
Abstract
Introduction:
Tissue retraction during minimally invasive surgery has been achieved to date with patient positioning or additional instrumentation. The Levita™ Magnetic Surgical System (San Mateo, CA), a novel, noninvasive, magnetic retraction device for minimally invasive surgery, has been used to facilitate reduced-port robotic prostatectomy using a multiport robotic platform. With the release of the da Vinci SP robotic system (Intuitive, Sunnyvale, CA), we now report a multi-institutional initial case series of magnet-assisted robotic prostatectomy using the single-port robotic platform.
Materials and Methods:
An IRB-approved, retrospective chart review was performed of all patients undergoing robot-assisted radical prostatectomy using the da Vinci SP surgical system and a single Levita magnetic retractor in treatment of prostatic adenocarcinoma at two institutions from November 2018 to January 2019. Preoperative, intraoperative, and postoperative data were collected for descriptive analysis.
Results:
A total of 15 men, median age 62 years (range 57–71), with mean PSA 7.0 ± 2.3 underwent surgery. The robotic cannula and a single 12-mm assistant port were utilized in all cases, the latter for suction, suture passage, and clip placement; the magnetic retractor aided with posterior dissection, dorsal venous complex stitch placement, bladder neck dissection, and lymphadenectomy. No cases required conversion to a multiport robotic platform, laparoscopy, or open surgery, nor placement of additional assistant ports. No intraoperative or postoperative complications occurred. Average operative time was 224 ± 43 minutes and blood loss was 198 ± 115 mL. All patients were discharged home within 2 days of surgery.
Conclusions:
Robotic prostatectomy utilizing the da Vinci SP system is feasible, safe, and effective. Use of the magnetic retractor facilitates tissue exposure and improves procedure ergonomics, mimicking the conventional multiport technique. Further exploration of magnet utilization in robotic surgery and optimization of assistant port placement for true single-site surgery is warranted.
Introduction
In minimally invasive surgery, tissue retraction has traditionally been accomplished by placement of additional ports either for a bedside assistant, and/or 4th robotic arm, or patient positioning. With introduction of laparoendoscopic single-site (LESS) surgery, 1 a need for a noninvasive means of tissue retraction emerged to overcome exposure and ergonomic challenges.
The Levita™ Magnetic Surgical System (San Mateo, CA), a magnetic retraction device for use in minimally invasive procedures, was developed and has shown safety and efficacy in cholecystectomy 2 and bariatric surgery. 3 The device has recently been utilized to perform reduced-port robotic prostatectomy on a multiport robotic platform. 4 The recent release of the da Vinci SP robot (Intuitive, Sunnyvale, CA), a dedicated, single-port robotic system, continues to advance the minimally invasive nature of surgical technology. We now report a multi-institutional initial case series of magnet-assisted robotic LESS prostatectomy using the single-port robotic platform.
Materials and Methods
All patients undergoing robot-assisted radical prostatectomy in the treatment of prostatic adenocarcinoma using the da Vinci SP surgical system and the Levita magnetic retractor (LMR) at two institutions (Mayo Clinic [MC] and University of Texas Southwestern [UTSW]) from November 2018 to January 2019 were reviewed. All cases were completed by one of two experienced robotic surgeons (M.T.G. and J.A.C.). Preoperative demographics and disease characteristics (e.g., body mass index [BMI], PSA, and clinical stage), intraoperative data (e.g., operative time and estimated blood loss), and postoperative data (e.g., hospitalization time, complications, and final pathology staging) were collected for descriptive analysis.
Port placement
All patients were placed in the Trendelenburg position on a split-leg bed with arms tucked. A 2.5-cm midline supraumbilical incision was made and access to the abdomen completed using the Hasson technique. This was typically performed 3 cm superior to the umbilicus. The robotic cannula was placed directly into the abdomen, which was then insufflated. A 12-mm assistant port was placed 10 cm away from the robotic cannula in the left lateral abdomen for suction and clip application (Fig. 1). Instruments used were monopolar scissors in arm 3 (right hand), Maryland dissector in arm 1 (left hand), and Cadiere grasper in arm 2 (4th arm). It is important to communicate using this new numerical nomenclature given the ability of the single-port system to rotate into both a camera above (Fig. 2A) and camera below position (Fig. 2B).
