
Abstract
Objective:
The aim of this study was to explore a new treatment strategy for left renal vein tumor thrombus directed at the thrombus level and the therapeutic effect of robotic surgery.
Materials and Methods:
Fifteen patients with left renal cell carcinoma with renal vein tumor thrombus (Mayo level 0) who underwent robotic radical nephrectomy and thrombectomy from July 2013 to July 2017 were included in this series. If the left renal vein thrombus transcended the superior mesenteric artery (SMA), the thrombus was classified as level 0b, the patient was positioned right side up for thrombectomy and repositioned left side up for nephrectomy, and angioembolization of left renal artery was necessary; otherwise, the thrombus was classified as level 0a and the patient was positioned left side up for both nephrectomy and thrombectomy. Baseline, perioperative, and follow-up data were analyzed.
Results:
Of all 15 patients, 10 had a level 0a tumor thrombus and 5 had a level 0b tumor thrombus. For level 0a patients, median operating time was 130 minutes, median estimated blood loss was 125 mL, with no patient receiving transfusion, and median hospital stay was 3.5 days. For level 0b patients, median operating time was 180 minutes, median estimated blood loss was 250 mL, with one patient receiving transfusion, and median hospital stay was 5 days. No perioperative complications or positive surgical margins occurred. For level 0a patients, one patient with preexisting lumbar vertebral metastasis died during a median follow-up of 39 months. For level 0b patients, all patients were alive at a median follow-up of 16.5 months.
Conclusions:
Our initial experience shows that the new treatment strategy for left renal vein tumor thrombus with the SMA as a dividing landmark directed at the thrombus level is safe and feasible. A larger cohort of level 0b patients and longer-term follow-up are needed to further assess the strategic advantages.
Introduction
Renal cell carcinoma (RCC) accounts for 2% to 3% of malignancies in adults 1 and has a natural propensity to extend into the venous system in 4% to 10% of cases. 2 Surgical management of RCC with venous extension has advanced over the past few decades, 2 –10 with the most favorable 5-year cancer-specific survival rate after radical surgery at 65%. 11 Laparoscopic or robot-assisted surgery for treatment of RCC with venous thrombus has been emerging in recent years. Although inherently challenging, several minimally invasive step-by-step procedures have been established through continued efforts by pioneers in the field. 6 –10
Due to a different anatomy on each side, management of left RCC with venous thrombus is more complex. 8 The left renal vein measures 6 to 10 cm, which is much longer than the right renal vein, and transcends the aortic artery and superior mesenteric artery (SMA). Therefore, tumor thrombus of left RCC is more frequently confined to the renal vein compared with right-sided tumors. 12 Several laparoscopic procedures for management of left renal vein thrombus (Mayo level 0) have been reported over the last decade. 13 –16 Desai et al. 13 described a transperitoneal laparoscopic technique using the Endo GIA stapler to transect the renal vein in cases of left RCC with level 0 thrombus. Wang et al. 16 later described a retroperitoneal laparoscopic technique based on varying lengths of left renal vein thrombi. However, if the left renal vein thrombus transcends the SMA, the left renal vein must be mobilized as proximal as possible toward the inferior vena cava (IVC) using either a transperitoneal or retroperitoneal approach, as previously described, 13,16 which is difficult because the SMA and aortic artery need to be mobilized to a great extent and may be injured during the dissection process. Hence, development of a modified minimally invasive procedure for treatment of left RCC with level 0 thrombus is greatly needed.
In the present study, we reclassified level 0 tumor thrombi of left RCC into 0a and 0b based on whether the thrombus transcended the SMA and developed a new robotic strategy for different thrombus levels.
Materials and Methods
Patients
A total of 15 patients diagnosed with left RCC with a renal vein tumor thrombus (Mayo level 0) and who underwent robotic radical nephrectomy and thrombectomy were included in this series. All cases were managed by a single combined robotic team from July 2013 to July 2017. Exclusion criteria were tumor thrombus invading the IVC (levels I–IV) and multifocal metastatic disease. Renal vein thrombus was originally classified according to the Mayo Clinic experience, 2 and four patients had preexisting single focal metastasis. This study was approved by the Ethics Committee of Chinese PLA General Hospital, and written informed consent was obtained from all patients.
