
Abstract
Purpose:
Our objective was to seek correlations between the type, volume, and duration of surgical work performed, surgeon habits and characteristics, and the prevalence of neck and back musculoskeletal complaint and intervention across career from training to retirement.
Materials and Methods:
An anonymous web-based multinational survey of urologists was conducted. The primary outcome measured was pain. Secondary outcomes included pain requiring intervention and surgery. Responses were subgrouped according to geography, practice patterns, and demographics. Student t test, Fisher's exact test, and chi-square test were used for analysis.
Results:
A total of 701 complete responses were received from this multinational survey. Gender, pain distribution, and private or academic practice did not correlate with pain, whereas exercise, lower weight, and body mass index (BMI) were protective. Dose–response of surgical type was assessed with high- and low-volume density quartiles and frequency of each pain severity; no correlation was found. Secondary analysis showed that female practitioners seek invasive therapy less than male counterparts, and practitioners of direct optical cystoscopy report no more neck trouble than others. Length of career since residency shows little relationship to pain or pain-free rates.
Conclusions:
In this, the largest surgical ergonomic study to date: surgical type, duration, volume, setting, and physician gender were unrelated to surgeon pain throughout career. Exercise was associated with lower prevalence of pain in a dose-related manner; increasing weight and BMI were positively associated with pain. Although 47% of urologists with spinal pain blame their career, we are unable to identify any dose–response relationship that supports that assumption.
Introduction
Workplace sickness and injury have been recognized as a risk of modern life for centuries, and received focus at least as long ago as the British Factory Act of 1802. Highly repetitive, unnatural or heavily loaded movements have been shown to result in a variety of injuries in dentistry, computer usage, mining, cytotechnology, and many forms of surgery. Just to name a few. 1 –5 Of late, great attention has been called to the discomfort that many surgeons experience in the course of their job, and great effort has been made to study it. The rapidly growing field of ergonomics has risen to the challenge, and sets of recommendations now exist to guide surgeons and optimize the operating room for minimization of discomfort and presumably injury, although to date these are generally poorly implemented. 6
The act of performing surgery is by nature a highly focused undertaking, and it is common that a surgeon may find himself/herself in a static position for a long period of time during an operation, and subsequently uncomfortable. The advent of laparoscopic surgery has been felt to add further stress to posture, adding necessity of looking at a monitor that may or may not be in a good location while extending one's arms in often-awkward directions. Hours a day in orthopedically unfavorable positions, from the sustained downward gaze of open surgery with the head far off-axis of the spine to the imbalanced and often poorly leveraged movements of laparoscopy have been shown to induce discomfort, and higher volume surgeons are possibly subject to more discomfort. 7 –9 Evidencing concern for injury that repetitive down-gaze could cause, and presumably motivated by neck pain from the earliest days of the microscope, Sir David Brewster stated in 1835 “the best position for microscopical observation is when the observer is lying horizontally on his back …” 5,10
Paradoxically, physical exercise is viewed as beneficial on an essentially universal level, and is linked to every possible form of benefit: cardiovascular health, improved cancer-specific outcomes, better erectile function, greater happiness, and decreased pain. 11 –15 Lack of exercise is directly associated with a wide spectrum of chronic disease. 16 Relevantly, exercise is recommended as an effective and cost-effective therapy for back pain. 17,18
Where then does the boundary between beneficial physical stress (exercise) and harmful physical stress as implicated in workplace injury lie? Certainly, many people of all walks of life report exercise as somewhat undesirable and/or uncomfortable, yet the overwhelming bulk of evidence presents it as beneficial. Further contaminating this soup is the significant background noise provided by the roughly 20% incidence of back pain faced by humanity, as well as near-universal neck pain and age-related physical deterioration. 19 The example of carpal tunnel syndrome may serve as a signpost for damaging overuse in extreme conditions where frequency, force, and day-long repetitiveness of some motions do appear to result in orthopedic injury requiring intervention. 20
Surgeons, workers, and people in general will modify their day to minimize discomfort as possible, and there likely exists individual bias in career selection that may reflect differing experiences of physical distress, and result in significant self-selection for career. We have undertaken to identify a dose–response curve of not only pain but also verifiable and objective damage that goes beyond the perception of discomfort: the incidence of intervention on the axial skeleton. This requires the opinion and participation of a specialist in spinal pathology, and can be used to represent the true coalescence of pain, a subjective perception, with objective and actionable physical damage in the opinion of the reviewing specialist.