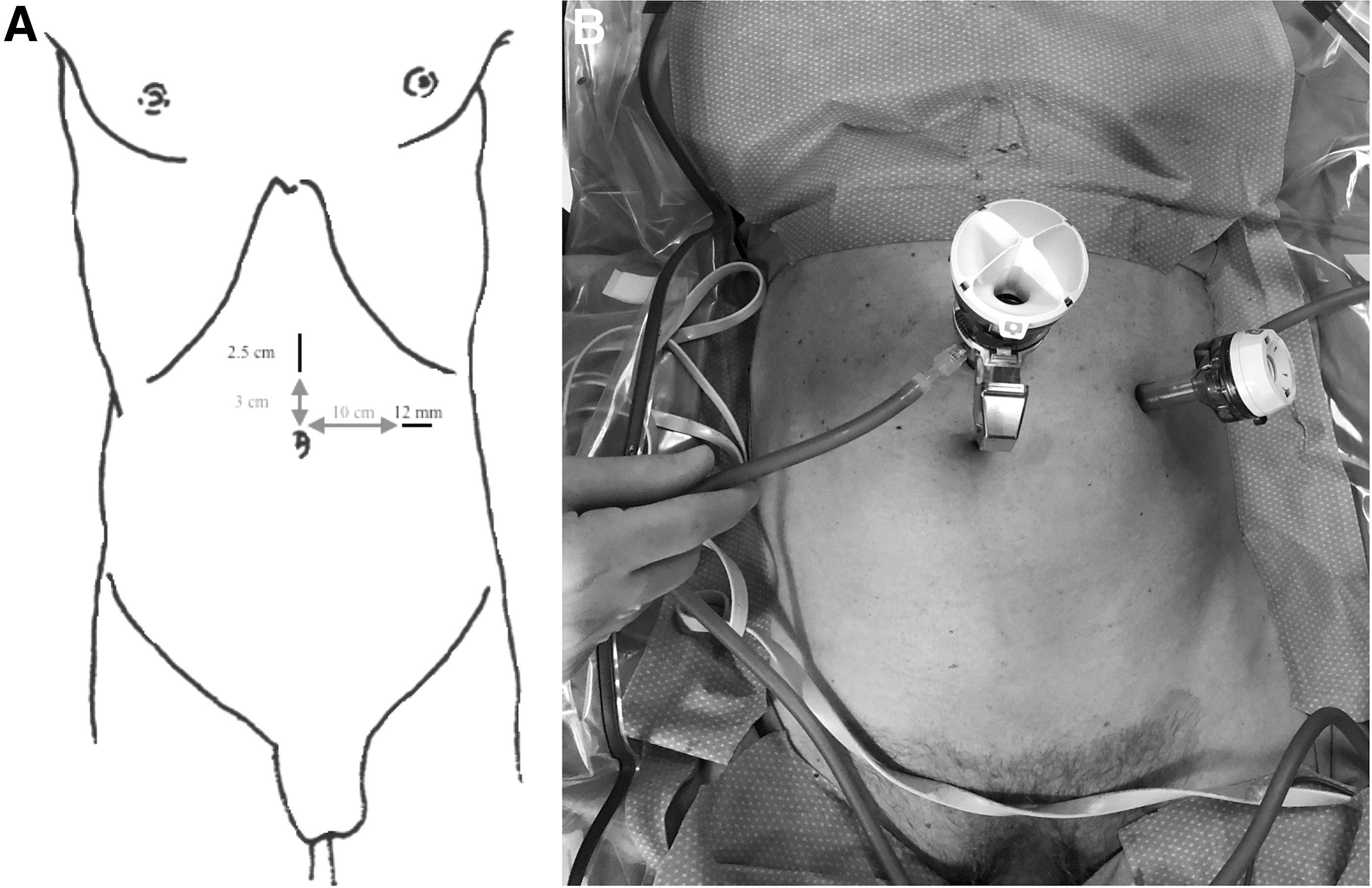
Schematic

da Vinci SP robotic cannula in the
UTSW approach
With the camera in the above position, a posterior approach was initially performed. The LMR was placed on the sigmoid colon for retraction out of the pelvis and the vasa and seminal vesicles were exposed. The LMR was then replaced on the peritoneum posterior to the bladder neck, providing anterior retraction during seminal vesicle dissection and the opening of Denonvilliers' fascia (Fig. 3A). Once the posterior dissection was complete, the robotic cannula was rotated into the camera below position to drop the bladder by transecting the urachus and medial umbilical ligaments. Once the dome of the bladder was dropped, the cannula was placed back into the camera above orientation. The remainder of the bladder was dropped, anterior prostate defatted, and endopelvic fascia opened.