Preoperative assessment and preparation
Routine preoperative workup was performed in all patients, and complete blood count, liver function, renal function, and serum electrolytes were all within normal limits. Color Doppler ultrasonography, computed tomography, and magnetic resonance imaging were used to define tumor location and renal vein extension in all patients. If the left renal vein thrombus transcended the SMA, we classified the thrombus as level 0b (Fig. 1B); otherwise, the thrombus was classified as level 0a (Fig. 1A). Angioembolization of the left kidney should be performed in patients with level 0b tumor thrombus. For patients with level 0a tumor thrombus, angioembolization is optional. The embolic material used is Gelfoam (Alicon, Hangzhou, China), and embolization occurs at the left renal artery trunk.
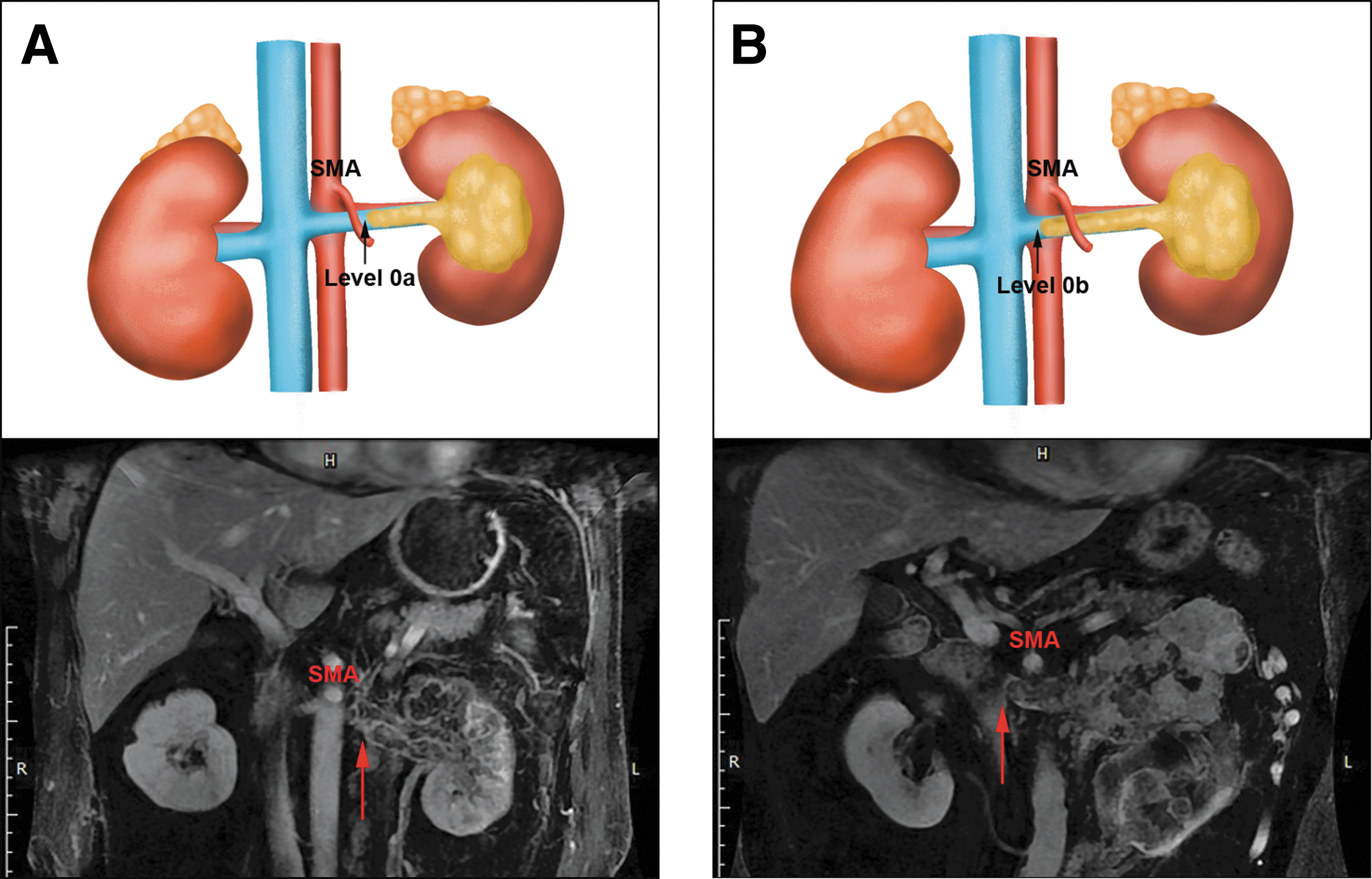
Schematic diagram and representative MRI of left RCC with level 0a
Surgical technique
Pure, transperitoneal, robotic radical nephrectomy and thrombectomy were performed in all cases.