We surveyed urologists to seek correlations between the type, volume, and duration of surgical work performed, surgeon physical characteristics, and the prevalence of musculoskeletal complaints across the span of careers from training into retirement. Musculoskeletal discomfort was divided into subjective experience of pain, which is common with many if not most jobs, and also into the categories of those seeking noninvasive treatment for their pain, and finally those who underwent invasive therapy for spinal problems.
Lifestyle factors such as presence, type, and frequency of athletic activity were assessed for their contributory or protective effect on the endpoints of subjective pain. Finally, a worldwide cohort was assessed, to aggregate different practice patterns, lifestyles, and allow the expression of other lifestyle factors.
Urologists are especially well suited to this study in that we were able to recruit a significant response volume from open surgeons, laparoscopic surgeons, robotic surgeons, and microsurgeons as well as endoscopists (both video and direct optical), to assess for differences in these practice types. A uniquely large and worldwide response was achieved, allowing control for locality of practice and assessment of local factors.
No prior surgical studies, to our knowledge, has worked to begin to identify lifestyle or protective effects for spinal complaints. Similarly, we are aware of no controlled study designed to eliminate baseline complaints as widely experienced by humankind. We set out to factor out the contribution of different surgical types, age, volume and locality, as well as to identify other factors in the nonwork life of these practitioners that may be protective.
Materials and Methods
An anonymous web-based multinational survey of urologists was designed with pain as the primary outcome (see Supplementary Appendix S1). A 14-question survey was distributed through a variety of society mailing lists after gaining approval from the relevant managing bodies. Trainees were included when encountered. Responses were voluntary with a single reminder sent. Results were collected for a period of 2 months. The University of Colorado-maintained Qualtrics (Provo, UT) system was used; data management was performed on the native software and downloaded to spreadsheets. Survey data were collected in anonymized format and software was configured to prevent multiple submissions from any single IP address. When available, the percentage of sent emails that were opened/seen by recipient was reported for use in calculating response rates.
