
Abstract
Background:
Although previous studies have compared the minimally invasive simple prostatectomy (MISP) with open simple prostatectomy (OSP) for large prostates, there is still controversy. This study aims to provide the latest evidence for clinical practice.
Materials and Methods:
We systematically searched Science, EMBASE, PubMed, and Clinicalkey databases for articles comparing MISP and OSP for large prostates. Result parameters including International Prostate Symptom Score (IPSS), quality of life (QoL), maximum urine flow rate (Q max), postvoid residual urine volume (PVR), operative time (OT), estimated blood loss (EBL), irrigation time (IT), catheterization time (CT), length of hospital stay (LOS), transfusion rate (TR), and complications were evaluated using RevMan 5.3.
Results:
A total of 995 patients were included in 10 studies. No statistically significant differences were found between two groups in IPSS (weighted average difference [WMD] = −0.36, p = 0.26), QoL (WMD = −0.22, p = 0.05), Q max (WMD = 0.46, p = 0.62), and PVR (WMD = −2.14, p = 0.65). The MISP group had similar IT (WMD = −1.52, p = 0.06), lesser EBL (WMD = −292.22, p < 0.001), shorter CT (WMD = −1.89, p < 0.0001), shorter LOS (WMD = −2.52, p < 0.001), lower TR (odds ratio [OR] = 0.21, p < 0.001), and lower complications (OR = 0.49, p < 0.001) compared with OSP group. However, the OT (WMD = 43.07, p < 0.001) of MISP was longer than that of OSP.
Conclusions:
The present results demonstrated that MISP provided similar efficacy to those of OSP while maintaining a better security. Our findings imply that MISP is a feasible and effective alternative to the OSP.
Background
Benign prostatic hyperplasia (BPH) is one of the common urinary diseases in elderly men and can have adverse effects on quality of life (QoL). About 1.1 billion men suffer from the disease and its associated clinical symptoms. 1 At present, the main treatments for BPH are medication and operation. After drug therapy, surgical intervention is often used as the final and most effective treatment. 2 As the guide records, operation is recommended for patients who have refractory urinary retention, overflow incontinence, recurrent urinary tract infections, bladder stones or gross hematuria because of BPH, and/or the medicine is not effective. 3
Over the past 5 years, holmium laser enucleation of the prostate (HoLEP) has been considered a feasible and potentially superior alternative to open simple prostatectomy (OSP), 4,5 because many studies have shown that it is an effective treatment for BPH regardless of prostate size. 6 However, its steep learning curve limited the wide-ranging implementation of this method and promoted the pursuit of alternatives. 7 With the increased experience of minimally invasive (laparoscopic and robotic) radical prostatectomy, minimally invasive simple prostatectomy (MISP) becomes the next logical step. Based on this situation, some urologists implemented MISP at their medical center and concluded that MISP is safe and feasible for large prostates. 8 –10 However, when compared with OSP, the effectiveness and safety of this procedure are still debated. 11 –13
Hence, we performed a systematic review and meta-analysis of comparative trials to determine the efficiency and safety of MISP vs OSP for large prostates, and provide the latest evidence for clinical practice.
Materials and Methods
Search strategy
We systematically searched all published literature on minimally invasive treatment of large prostates from January 2000 to March 2019 and used the following databases for examination: EMBASE, PubMed, Science, and Clinicalkey databases. Search terms included the following: “minimally invasive OR laparoscopic OR robotic OR robot-assisted” and “open prostatectomy OR open adenomectomy,” and “benign prostate hyperplasia OR prostatic hyperplasia OR prostate adenoma OR BPH,” and modified the corresponding search strategy according to the requirements of each database. In addition, a complete manual search of the references in the relevant articles, and the minutes and abstracts, was managed. Search was not limited by region or language. The document retrieval and screening process were completed independently by two examiners and settled through discussion.
Study selection
All eligible studies were enrolled in the meta-analysis based on predesigned inclusion and exclusion criteria. Inclusion criteria were as follows: (1) BPH was diagnosed in the study patients and required surgical intervention, and the patients' prostate volume was at least 80 mL or 80 g; (2) the study had a comparison between MISP and OSP, and at least one corresponding outcome indicator exists. Exclusion criteria were as follows: (1) experimental data were based on animal experiments; (2) research lacks control group; (3) lack of result data required for meta-analysis; and (4) the type of article was review, case report, or comment.