For patients with a level 0a tumor thrombus, the patient was secured in a modified right lateral decubitus position with a 70° bump (Fig. 2A). Port placement and robot docking were the same as previously described for left radical nephrectomy. 8 After splenocolic ligament incision, the descending colon was reflected medially to expose the thrombus-bearing left renal vein (Fig. 2B). The left renal artery behind the renal vein was dissected and ligated using Hem-o-lok clips (Fig. 2C). The tributaries of the left renal vein were divided, and the left renal vein was mobilized as proximal as possible toward the SMA. The segment of the proximal renal vein uninvolved with the thrombus was flat in appearance. When necessary, intraoperative ultrasonography was used to identify the extent of the thrombus. The thrombus-free segment of the left renal vein was ligated using Hem-o-lok clips (Fig. 2D) or transected using the Endo GIA stapler. If angioembolization of the left kidney was performed preoperatively, the thrombus-bearing left renal vein could be controlled first, followed by ligation of the left renal artery (Supplementary Video S1). After radical nephrectomy, ipsilateral lymphadenectomy was performed, and the left kidney along with the level 0a renal vein thrombus was removed in an EndoCatch bag.

Radical nephrectomy and thrombectomy for left RCC with level 0a renal vein thrombus:
For patients with a level 0b tumor thrombus, we initially secured the patient with the right side up to facilitate exposure and control of the proximal renal vein thrombus. The patient was secured in a modified left lateral decubitus position with a 70° bump (Fig. 3A). Port placement and robot docking were the same as previously described for IVC thrombectomy. 8 After hepatocolic ligament incision and liver retraction, the ascending colon and duodenum were reflected medially to expose the IVC and thrombus-bearing left renal vein (Fig. 3B). The left renal vein was mobilized as proximal as possible toward the IVC, and the segment of the proximal renal vein uninvolved with the thrombus was flat in appearance. When necessary, intraoperative ultrasonography was used to identify the extent of the thrombus. The thrombus-free segment of the left renal vein was transected using the Endo GIA stapler (Fig. 3C, D), and the patient was repositioned right side up for left radical nephrectomy. Patient position, port placement, robot docking, and procedure were the same as described for level 0a thrombus management, except that we only need to mobilize the ligated left renal vein (Fig. 4) (Supplementary Video S1). After radical nephrectomy, ipsilateral lymphadenectomy was performed, and the left kidney along with the level 0b renal vein thrombus was removed in an EndoCatch bag.