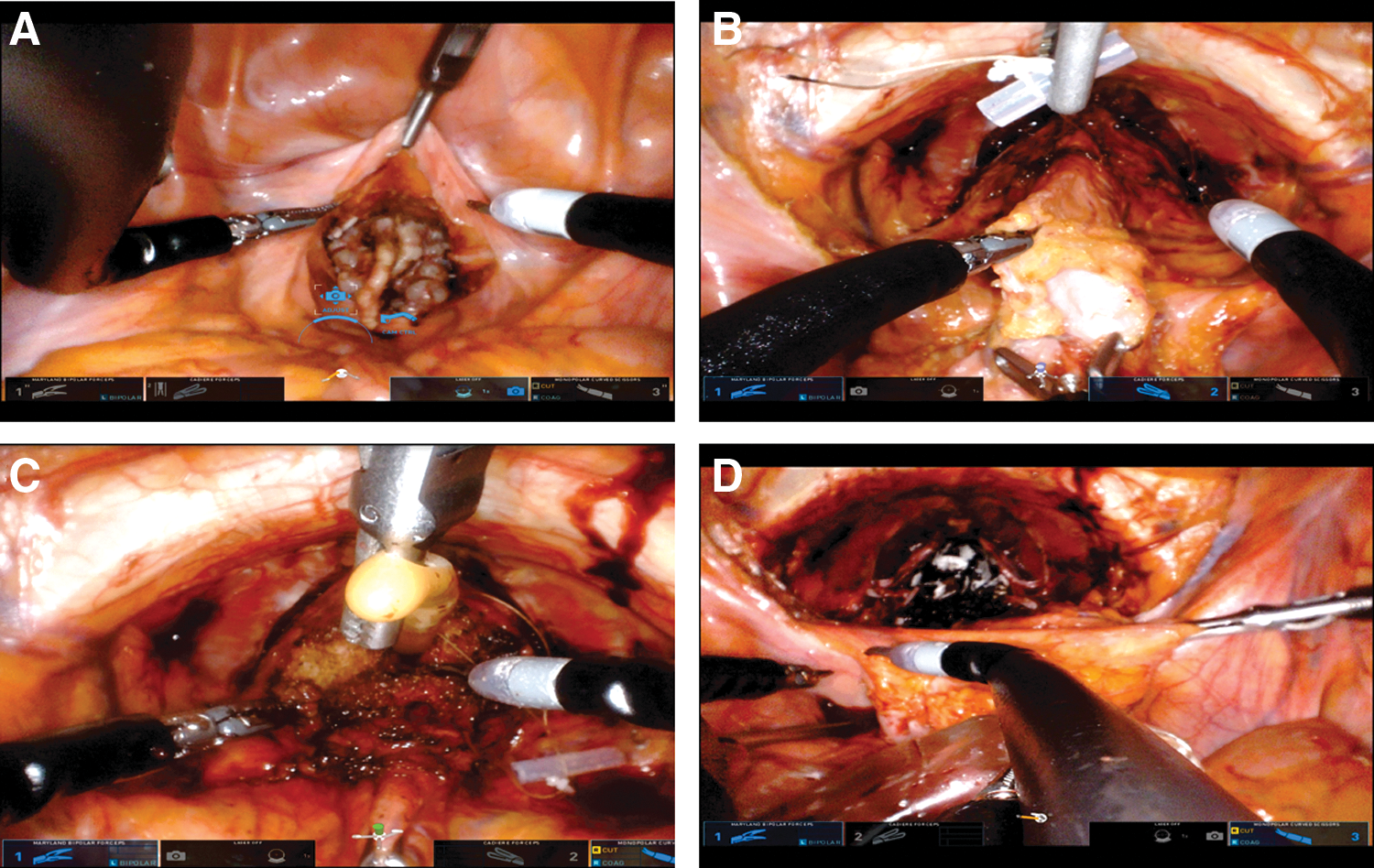
Intraoperative images of the magnetic retractor performing
A retraction suture was then placed at the level of the bladder neck. The LMR was placed on the retraction suture to provide anterior and cephalad retraction during dorsal venous complex (DVC) suture ligation with a 3-0 barbed suture. The LMR was then repositioned further caudal, still affixed to the retraction suture, to provide anterior countertraction during bladder neck dissection. The bladder neck was spared in all cases (Fig. 3B, C). The LMR was then moved to the seminal vesicles for superolateral retraction during ligation of the lateral bladder attachments. Arm 2 of the robot was used for prostate retraction during neurovascular bundle release. Nerve sparing was attempted in all cases. The prostatic pedicles were isolated and clipped in a standard manner. The apex was dissected free, completing the prostatectomy.
The LMR was then placed on the bladder to provide contralateral retraction during pelvic lymphadenectomy (Fig. 3D). All patients underwent a standard pelvic lymph node dissection with removal of the external iliac and obturator lymph node packets. The anastomosis was performed using a standard van Velthoven technique with a 3-0 barbed suture. A posterior urethral suspension was performed using two 2-0 polyglactin sutures. An 18F urethral catheter was left in place. The bladder was filled with 300 mL of saline to confirm no anastomotic leak. A 16F suprapubic tube was placed using a punch kit, as is routine practice for patients undergoing robotic prostatectomy by this surgeon. No drains were placed after confirming no anastomotic leak.
Mayo Clinic approach