Goals were to quantify the type of urologic surgery: robotic, laparoscopic, microscopic, open, and endoscopic (Fig. 1). These results, as well as the surgeon characteristics of length of surgical career (surgical dose), worldwide locality, basic physical characteristics (gender, height, weight, body mass index [BMI]), and exercise (amount and type) were then crossed against three categories of neck and back problems: pain, need for noninvasive therapy (physical therapy, massage, and acupuncture), and need for invasive therapy (injection or surgery). Finally, practitioner self-assessment as to whether complaints were felt to be the consequence of their surgical career was sought.
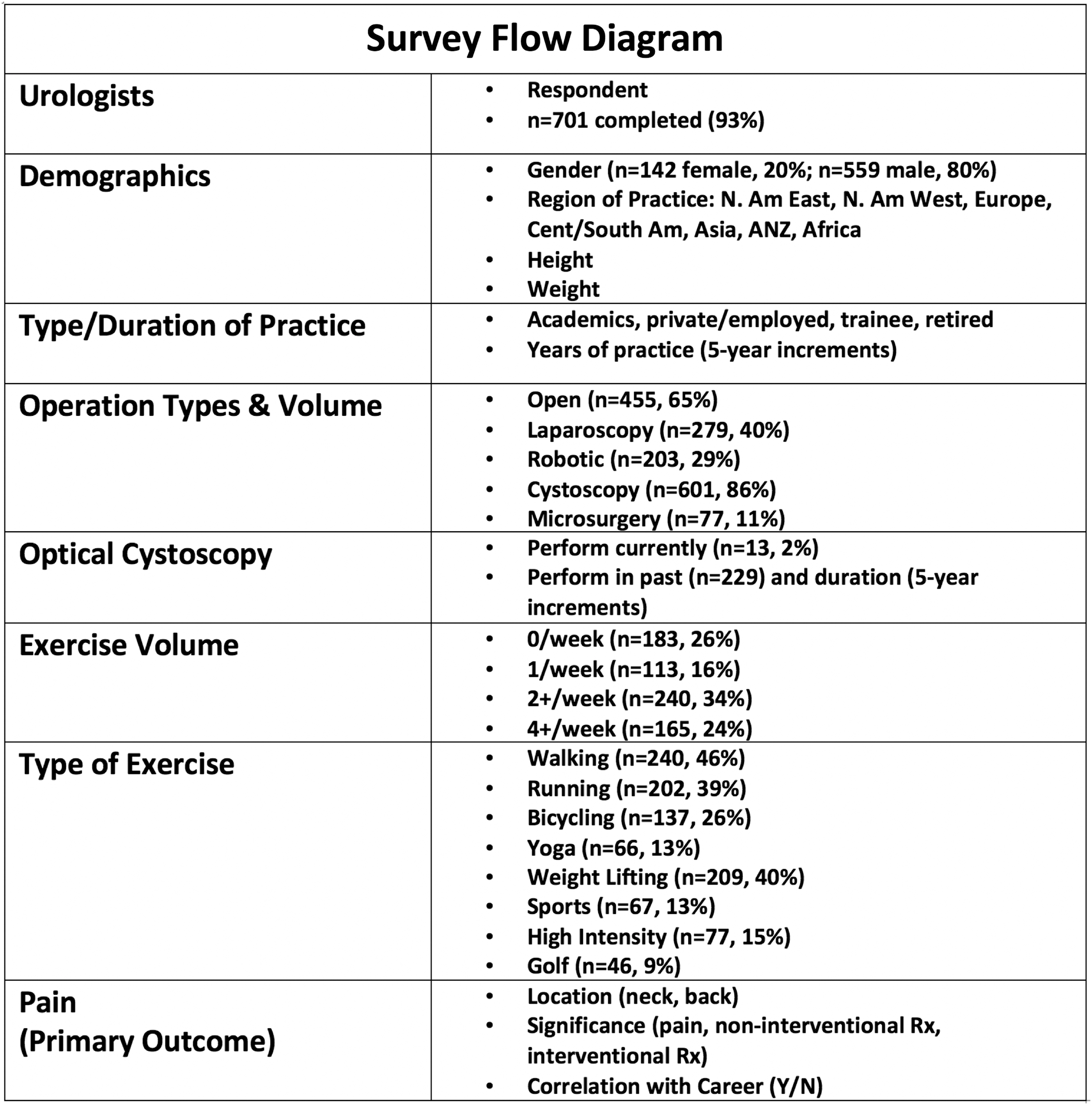
Survey flow diagram.
Statistical comparisons were made for comparing predisposing factors for pain, using chi-square testing. Statistical significance was set at p < 0.05. Comparisons of continuous variables such as height, weight, and BMI were made with Student t tests. Secondary outcomes such as pain-seeking noninvasive treatment and pain requiring invasive treatment (surrogate of severity) were made against the “no pain” group using identical statistical methods (Table 1).
Respondents Reporting Presence or Absence of Pain, Pain Requiring Noninvasive Treatment Such as Massage, or Invasive Treatment Such as Injection or Surgery Compared with Exercise, Body Mass Index Components, Gender, and Practice Setting
Denotes p < 0.05.
BMI = body mass index; SD = standard deviation.
To separate certain procedure types as independently etiologic for pain, current procedure type volumes were divided into quartiles based on weekly surgeon estimate. The low- and high-volume quartiles are displayed side by side for comparison in Figure 2, estimating the direct effect of significant volume of any certain procedure type.

High- vs low-volume quartiles of practice by reported weekly volume within each urologic surgical domain.
Results
Responses were received from 764 worldwide respondents. After excluding nonsurgeons and incomplete surveys, we analyzed 701 responses, with a completion rate of 93%. Outline and survey design flow are outlined in Figure 1.
Efforts were undertaken to control for survey invitations that were sent to inactive email addresses, spam boxes, or otherwise were never reviewed by the intended recipient. The majority of our sent emails were managed through societies that were able to track data on whether or not the email itself was opened. This revealed an average opening rate of 31.3% (3776 sent/1208 opened). This rate was applied to the minority of sent emails without opening rate data (3372), yielding a calculated opened number of 1055. After exclusion of incomplete surveys, total calculated response rate for completed surveys was 701/2263 = 30.9%.