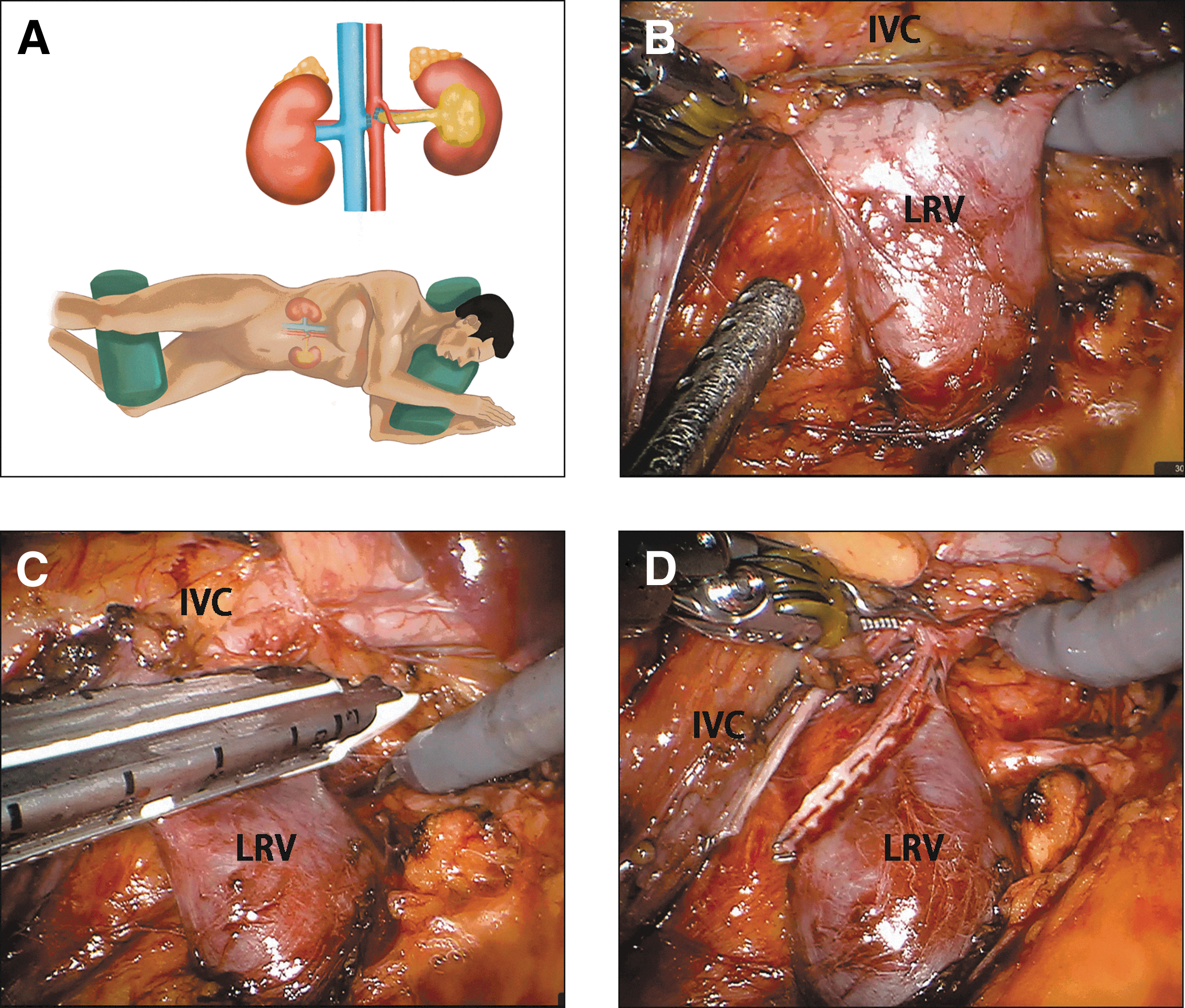
Thrombectomy for left RCC with level 0b renal vein thrombus:

Radical nephrectomy for left RCC with level 0b renal vein thrombus:
Postoperative care and follow-up
Standard postoperative care, including nutrition, pain control, and early ambulation, was provided to all patients. Follow-up consisted of history, physical examination, laboratory tests, and imaging surveillance at recommended intervals according to patient stage. 17
Data collection and analysis
Data were obtained retrospectively from our renal database. Baseline characteristics, including age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) score, Charlson comorbidity index (CCI), preoperative creatinine, tumor size, preexisting metastatic condition, thrombus length, thrombus level (new classification of renal vein thrombus), and preoperative angioembolization status, were assessed. Perioperative data, including operating time, estimated blood loss, length of hospital stay, transfusion rate, margin status, lymph node status, and complications, also were assessed. Tumor histology and survival status were recorded. RCC was staged according to the American Joint Committee on Cancer 2010 TNM staging criteria, 18 and complications were graded according to the Clavien-Dindo system. 19 Continuous data are presented as median and range, while categorical data are presented as number and percentage.