An anterior approach was employed. The robotic cannula was placed into the camera above position. The urachus and medial umbilical ligaments were transected and the bladder was dissected off the anterior abdominal wall using sharp and blunt dissection, the anterior prostate defatted, and the endopelvic fascia opened. A retraction suture was then placed at the level of the bladder neck. The LMR was placed on the retraction suture to provide anterior and cephalad retraction during DVC suture ligation with a 1-0 polyglactin suture. The LMR was then repositioned further cephalad, still affixed to the retraction suture, to provide anterior countertraction during bladder neck dissection performed using a bladder neck-sparing technique.
After completion of the bladder neck, the vas deferens and seminal vesicles were then isolated and dissected free from surrounding structures. The LMR was then moved to the seminal vesicles for superolateral retraction during ligation of lateral bladder attachments. Neurovascular bundle release was then performed in all patients using arm 2 of the robot to provide lateral retraction. The prostatic pedicles were clipped in a standard manner. The apex was dissected free, completing the prostatectomy. The LMR was then placed on the bladder to provide contralateral retraction during pelvic lymphadenectomy (Fig. 3D). All patients underwent standard pelvic lymph node dissection with removal of the external iliac and obturator lymph node packets. The anastomosis was performed using a standard van Velthoven technique with a 3-0 barbed suture. An 18F urethral catheter was left in place. The bladder was filled with 120 mL of saline to confirm no anastomotic leak. No drains were placed after confirming no anastomotic leak.