Data extraction
Two investigators independently extracted data from the qualified literature according to a predesigned standard form, and the differences were resolved through discussion. Finally, the following variables were extracted: first author, year of publication, study design, intervention, sample size, age, prostate volume, and duration of follow-up. In addition, the main outcome measures were also included: International Prostate Symptom Score (IPSS), QoL, maximum urine flow rate (Q max), postvoid residual urine volume (PVR), operative time (OT), estimated blood loss (EBL), irrigation time (IT), catheterization time (CT), length of hospital stay (LOS), transfusion rate (TR), and complications. In addition, the expression of the data in the article was converted to a mean ± standard deviation. 14,15
Study quality assessment
The Joanna Briggs Institute Critical Appraisal Checklist for Case-Control Studies was used by us to assess the quality of the included studies in the meta-analysis. The range is 0 to 10 scores, and the score is ≥7, designating that the included study is of high quality. 16 The two authors scored all the studies separately, disagreements were resolved by discussion. The funnel plot contributed a qualitative appraisal of the bias of published studies, with no evidence of bias (Supplementary Fig. S1).
Statistical analysis
When two or more studies reported the main result data, a pooled analysis was performed using RevMan v.5.3 (The Cochrane Collaboration, Oxford, United Kingdom), in which the dichotomous variables and continuous variables were compared by the weighted average difference (WMD) and odds ratio (OR), respectively. All results reported a 95% confidence interval (CI) and p-values. Heterogeneity was measured by the I 2 test. If the heterogeneity is high (I 2 >50%), the random-effects model was introduced, otherwise the fixed-effects model was utilized for meta-analysis. A subgroup analysis was also applied to probe possible discrepancies between groups. All p-values were two-tailed, and p < 0.05 was regarded as statistically significant.
Results
Description of studies
A total of 441 articles were preliminarily searched from the databases, and 178 duplicates and 224 irrelevant reports were removed. After reading the full text, 29 articles were excluded. Finally, 10 studies with 995 patients were included in our meta-analysis (Supplementary Fig. S2). 17 –26 Six studies were comparisons between laparoscopic simple prostatectomy (LSP) and OSP, whereas four were comparisons between robot-assisted simple prostatectomy (RASP) and OSP. In addition, a retrospective study was excluded because of the inability to determine the prostate volume of the study patients. 27 Table 1 provides the basic characteristics and quality evaluation of the included studies.
Basic Features and Quality Assessments of the Included Studies
The data are converted to mean ± standard deviation.
CT = catheterization time; EBL = estimated blood loss; IPSS = International Prostate Symptom Score; IT = irrigation time; LOS = length of hospital stay; LSP = laparoscopic simple prostatectomy; MISP = minimally invasive simple prostatectomy; NR = not reported; OSP = open simple prostatectomy; OT = operative time; Q max = maximum urinary flow rate; PVR = postvoid residual urine volume; QoL = quality of life; RASP = robot-assisted simple prostatectomy; TR = transfusion rate.
Postoperative efficacy
As given in Table 2, there were no significant differences between MISP and OSP regarding postoperative IPSS (WMD = −0.36; 95% CI = −0.99 to 0.27; p = 0.26), QoL (WMD = −0.22; 95% CI = −0.44 to 0.00; p = 0.05), Q max (WMD = 0.46; 95% CI = −1.37 to 2.30; p = 0.62), and PVR (WMD = −2.14; 95% CI = −11.37 to 7.08; p = 0.65).
Overall Analysis of Postoperative Efficiency Parameters Comparing Minimally Invasive Simple Prostatectomy and Open Simple Prostatectomy
CI = confidence interval; WMD = weighted average difference.
Perioperative outcomes
Operative time
In the meta-analysis, 10 studies involving 995 patients reported the OT data. 17 –26 The MISP group had a longer OT than the OSP group (WMD = 43.07; 95% CI = 31.46–54.68; p < 0.001). In addition, we did a subgroup analysis of patients treated with LSP and RASP for large prostates. The subgroup analysis indicated that compared with the OSP group, the LSP group had obvious statistical significance (WMD = 34.50; 95% CI = 21.85–47.15; p < 0.001), and a similar result was observed in the RASP group (WMD = 57.78; 95% CI = 42.23–73.32; p < 0.001; Fig. 1).

Forest plot and meta-analysis of operative time between MISP and OSP. CI = confidence interval; LSP = laparoscopic simple prostatectomy; MISP = minimally invasive simple prostatectomy; OSP = open simple prostatectomy; RASP = robot-assisted simple prostatectomy; SD = standard deviation.
Estimated blood loss
The EBL data were extracted from 9 studies, 17,18,20 –26 totaling 715 patients (MISP = 343 vs OSP = 372). The combined results showed that the difference in EBL was statistically significant between MISP and OSP (WMD = −292.22; 95% CI = −373.73 to −210.70; p < 0.001; Fig. 2). Furthermore, the subgroup analysis revealed that both LSP and RASP can significantly reduce EBL compared with OSP (LSP: WMD = −288.26, 95% CI = −397.96 to −178.55, p < 0.001; RASP: WMD = −305.08, 95% CI = −447.13 to −163.03, p < 0.0001).