Overall, the incidence of spinal pain was 45% (n = 213), including 24% incidence of neck pain and 35% back pain (with overlap). Complaints of back and neck pain were stable across the different types of urologic surgery, including when only the highest volume of respondents was analyzed. Groups representing “high-volume” and “low-volume” surgeons were created that subtended the highest and lowest quartile of reported activity for each type of surgery and analyzed; no differences were seen in reported pain between high- and low-volume surgeons within any surgical type or across different types (Fig. 2).
Physical characteristics of the surgeons appeared to be mildly related to complaints, especially of back pain, with an increase in complaints of pain correlating with BMI (Table 1).
Exercise appeared to have a dose-related protective effect. Respondents who exercised more than two times per week and those who report exercise at more than four times per week (p < 0.05) showed progressive diminution in likelihood of complaining of pain.
Globally, the incidence of spinal pain was lower in North America than the rest of the world, with 247/417 (59.2%) of North American respondents reporting no significant pain vs 146/284 (51.4%) in the rest of the world, although this finding did not achieve statistical significance.
Complaints of pain were static across all cumulative doses of surgery and aging—from trainees and those in early career, through midcareer, and into retirement (Fig. 3). Contrary to other reports, we found no difference in the rate of pain as a complaint in female surgeons, and women who did have pain sought invasive therapy at a rate lower than did men (6 vs 11%, p < 0.05). 21
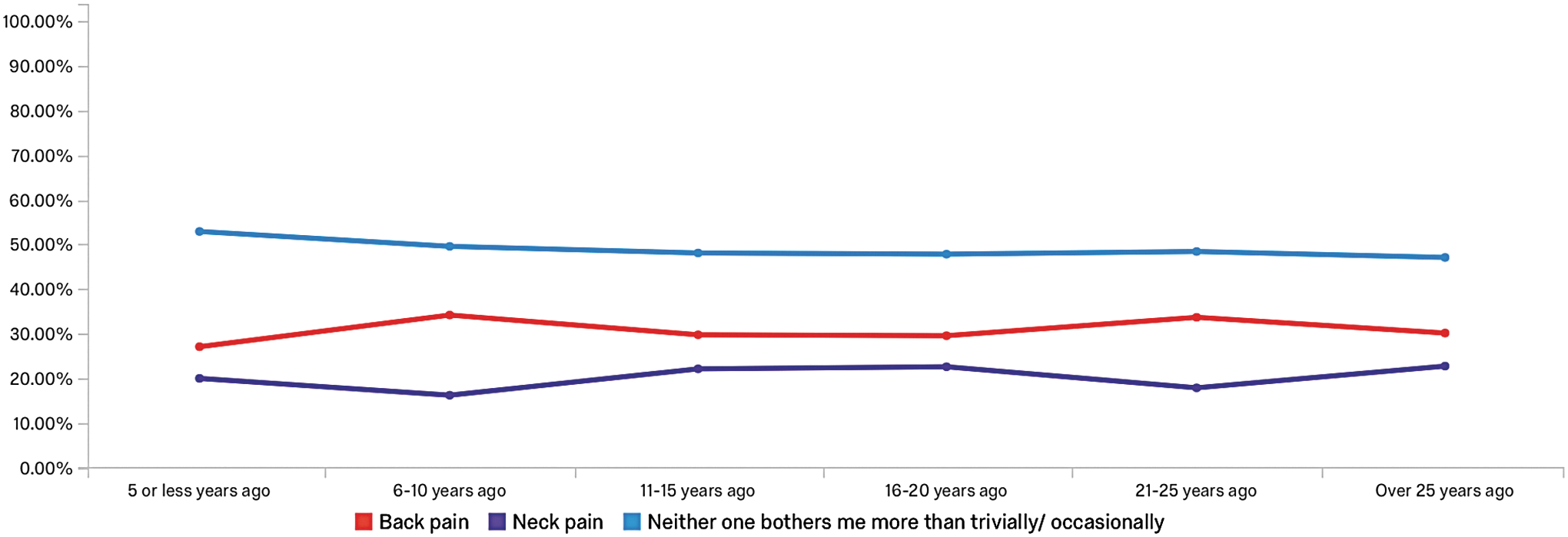
Relationship between duration of career and percentage of respondents reporting neck or back pain. Reporting of both was allowed, thus totals may not equal 100%.