Results
A total of 15 men of median age 62 years (range 57–71 years) underwent surgery as described above. Baseline patient demographics and preoperative disease characteristics can be seen in Table 1.
Demographics and Preoperative Disease Characteristics
BMI = body mass index.
No procedures required additional port placement or conversion to other robotic platforms or open surgery. No intraoperative complications occurred. Subjectively, the tissue on which the magnetic retractor was placed demonstrated no crush injuries or other damage after removal. Exposure was deemed adequate using the SP robot and magnetic retractor for all facets of the operation. Mean operative time was 224 ± 43 minutes and mean blood loss was 198 ± 115 mL. No patient required transfusion. All patients were discharged home by postoperative day (POD) 2. At USTW, all patients had their urethral catheters removed and suprapubic tubes placed for drainage on POD1. Suprapubic tubes were capped by patients at home on POD 8 and removed in the clinic on POD 9 or POD 10. At Mayo clinic, urethral catheters were left in place for 7 days. Neither institution performed postprocedural imaging before catheter removal.
Catheters were left in place for 7 days and no further postoperative imaging was obtained.
Table 2 demonstrates intraoperative and postoperative outcomes. Two patients were found to have both positive lymph nodes and positive margins. The margins were noted at the bladder base in one and the bladder base and apex in the other. Both patients had pT3b disease, one with grade group 3 disease with a tertiary 5 pattern and the other with grade group 5 disease. The sole 30-day complication was a patient readmitted for a TIA 2 weeks after surgery (Clavien-Dindo grade 4).
Intraoperative and Postoperative Patient Outcomes After Magnet-Assisted Robotic Prostatectomy
Discussion
This is the first report to describe magnet-assisted robotic LESS prostatectomy using the da Vinci SP robotic platform. We demonstrate that the procedure is both safe and feasible without significant alteration in the steps of the procedure. No transfusions or major complications occurred in any patients.
Minimally invasive urologic surgery has evolved greatly since the initial laparoscopic nephrectomy was completed. 5 After describing other urologic procedures, such as pyeloplasty, 6 LESS surgery 1 was explored in an effort to further reduce the invasiveness of laparoscopy, which was quickly followed by natural orifice transluminal endoscopic surgery (NOTES). 7 Later, robotic LESS, 8 utilizing multiport robotic systems in a reprogrammed cross-armed manner and with novel curved instruments, was described. These techniques were not widely adopted due to increased procedural difficulty, particularly with suturing and instrument clashing. Recently, the da Vinci SP robotic surgical system (Intuitive), a dedicated single-port robot, was approved by the Food and Drug Administration (FDA) for radical prostatectomy and clinical utilization has begun.
Over this same time period, magnetic actuation of laparoscopic surgical equipment, including but not limited to the camera and retractors, was explored both in transabdominal single-site surgery 9 –12 and NOTES. 13 Unfortunately, further development was limited by the optical quality of the camera and rapid adoption of robot-assisted laparoscopic surgery. Recently, the Levita magnetic system was FDA approved for retraction in patients with a BMI as much as 60. Our group has previously reported on the use of the device as a means of performing reduced-port robotic prostatectomy on the multiport robotic platform. 4 There are no absolute contraindications to using the LMR, although in patients with pacemakers, a 20-inch (50 cm) distance between the pacemaker and the external magnet is recommended.
