
Abstract
Purpose:
Photoselective vaporization of the prostate (PVP) with a 940-nm diode laser is an option for treating symptoms caused by benign prostatic hyperplasia (BPH). Here, we present our experience using this technology.
Methods:
We prospectively evaluated 126 patients with lower urinary tract symptoms (LUTS) secondary to BPH who underwent PVP with a 940-nm diode laser from January 2011 to January 2014. The patients were assessed using the International Prostate Symptom Score (IPSS), quality of life (QoL) score, prostate-specific antigen (PSA) level, maximum urinary flow (Qmax) by uroflowmetry, postvoid residual volume, and prostate volume by ultrasound at baseline and 3, 6, 12, and 24 months after the procedure.
Results:
The average patient age was 68.8 ± 8.7 years (range 48–90 years), whereas the average preoperative parameters were as follows: IPSS, 26.1 ± 5.2; IPSS-QoL, 4.9 ± 0.8; Qmax, 4.5 ± 3.1 mL/s; prostate volume, 76.5 ± 35.5 mL; and PSA level, 3.9 ± 2.6 ng/mL. The average catheterization time was 24.7 ± 25.5 hours (range 3–120 hours), and the length of hospital stay was 22.4 ± 17.0 hours (range 8–144 hours). The mean follow-up duration was 17.9 months (range 1–36 months). All parameters showed significant improvement after 12 months. After 24 months, the IPSS (8.8 ± 5.4, p < 0.07), IPSS-QoL (1.6 ± 0.9, p < 0.13), Qmax (15.9 ± 7.3 mL/s, p < 0.11), and PSA level (1.2 ± 0.8 ng/mL, p < 0.11) were improved compared with the baseline, but the difference was not significant, probably due to the small number of patients evaluated in this period. No patients required a transfusion.
Conclusions:
The results suggest that PVP with a 940-nm diode laser is safe, effective, and durable for the treatment of LUTS secondary to BPH. The patients continue to be monitored for evaluation of the long-term results. A prospective randomized study would allow more solid conclusions regarding the technology to be reached.
Introduction
Benign prostatic hyperplasia (BPH) is one of the most prevalent diseases in men older than 50 years, affecting 50% of men aged 51 to 60 years and over 80% of men older than 80 years. Obstructive lower urinary tract symptoms (LUTS) caused by BPH directly influence the quality of life (QoL) of patients in terms of both physical and psychological aspects of health. 1
Due to the high prevalence of BPH and its impact on the QoL of patients, much has been carried out to treat BPH. Current therapeutic options include drug therapy and surgical procedures. Transurethral resection of the prostate (TURP) has existed for over 50 years, and it is still considered the gold standard for the surgical treatment of small or moderate BPH. 2,3 However, even minimally invasive procedures are not completely free from morbidity. In the last two decades, laser-based procedures for prostate hyperplasia have gained importance, as technological advances continue to be stimulated by the necessity to attend to aging populations with more comorbidities and reduce the complications of TURP (e.g., retrograde ejaculation, bleeding, and water intoxication). 4,5 In 1992, Costello and colleagues 6 reported the first cases of BPH treated with a laser, in which a neodymium:yttrium aluminium garnet (Nd:YAG) laser was used. Since then, the technology has been improved; currently, various types of lasers are available, with the most widespread being holmium:yttrium aluminium garnet (Ho:YAG), thulium:yttrium aluminium garnet (Tm:YAG), titanyl potassium phosphate (KTP), and diode lasers. While Ho:YAG, Tm:YAG, and KTP lasers use crystals to generate radiation, diode lasers use semiconductors that produce light at a wavelength ranging from 375 to 1800 nm.
The main advantage of the diode lasers is the exact wavelength, which offers high simultaneous absorption by water and hemoglobin, thus combining efficient vaporization of the prostate with haemostasis. 7 In contrast, the KTP laser is strongly absorbed by hemoglobin, which is good for hemostasis, but a long operative duration is required. 8 –10 The Ho:YAG laser is superior in terms of cutting capability due to the high absorption coefficient of water, but holmium laser enucleation of the prostate requires a highly skilled operator. 11 Therefore, diode laser vaporization shortens the duration of the operation, increasing the efficiency. 12
Several studies have shown comparable clinical results with photoselective vaporization of the prostate (PVP), but with shorter term catheterization, a shorter hospital stay, and a lower risk of bleeding. 13 –15 To date, few prospective randomized trials have been published and have had short follow-up periods; thus, the evidence regarding laser surgery for BPH is limited. 16
In this article, we present our experience with 940-nm diode laser PVP after 126 cases and 24 months of follow-up.
Patients and Methods
Study population
We prospectively included 126 patients who were treated with 940-nm diode laser PVP between January 2011 and January 2014.