Results
According to our new classification of left renal vein thrombus, of all 15 patients, 10 (66.7%) had a level 0a tumor thrombus and 5 (33.3%) had a level 0b tumor thrombus. For level 0a patients, the median thrombus length was 2.4 cm (range 1–3.5 cm), preoperative creatinine was 85.5 μmol/L (range 64.3–215.1 μmol/L), four patients (40%) had preexisting single focal metastasis (one pulmonary, one lumbar vertebra, and two ipsilateral adrenal gland), and five patients (50%) had preoperative angioembolization of the left kidney. For level 0b patients, the median thrombus length was 7 cm (range 5–9 cm), preoperative creatinine was 118 μmol/L (range 82.6–130.9 μmol/L), no preexisting metastasis was present, and all five patients (100%) had preoperative angioembolization of the left kidney. Other baseline characteristics, such as age, sex, BMI, ASA score, CCI, and renal tumor size, were comparable between level 0a and 0b patients (Table 1).
Baseline Characteristics
Continuous data are presented as median (range), and categorical data are presented as n (%).
ASA = American Society of Anesthesiologists; BMI = body mass index; CCI = Charlson comorbidity index.
All cases were managed according to our new strategy directed at our new classification of left renal vein thrombus without open conversion. For patients with ipsilateral adrenal gland metastasis, ipsilateral adrenalectomy also was performed. For level 0a patients, median operating time was 130 minutes (range 90–165 minutes); median estimated blood loss was 125 mL (range 20–700 mL), with no patient receiving transfusion; median hospital stay was 3.5 days (range 2–8 days); and one patient was found to have positive lymph nodes (10%). For level 0b patients, median operating time was 180 minutes (range 150–315 minutes); median estimated blood loss was 250 mL (range 100–1000 mL), with one patient receiving transfusion; median hospital stay was 5 days (range 3–11 days); and one patient was found to have positive lymph nodes (20%). No perioperative complications or positive surgical margins occurred. Perioperative and pathologic data of both level 0a and 0b patients are listed in Table 2.
Perioperative, Pathological, and Follow-Up Data
Adjuvant refers to immunotherapy or targeted therapy. Continuous data are presented as median (range), and categorical data are presented as n (%).
Table 2 also presents follow-up data. For level 0a patients, median follow-up time was 39 months (range 22.1–61.4 months), five patients (50%) with preexisting metastatic disease or positive lymph nodes received adjuvant therapy, and one patient (10%) with preexisting lumbar vertebral metastasis died at a postoperative survival time of 22.1 months. For level 0b patients, median follow-up time was 16.5 months (range 13.5–36.3 months), one patient (20%) with positive lymph nodes received adjuvant therapy, and all patients were alive at the final follow-up. No patient developed new-onset metastatic disease.
Discussion
Step-by-step procedures for robotic level I–III IVC tumor thrombectomy have been carefully documented and their feasibility and safety well testified. 8,10 Compared with IVC tumor thrombus, left renal vein tumor thrombus (level 0) is more common in patients with RCC 2,12 and its treatment strategy should be given more attention.