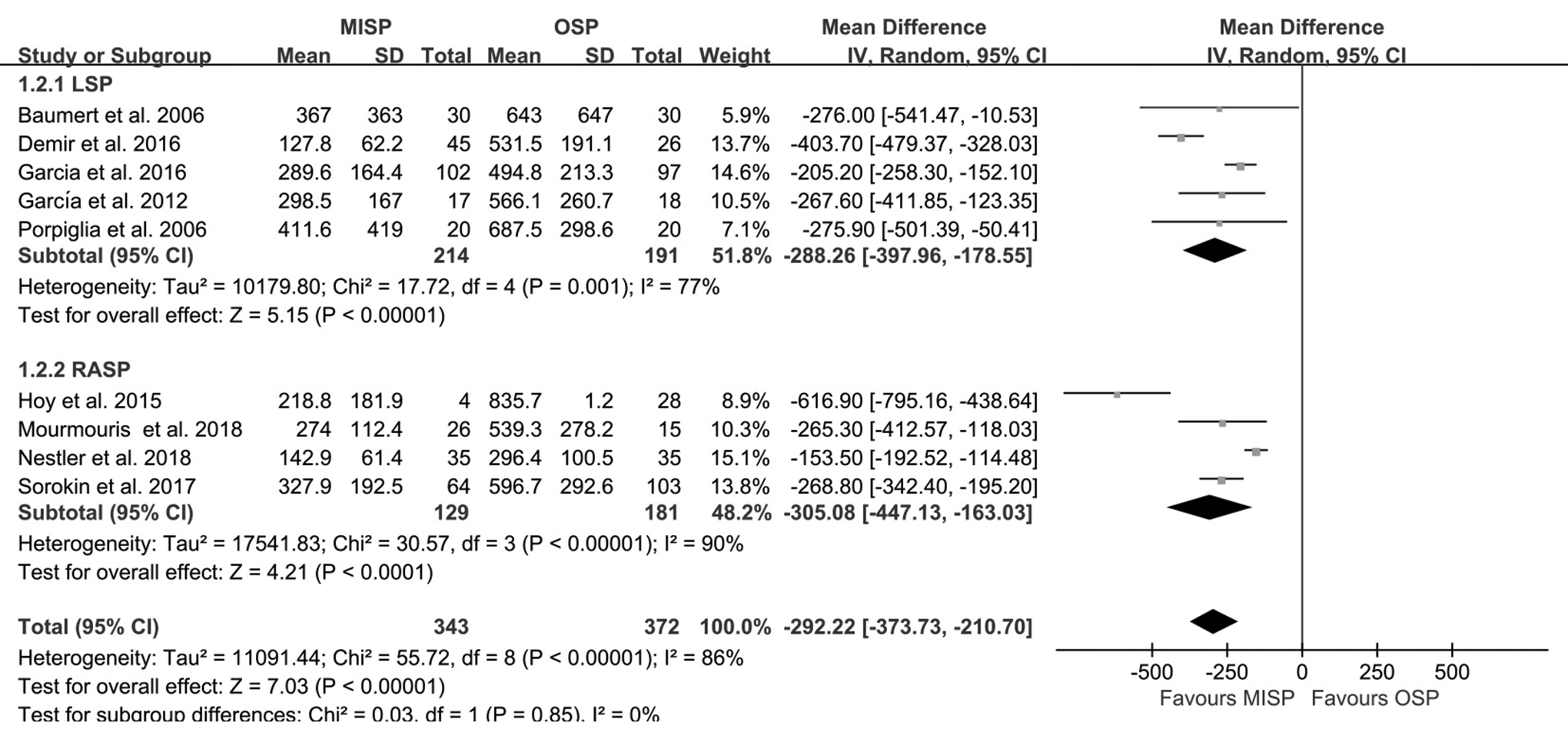
Forest plot and meta-analysis of estimated blood loss between MISP and OSP.
Irrigation time
Five studies were analyzed, 17,19,20,22,25 including 796 patients. Of these, 371 underwent MISP and 425 OSP, and there was no significant difference in IT between the groups (WMD = −1.52; 95% CI = −3.11 to 0.06; p = 0.06; Fig. 3).