Discussion
Two indelible features of modern bipedal life are work and spinal pain. The relationship between the two is unclear, but clearly many workers with bother are willing to blame these spinal issues on their job (47% in our survey). However, finding a correlation that fits Hill's classic criteria for causality 22 is not possible within this data set.
This is the largest worldwide study of surgeon work-related complaint and injury to date, and it contains good news for practicing surgeons. Despite long careers in the highly varied types of urologic surgery, there appears to be no relationship across the duration of career, and no identifiable dose–response between types of surgery or relative self-reported volumes of operating. The 1980s cinema appears to have had it right in professing “Life is pain … anyone who says otherwise is selling something.” 23 Even a long career performing surgery, fortunately, appears not to be associated with additional pain.
We explored the mythology associating optical cystoscopy with surgeon neck pain and injury. Anecdotally, significant volumes of optical cystoscopy relate to neck discomfort at the time of performance. However, we again were unable to find any correlation between the amount of this practice and the incidence of neck or back damage or issues that persist beyond the surgeon leaving the room.
Surgeons undoubtedly self-select for careers and types of surgery that feel good to them and are pleasant to perform. Few people of any vocation would actively pursue high volumes of a task that is severely uncomfortable for them, and although surgeons are certainly a driven group, we find no evidence that even in the face of high volumes of particular types of procedures, injuries are being incurred. We observe a lower rate of pain reported by North American surgeons than the rest of the world, and also less pain in women than in men. This mirrors other much larger global assessments of back pain, which also find lower rates in North America than essentially any other world region, and also again find similarly lower rates in women. 24 Whether this reflects variances in activity levels, diet or a higher ability to choose a nondamaging vocation is unclear, but our findings are parallel with these studies.
Comfort and ergonomic appropriateness during surgery should not be ignored. Although our study does not address this, it seems hard to imagine that the operations themselves are performed better or with superior outcomes in the setting of high surgeon discomfort. Allowing the practitioner to relax and focus on the task in an easy and nonstressful setting is intuitively an attractive approach, and these authors strongly support the ongoing study of ergonomics.
Nearly half of our respondents with pain (47%) blame their maladies on their vocation. Whether work represents a convenient scapegoat or a plausible assumption in the absence of acute injuries outside of work, we find no evidence supporting this attribution of pain to surgical workload. We feel this study provides reassurance that continued work, even high-volume work, is safe and allows surgeons to redirect their focus toward other more holistic approaches such as weight loss and increased exercise. However, the interplay of pain with work and burnout deserves exploration: with 21% of respondents in this study reporting significant pain that they blame on their work, the relationship of this meaningful complaint to the workplace and continued career enjoyment is in critical need of exploration in a specialty that reports concerning burnout rates.
Weaknesses and limitations of this study include all the challenges of extrapolating survey-based data to a broad population. Although attempts were made to present the survey content and questions as blandly as possible, selection bias either to avoid or seek to answer pain-related questions may have resulted in a nonrepresentative analysis of practicing urologists. Second, these data rely on urologists who are members of professional societies who themselves may represent a subset of practitioners who are more engaged in their practices, and may differ in BMI, exercise, surgical volume, and rates of pain from nonsociety members. Conversely, nonemail responsers may be busy living their pain-free life.
Challenges in interpretation of orthopedic damage as a consequence of surgery include the fact that in modern day life, physicians in general have a degree of latitude to choose vocation and work hours that was entirely unavailable to the workers in the industrial revolution, or for that matter many contemporary workers who lack the same control over their vocation. A medical student who is uncomfortable with the physical demands of surgery, we suspect, will be far less likely to choose a career in that field. Even within urology, choice and evolution of practice occur—surgeons have the ability to change the surgical content of their practices to avoid unnecessary volumes of procedures that they do not find comfortable.
Conclusions
In this large worldwide survey of urologists, we find no damaging effects on the spine from the act of performing surgery, regardless of duration, intensity, surgical modality, setting, or region of practice. It should be good news to urologists of all varieties that, despite studies reporting discomfort at the end of the surgical workday, there appears to be no relationship between long-term pain and the likelihood of undergoing surgery/intervention of the spine. Exercise and BMI appear associated with less development of back pain, and women who have pain seek intervention less than men.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix S1
Abbreviation Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.