another kind of combination therapy based on ADT, but it is controversial. Such interventions are still considered experimental due to a lack of evidence. 12 It is thought that local treatment of mPCa cannot be beneficial because mPCa has the properties of a systemic disease, in which tumor cells have already spread into other organs such as lymph nodes, bones and abdominal viscera through the circulation. In HORRAD and STAMPEDE trail, there were no OS benefits with the addition of radiotherapy (RT) to ADT for men with mPCa. Interestingly, the OS was significantly improved when patients split into subgroups of high burden and low burden. 13,14
Besides radiotherapy, several studies have demonstrated that reducing the tumor burden leads to a survival benefit and a better response to systemic therapy. A large population study using the Surveillance Epidemiology and End Results (SEER) database revealed that local treatment of the prostate, including radical prostatectomy (RP) and brachytherapy, in men diagnosed with mPCa had a survival benefit. 15 Data from the Munich Cancer Registry were used to reproduce the study, to include 1538 patients who were newly diagnosed with mPCa. The results showed a significant survival benefit for patients who received RP as a local treatment. 16 Furthermore, another study was carried out by professor Löppenberg and his colleagues, focusing on the application of local treatment to improve the survival rate by using propensity score matching. 17 Moreover, Bianchini and his colleagues 18 investigated the locoregional treatment, including radiotherapy and transurethral prostatectomy, in patients with mPCa in a single institution. The results showed that locoregional treatment can significantly increase patients' OS. However, the majority of these studies were retrospective, which lack strong evidence, although several prospective and randomized studies are being in progress currently. 19,20 Another limitation was that RP and RT usually results in adverse complications, such as urinary incontinence and erectile dysfunction.
pTURP was proved to be safe and effective in relieving bladder outlet obstruction, helping patients with late stage PCa have better voiding. 5,21,22 As a kind of cytoreductive surgery, the oncologic outcomes of pTURP in advanced PCa are thought to be controversial. A previous retrospective study compared 39 patients who received pTURP + ADT with 107 patients who received ADT alone. 3 The results showed that patients in the combination therapy group had a significantly better response to ADT and had a trend toward longer CSS. Recently, another research evaluated the survival difference between pTURP + ADT and ADT groups using propensity score matching. 23 Although the surgery is safe enough, the results revealed a worse CRPC-free survival, CSS, and OS in the pTURP + ADT group, indicating that pTURP should be seriously considered for application.
In our study, pTURP was proved to be safe as an approach to reduce lower urinary tract obstruction and hematuria without any complications. More importantly, it could significantly improve 3-year CSS by 30% when comparing with ADT alone. And another interesting point was that pTURP could increase the survival rate with statistical significance when PSA >65 ng/mL, GS >8, and bone metastasis ≤5. The results indicated that pTURP had advantage in patients with worsened local conditions and lower metastatic bone lesions, which help us in the selection of patients. A controversial result is that patients in combination group had improved CSS, but with the same CRPC-free survival can be explained that time to CRPC is not an important prognostic factor in predicting OS. CRPC was seldom mentioned in other large studies in treating mPCa by combination therapies. 24,25
Mechanisms underlying the survival benefit of a cytoreductive treatment remain unknown. We speculate that the possible reasons include decreasing the burden of tumor tissue, removing tumor-promoting factors and immunosuppressive cytokines, facilitating the combination of androgen blocker with the receptor in tumor cells, and reducing the possibility of metastasis from the primary site to other sites. 15 In the group of pTURP + ADT, 44.3% patients received other treatments although without significance, which was thought to be another important reason. We think that patients in the combination therapy group were more willing to actively cooperate with doctors to receive further treatment, such as chemotherapy and abiraterone, which helps increase the survival.
The main limitation of the study is short follow-up period in both groups. Compared to 44 months as the median survival for patients with mPCa, most patients of the study did not reach the research end point that influences our results. Nevertheless, we analyzed the existing data and discovered a trend with statistical significance.
Conclusion
To our knowledge, this is the first prospective study investigating the combination of pTURP and ADT in patients with mPCa. We found that patients who underwent pTURP and ADT had survival advantages compared with those who underwent ADT alone. As a kind of cytoreductive surgery, pTURP might have the function of reducing the tumor burden and therefore lower the possibility of disease progression. We suggest that mPCa patients with PSA ≥65 ng/mL, GS >8, and bone metastasis ≤5 may perform pTURP before ADT.
Footnotes
Author Disclosure Statement
No competing financial interests exist.