The LMR compliments the advantages of the SP robotic system for robotic LESS procedures. The LMR has no limitation to the angle or exact vector of upward or lateral retraction that can be achieved. In standard multiport robotics, the direction of retraction is constrained by robotic instrument joints and port placement, which could lead to robotic arm collisions. Using the LMR for anterior/lateral retraction frees robotic arm 2 to perform other retractions, namely in a posterior direction. This replicates the actions of the assistant or 4th arm in conventional, multiport robotic surgery. Furthermore, the LMR can be placed in any part of the abdomen. As the SP robotic system allows for easy multiquadrant surgery, this may avoid the need to place additional assistant ports when moving to another portion of the abdomen in other procedures. While only utilized for bladder retraction during lymphadenectomy in this series, the wide range over which the LMR is capable of providing retraction may benefit urologists desiring to perform extended or superextended lymph node dissections for prostate or bladder cancer surgery. Finally, use of the LMR allows the bedside assistant to focus on suction/irrigation and clip application during the procedure, making the surgeon more autonomous.
We acknowledge that although the goal remains to perform procedures in a true single-incision manner, a separate assistant port was necessary. SP robotic systems do not have suction/irrigation capabilities and clip application would require replacement of one of the three working instruments, thereby increasing operative time due to the numerous arm changes required. Attempts have been made to perform the procedure in a true single-incision manner with the aid of GelPOINT (Applied Medical, Rancho Santa Margarita, CA), but the ability of the assistant to perform suction was limited by collisions with the robotic cannula.
The only other report, to our knowledge, on single-port robotic prostatectomy using the SP system involved a similar port placement strategy, including a separate assistant port for clipping and suction, but included a GelPOINT mini through which the robotic cannula was placed. 14 Furthermore, a Keith needle was placed percutaneously to provide upward retraction on the Foley catheter to complete the posterior bladder neck dissection. In our series, this was completed with the LMR. The main difference between techniques appears to be the use of upward retraction/countertraction in more circumstances in our series, which was easily accomplished with the LMR. Theoretical advantages of the GelPOINT include easier specimen extraction and placement of assistant ports within the GelPOINT, while advantages of the LMR include improved anterior retraction and liberating the assistant from the need to aid in retraction. Given the small number of cases completed, further comparison of techniques (e.g., operative time) is limited.
In completing these procedures, there are a few important observations made as part of the learning curve. While LMR retraction was optimal in this cohort, larger patients with thicker body walls may have weaker magnetic coupling at some locations given that magnetic force is proportional to the inverse of the square of the distance between the two magnets (force ∝1/r2). In addition, new robotic instruments present a number of new considerations. First, awareness of the instrument's elbows is important when working in tight spaces (e.g., deep pelvis). The elbows straighten during instrument removal, thus attention to straightening the arms before removal is essential to avoid damage to surrounding structures. In addition, given the presence of the elbow, the instrument wrist is changed and thus suturing feels like a hybrid of robotic and laparoscopic tools. As such, suturing directly back toward the robotic cannula/camera is not possible. Given the smaller size of the da Vinci SP robot arms (6 mm) compared with prior robotic platforms (8 mm) and implementation of the instrument elbow, the strength of robotic arms is reduced. Consequently, direct manipulation of the LMR with the robotic arms is not possible. Finally, the da Vinci SP robotic cannula is recognized by the robotic arm through detection of a magnet within the cannula. Contact of the external magnet of the LMR with the robotic cannula or arm risks disruption of this detection and development of a recoverable or unrecoverable fault. Thus, ensuring a least an 8–10-cm distance between the arm/cannula and external magnet is advised.
Conclusions
Magnet-assisted robotic LESS prostatectomy using the da Vinci SP robotic platform can be safely completed with only minor changes in the surgical approach. The magnetic retractor provides further surgeon autonomy, replicates the steps of a multiport robotic prostatectomy, and frees the bedside assistant to focus on suction and clipping. Optimizing the placement of the assistant port to allow for true single-site surgery is needed.
Footnotes
Author Disclosure Statement
J. Cadeddu is an investor and advisory board member for Levita Magnetics; M.T. Gettman is a consultant for Levita Magnetics and Intuitive Surgery; and R.L. Steinberg, B.A. Johnson, and M. Meskawi have no competing financial interests.
Funding Information
No funding was received for this article.