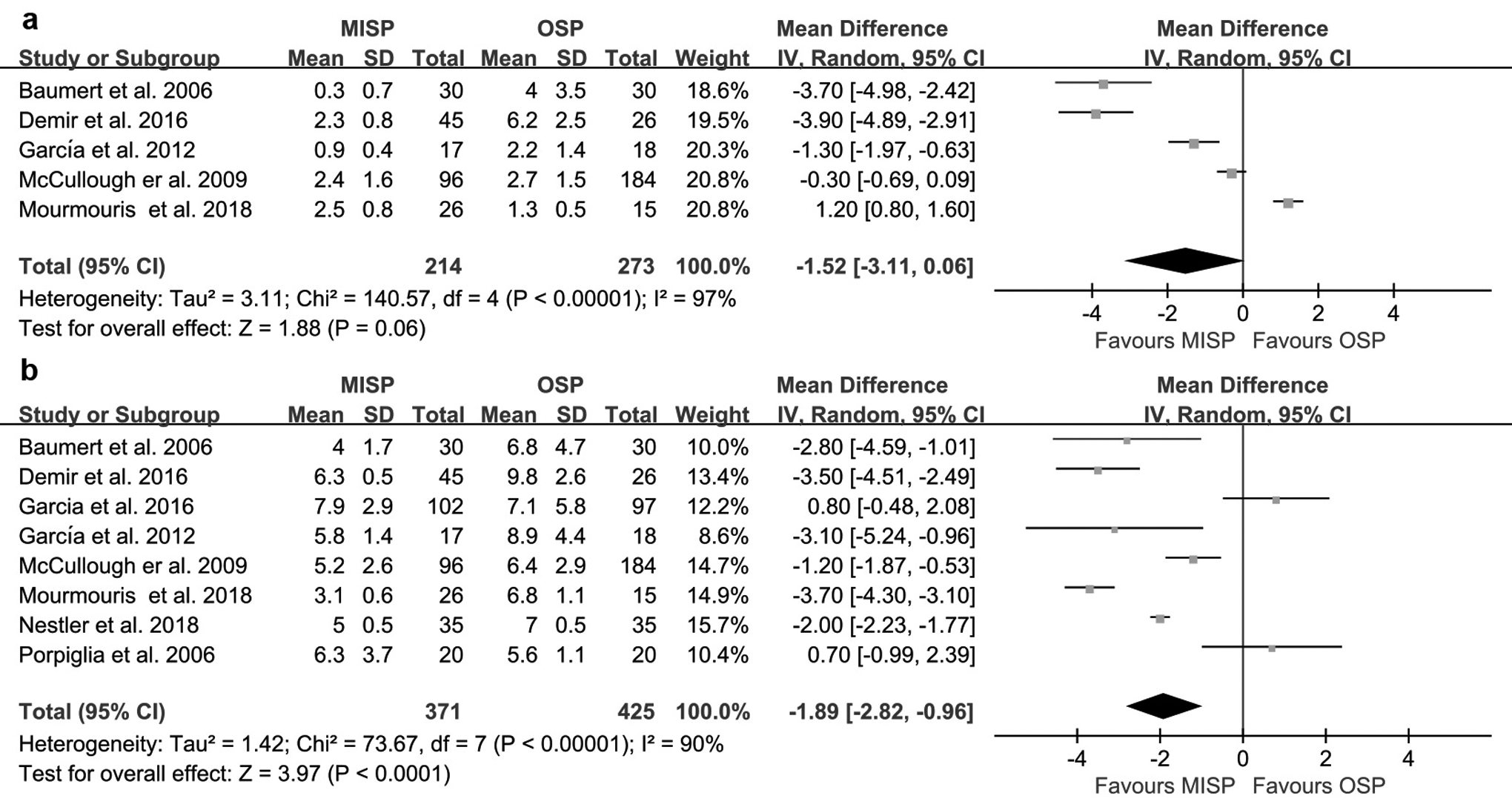
Forest plot and meta-analysis of perioperative variables between MISP and OSP.
Catheterization time
Data on CT were recorded in 8 studies involving 796 patients. 17 –20,22,23,25,26 The merged results represented that MISP had a shorter postoperative CT compared with OSP (WMD = −1.89; 95% CI = −2.82 to −0.96; p < 0.0001; Fig. 3).
Length of hospital stay
Ten studies reported the LOS. 17,18,20 –26 Patients treated with MISP have lower LOS (WMD = −2.52; 95% CI = −3.42 to −1.62; p < 0.001; Fig. 4), and the subgroup analysis also indicated that LOS with either LSP or RASP were less than OSP (LSP: WMD = −2.05, 95% CI = −3.11 to −0.99; p = 0.0002; RSAP: WMD = −3.05, 95% CI = −4.58 to −1.53; p < 0.0001).