As the left renal vein transcends the aortic artery and SMA, it is difficult to perform thrombectomy in left-sided cases if the thrombus extends beyond the SMA. In 2003, Desai et al. 13 reported successful transperitoneal laparoscopic radical nephrectomy with left renal vein thrombectomy. In that case, the left renal vein thrombus extended up to the interaortocaval region, and the surgeon carefully mobilized the SMA to create adequate space for engaging the Endo GIA stapler on the uninvolved left renal vein adjacent to the IVC. Since then, similar techniques have been adopted at other centers with minimally invasive expertise. 14,15 In 2014, Wang et al. 16 categorized patients with left RCC with renal vein thrombus into four grades based on the distal limit of the thrombus and described their retroperitoneal laparoscopic technique for different thrombus extensions. For a left renal vein thrombus extending beyond the SMA (grades 3 and 4 according to their classification), the surgeon also needs to mobilize the SMA to reach the junction of the left renal vein and IVC. Although feasible, the issue with these two procedures is that they both need to mobilize the SMA to reach the distal limit of the thrombus and there is high risk of SMA injury and consequent hemorrhage during this process. Therefore, how can we avoid mobilizing the SMA too much and still have adequate space for controlling the distal limit of the left renal vein thrombus?
Our team previously reported a robotic technique for level I–II IVC thrombectomy for left RCC. 8 Essential aspects of this procedure include initially securing the patient with the right side up for IVC thrombus control and then repositioning with the left side up for radical nephrectomy. We also considered applying this strategy to left renal vein thrombus management so that we would not need to mobilize the left renal vein all the way from the left kidney to the IVC. Instead, we could mobilize proximal and distal parts of the left renal vein separately. That way, we would not need to mobilize the SMA too much either. To make the treatment strategy for left renal vein tumor thrombus more specific, we reclassified left renal vein tumor thrombus into levels 0a and 0b. Level 0b indicates that the thrombus transcends the SMA, in which case we adopt the reposition strategy. Level 0a indicates that the thrombus is confined to the left side of the SMA and we can complete both radical nephrectomy and thrombectomy with the left side up, which requires much less time than repositioning.
When we first manage the tumor-bearing left renal vein with level 0b thrombus with the right side up, we can hardly control the left renal artery. Therefore, preoperative angioembolization of the left kidney is an essential step for level 0b tumor thrombus so that blood loss can be greatly decreased. For management of level 0a thrombus, because we can first control the left renal artery with the left side up, preoperative angioembolization of the left kidney is optional. Thus, we only applied angioembolization to larger tumors or suspicious lymphadenopathy in level 0a patients. To eliminate the potential for inducing a perirenal inflammatory reaction, 20 angioembolization of the left kidney was performed 1 to 2 hours before surgery. The tumor-free segment of the left renal vein usually appears collapsed, and intraoperative ultrasonography can be used to identify the extent of the thrombus.
Our initial experience with this new classification and robotic strategy for left RCC with renal vein tumor thrombus is encouraging. For level 0b patients, median operating time was longer (180 vs 130 minutes), median estimated blood loss was greater (250 vs 125 mL), and median hospital stay was longer (5 vs 3.5 days) compared with level 0a patients. These results can be explained by the repositioning procedure and more abundant venous collaterals of level 0b patients. Therefore, the new classification of left renal vein thrombus should be accurate as the new strategy directed at this classification can not only save operating time for level 0a patients but also make the operation safer for level 0b patients. We have performed surgeries for four level 0a patients with preexisting metastasis, as nephrectomy and thrombectomy are associated with improved overall survival of these patients, 20 and our results showed that only one patient with preexisting metastasis died during follow-up of 22.1 months and other patients had been in good status so far.
Several limitations of this study should be noted. First, the level 0b patients were a relatively small cohort (n = 5). Second, although no patient developed new-onset metastatic disease and only one patient with preexisting metastasis died, follow-up time was relatively short (median of 39 months for level 0a patients and 16.5 months for level 0b patients). Thus, the long-term oncologic effect of this procedure should be determined in the future.
Conclusions
Our initial experience shows that classification of left renal vein tumor thrombus based on whether the thrombus transcends the SMA and the new strategy directed at the thrombus level are safe and feasible. A larger cohort of level 0b patients and longer-term follow-up are needed to further assess the strategic advantages.
Footnotes
Acknowledgment
This work was financially supported by the National Natural Science Foundation of China (No. 81702492).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Video S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.