The surgical indications were in accordance with the BPH guidelines of the American Urological Association: persistent moderate-to-severe LUTS despite prior medication and/or surgery, refractory urinary retention, persistent gross hematuria (CT urography and cystoscopy normal), bladder stones, and recurrent urinary tract infections (UTIs). 17 The use of anticoagulants or antiplatelet therapy and indwelling urinary catheters for urinary retention was not a criterion for exclusion. 18 Patients with a history of neurogenic voiding dysfunction, urethral stricture, bladder neck stenosis, and prostate and/or bladder cancer were excluded from the study.
Surgical technique
All procedures were performed by a single surgeon (J.P.M.), with extensive experience in PVP, under general or spinal anesthesia. Laser vaporization was performed using a 940-nm diode laser (Dornier Medilas D UroBeam; Dornier MedTech, Wessling, Germany). A 70-degree side-firing laser fiber (Dornier Side Fibre Focus) was introduced through a 26F continuous-flow Olympus laserscope (Olympus, Tokyo, Japan) placed in the prostatic urethra.
The power was usually set to 175 W at first, especially near the bladder neck and sphincter areas, whereas it was increased to 250 W to widen the cavity. When bleeding was observed, the laser beam was directed toward that region to achieve hemostasis. Isotonic saline at room temperature was used as an irrigation solution. 3
At the end of each operation, a Foley catheter between 18F and 22F in size was inserted without irrigation. Bladder irrigation was performed only in cases of significant hematuria. An attempt at catheter removal was planned for ∼8 to 12 hours after the procedure to evaluate spontaneous voiding. If this attempt failed, the patient was re-catheterized, and another attempt was made after 12 hours. All patients received prophylactic antibiotic therapy for 7 days after the operation, with a first-generation cephalosporin
Assessment
The International Prostate Symptom Score (IPSS), QoL score, prostate-specific antigen (PSA) level, postvoid residual (PVR) volume, maximum urinary flow (Qmax) by uroflowmetry, and prostate volume by ultrasonography were assessed at baseline and 3, 6, 12, and 24 months after the surgery.
Moreover, data regarding the spent energy, number of fibers used, operative duration, lasing time, necessity of bladder irrigation, catheterization time, length of hospital stay, and complications were also registered.
Statistical analysis
Continuous variables are presented as the mean ± standard deviation and range; categorical variables are presented as a percentage. Statistical analysis was performed using Microsoft Office Excel 2010 and SPSS version 21.0 (IBM Corp.). Student's t-test was used to statistically compare preoperative and postoperative data, and p < 0.05 was considered to indicate statistical significance.
Results
A total of 126 patients underwent PVP with a UroBeam laser without intraoperative complications.
Patient characteristics
The baseline characteristics of the 126 patients treated with the UroBeam laser are shown in Table 1. Of all patients, 27% had an indwelling urinary catheter before surgery due to urinary retention.
Baseline Patient Characteristics
IPSS = International Prostate Symptom Score; PSA = prostate-specific antigen; PVR = postvoid residual (urine); Qmax = maximum flow rate; QoL = quality of life; SD = standard deviation.
The mean patient age was 68.8 ± 8.7 years (range 48–90 years), and the mean follow-up duration was 17.9 months (range 1–36 months). The preoperative parameters were as follows: IPSS, 26.1 ± 5.2; IPSS-QoL, 4.9 ± 0.8; Qmax, 4.5 ± 3.1 mL/s; prostate volume, 76.5 ± 35.5 mL; and PSA level, 3.9 ± 2.6 ng/mL.
Operative parameters
The operative duration and lasing time were 69.3 ± 30.6 minutes (range 30–160 minutes) and 28.5 ± 15.1 minutes (range 7–80 minutes), respectively. In most procedures, a single laser fiber (1.0 ± 0.2) was used, except in cases in which it was damaged earlier than expected due to technical reasons. Only 31.7% (40) of the patients required bladder irrigation after the surgery, and the mean irrigation time was 6.3 ± 3.0 hours (range 2–12 hours). The catheterization time was 24.7 ± 25.5 hours (range 3–120 hours), and the length of hospital stay was 22.4 ± 17.0 hours (range 8–144 hours). The average energy spent was 325.0 ± 139.3 kJ (range 82–827 kJ), and the energy spent per unit prostate volume was ∼4.5–1.9 kJ/mL (range 1.2–10.4 kJ/mL). The data are summarized in Table 2.