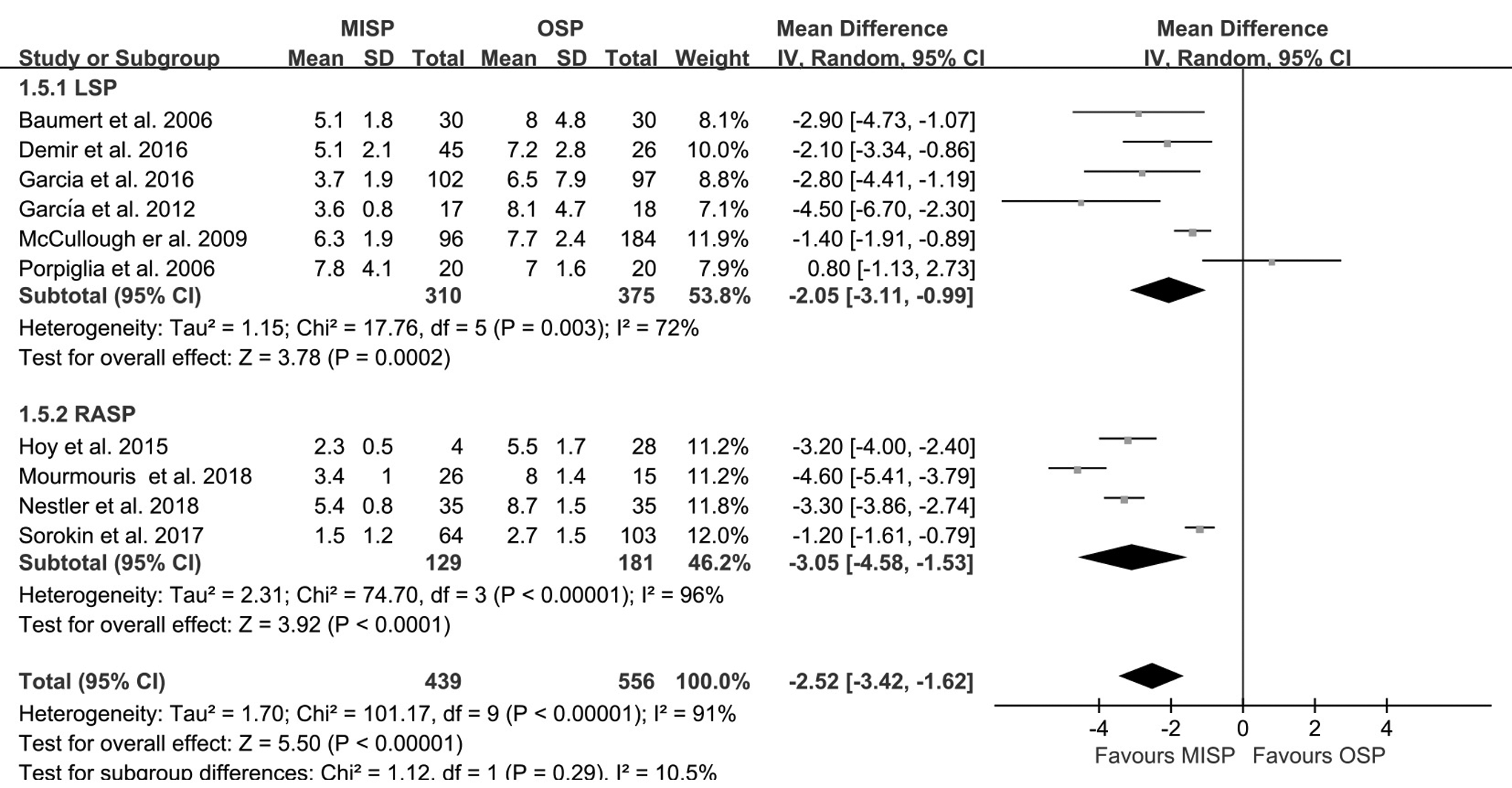
Forest plot and meta-analysis of length of hospital stay between MISP and OSP.
Complications
TR was discovered in nine studies. 17,18,20 –26 The pooled analysis indicated that compared with the OSP, the MISP had a significantly lower TR (OR = 0.21; 95% CI = 0.13–0.36; p < 0.001; Fig. 5). In addition, the subgroup analysis showed that the TR of both LSP (OR = 0.22; 95% CI = 0.12–0.41; p < 0.001) and RASP (OR = 0.21; 95% CI = 0.08–0.52; p = 0.0009) were lesser than that of OSP.
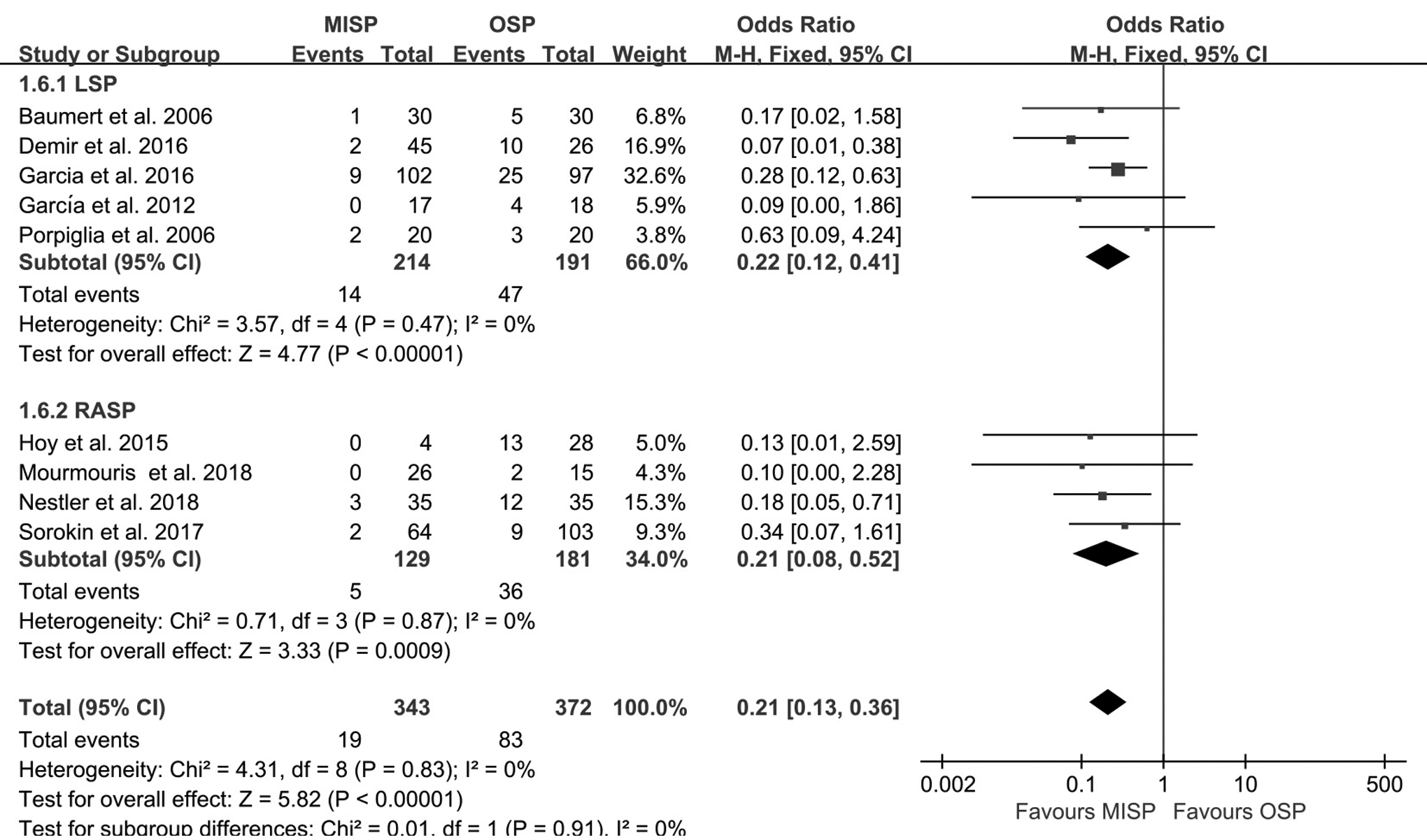
Forest plot and meta-analysis of transfusion rate between MISP and OSP.
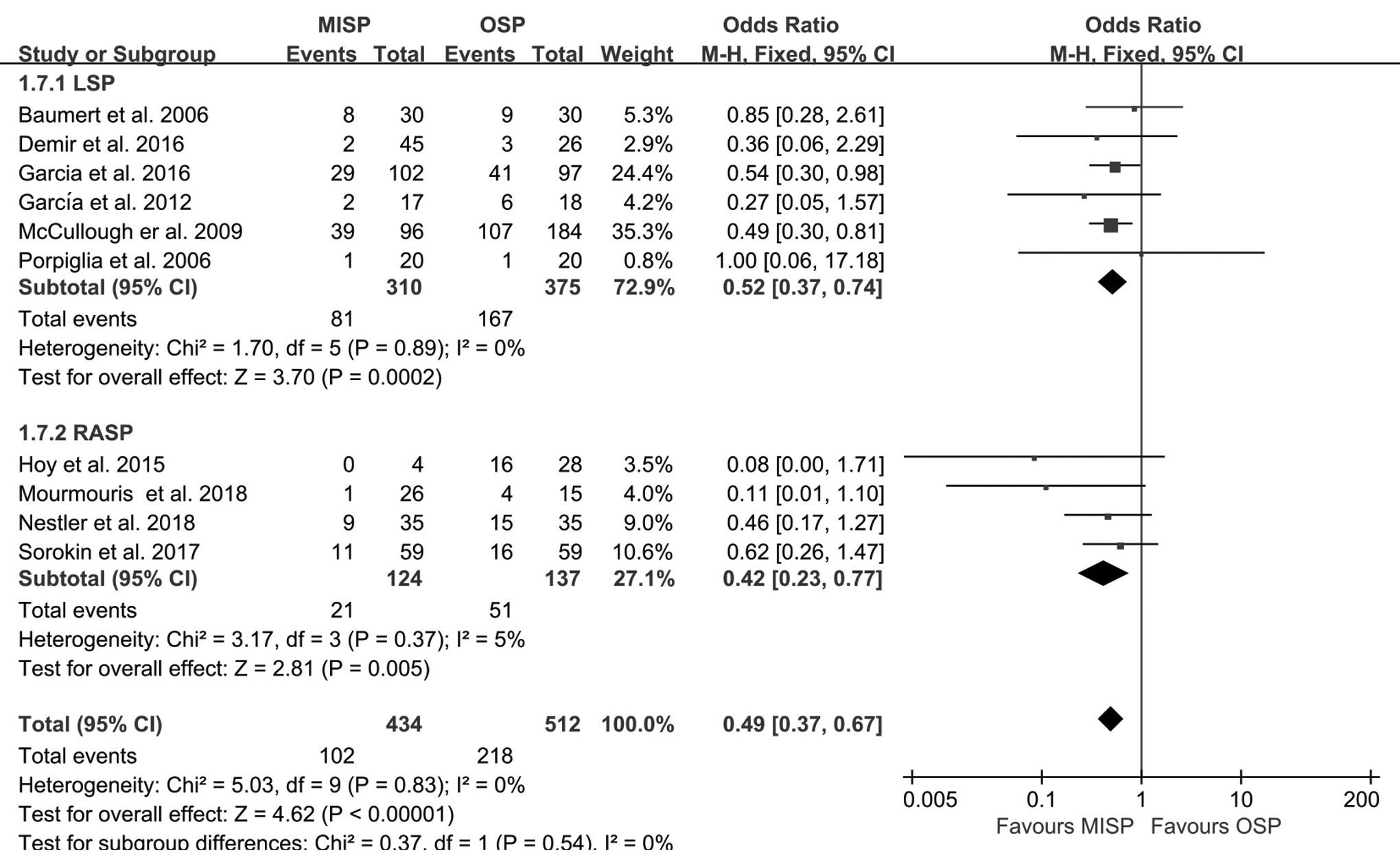
In the final statistical analysis, 10 studies documented overall complications. 17 –26 The incidence of complications for the MISP group was significantly lower than for the OSP group (OR = 0.49; 95% CI = 0.37–0.67; p < 0.001; Fig. 6). Our subgroup analysis demonstrated that the number of complications in the LSP group was less than that in the OSP group (OR = 0.52; 95% CI = 0.37–0.74; p = 0.002), and the RASP group had the same result (OR = 0.42; 95% CI = 0.23–0.77; p = 0.005).
Forest plot and meta-analysis of complications between MISP and OSP.
Discussion
Although transurethral resection of the prostate remains the “gold standard” for the treatment of moderate to severe lower urinary tract symptoms, 28 it is usually associated with bleeding and transurethral resection syndrome, and its efficacy decreases in large prostates. 29 Because of these known shortcomings, urologists have explored a variety of minimally invasive surgical procedures. HoLEP has been described as a “size-independent” treatment for BPH with excellent long-term efficacy. 5,6,30,31 However, its steep learning curve is a major obstacle to the widespread implementation of this procedure. 7 MISP, a promising surgical technique, has attracted the attention of urologists. Several studies have shown the significant advantages of MISP in treating large prostates, such as less bleeding and lower surgical morbidity. 32 However, when compared with traditional OSP, its effectiveness and safety in large prostates remain controversial.
Ten studies were included in our analysis, and perioperative outcomes, postoperative efficacy, and complications were appraised carefully. Moreover, we performed a subgroup analysis to detect the possible differences between LSP and RASP. The present data suggest that MISP has the same efficacy and provides some advantages including reduced blood loss, decreased CT, shorter hospital stays, and a lower transfusion and complication rate but with longer OT.
This meta-analysis showed MISP was not significantly different from OSP in terms of postoperative efficacy (IPSS, QoL, Q max, and PVR). Professor Demir and his colleagues noticed no differences in IPSS (p = 0.76), QoL (p = 0.06), and PVR (p = 0.92) between the LSP and OSP groups during a 3-month follow-up. 22 Later, Sorokin and associates 24 also confirmed in their study that the difference in postoperative efficacy after the two surgical methods (RASP vs OSP) was not obvious (IPSS: p = 0.884, QoL: p = 0.601, Q max: p = 0.36, PVR: p = 0.007). In addition, one study had a postoperative PSA comparison analysis between RASP and OSP. They found that there was no significant difference between the groups (0.78 vs 0.64, p = 0.12). 25 However, randomized controlled trials with longer follow-up periods are still needed to confirm our findings.
Our analysis displayed that compared with OSP, MISP significantly increased the OT, and in subgroup analysis, both LSP and RASP had the same results. However, the OT of RASP seems to be longer than LSP. A retrospective study described the comparison of the OT of RASP and LSP, and they found that RASP OT was longer than LSP (p = 0.01; OR = 0.99; 95% CI = 0.9–1.0). 33 It is worth mentioning that there was no difference in the weight of the surgically removed prostate (p = 0.81), which eliminated the impact of prostate volume. However, we are currently unable to assess the clinician's experience and the impact of intraoperative peritoneal adhesions on the duration of operation. Furthermore, the operating time seems to be related to the surgeon's technical proficiency, and robot-assisted therapy as a new technology, less used by urologists, may extend the OT. 34
As one of the indicators to measure the pros and cons of surgical methods, blood loss has always been the focus of clinicians. The EBL of MISP was lower than that of OSP in our meta-analysis, and the results of the comparison between MISP and OSP in the nine studies we included and the unincorporated studies were consistent. 11,17,18,20 –26 Both the laparoscopy and robot vision imaging systems can amplify the surgical field of view, allowing the urologist to carefully observe the blood vessels entering the proliferating prostate tissue under direct vision and detect the bleeding point in time, and then stop the blood by electrocoagulation forceps, thus effectively reducing bleeding from operation. 25 Sotelo et al. and Mariano et al. believed that there was a learning curve for MISP. 35,36 With the experience of the surgeon and the advancement of technology, the operation time can be significantly shortened, and the intraoperative EBL can be significantly curtailed. Because of the limitations of the study, we are unable to assess whether other factors influence the EBL of the operation.
Limited researches reported IT, and combined with the current meta-analysis, we still cannot consider that MISP's IT is lower than OSP. In addition, we also found that MISP has a lower CT than OSP. The results of two recent studies 25,26 supported and strengthened the level of evidence in our research, making our conclusions more reliable. However, an earlier study had the opposite result, and they affirmed that the CT of OSP was lower than MISP. 23 We read the relevant articles and ascertained that the extubation standards were different between the studies, which may affect our results. Furthermore, we found that MISP (LSP and RASP) can significantly reduce the LOS, which is highly consistent with a considerable number of studies. 11 But the earliest study showed no overt difference in LOS between the two groups (LSP vs OSP). 18 We found that the patient's own condition (such as economic status and mental factors), intraoperative blood loss, and postoperative CT will affect the LOS.
We executed a meta-analysis of the overall complications between MISP (LSP and RASP) and OSP. The results indicated that LSP and RASP can effectively reduce the occurrence of complications, and hematoma, urinary retention, and urinary tract infections are the most common complications. 6,19 In addition, we also compared the TR of the two procedures (MISP vs OSP). When compared with OSP, MISP had a lower TR, and our comparison results were similar to the previous studies. However, Sorokin and colleagues found no difference in TRs between RSAP and OSP (3.1% vs 8.7%, p = 0.207), and the differences between the studies may be related to the institution's blood transfusion guidelines, doctor's experience, and patient comorbidities.
One of the main reasons for opposing the implementation of MISP is cost. In our analysis, only one study compared the costs of the two groups (LSP vs OSP). They noted that the average operation cost of the LSP group was higher than the OSP group ($396.62 vs 344.23, p = 0.001). 22 Sutherland and colleagues also found that the cost of RASP was twice that of OSP ($5212 vs $2415). 37 However, RASP has the advantage over OSP in terms of cost (€3840 vs €5400), according to Matei and colleagues. 38 As they described, longer LOS and higher TR can further increase the cost of OSP patients. In addition, the cost of HoLEP seems to be cheaper than MISP. In the study by Salonia and co-workers, 6 the average cost of HoLEP was €2356. Unfortunately, the cost comparison analysis of the two technologies has not been reported. Cost–benefit analysis is a complex problem affected by multiple factors, and large-scale, well-designed studies are needed before a clear conclusion can be drawn. 25
Our meta-analysis also has certain constraints. The sample size of the included studies was small (only 995 cases). Postoperative safety indicators (such as OT, EBL, IT, CT, and LOS) are more heterogeneous. Subgroup analysis explained partial heterogeneity, but other factors affecting heterogeneity have not been evaluated. There are too few studies on reporting performance pointers that may have an impact on our results. In addition, most of the studies we included were retrospective, with choice and distribution and blindness bias. Despite this, our meta-analysis has a high level of evidence. The number of studies included was large, most of which was published in the past 5 years, and the analysis of outcome indicators was comprehensive, which significantly improved the credibility of our results.
Conclusions
The present meta-analysis suggests that MISP is a viable and effective alternative to OSP. It provides similar functional outcomes and has significant advantages in EBL, CT, LOS, TR, and complication rate. Nevertheless, more prospective randomized controlled trials with multicenter and large sample size are needed to confirm our findings.
Footnotes
Acknowledgment
The authors thank Ms. Mengqi Chen for her support in our article.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.