Operative Parameters
Efficacy
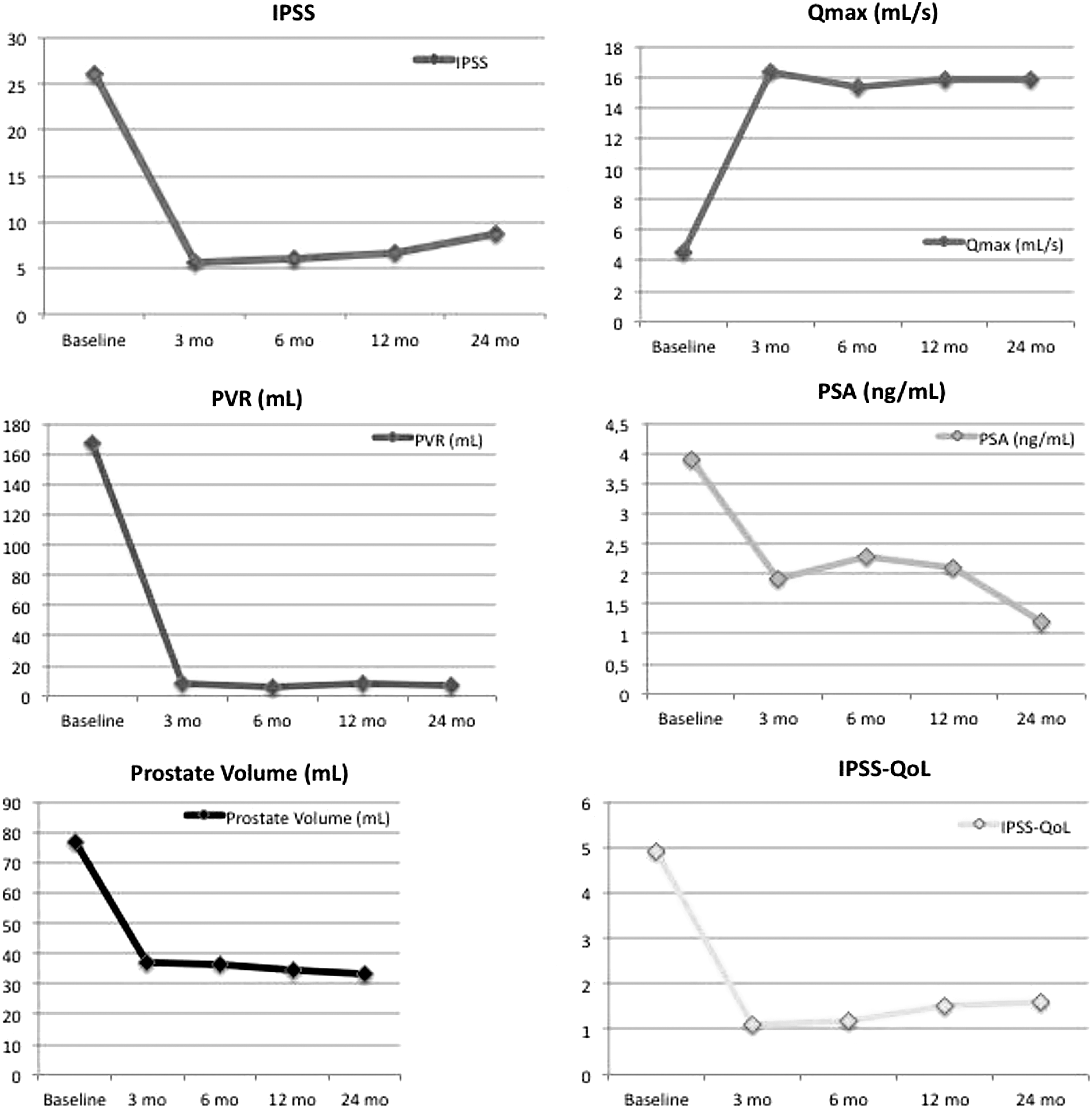
Three months after the operation, all parameters were reassessed, and statistical analysis was performed to compare these data with the baseline data. Significant improvements were observed in the IPSS (5.5 ± 1.4, p < 0.00001), Qmax (16.3 ± 3.2 mL/s, p < 0.00001), PVR volume (8.7 ± 16.0 mL, p = 0.00002), IPSS-QoL (1.1 ± 0.8, p < 0.00001), PSA level (1.9 ± 2.2 ng/mL, p = 0.00002), and prostate volume (37.1 ± 16.5 mL, p < 0.00001). At the 12-month follow-up, the improvements in the IPSS (6.6 ± 3.4, p < 0.00001), Qmax (15.8 ± 4.6 mL/s, p < 0.00001), PVR volume (8.3 ± 16.9 mL, p = 0.0006), IPSS-QoL (1.5 ± 1.7, p = 0.0002), PSA level (2.1 ± 3.2 ng/mL, p = 0.00067), and prostate volume (34.4 ± 19.9 mL, p = 0.00016) persisted.
After 24 months, despite improvements in the IPSS, IPSS-QoL, Qmax, and PSA level, only the prostate volume and PVR volume showed sustained and statistically significant improvements. The functional results are listed in Table 3, and the evolution of the clinical outcome is demonstrated in Figure 1.
Change in functional parameters according to baseline level.
Preoperative and Postoperative Functional Parameters *
Mean ± SD values shown with the number of patients for whom data are available.
p = significance relative to baseline.
Early adverse events
The main early adverse events are shown in Table 4. The rate of rehospitalization within 30 days was 3.17% (four patients): two patients (1.58%) were rehospitalized for immediate retreatment due to urinary retention by residual adenoma, and TURP was performed; one patient (0.79%) was rehospitalized due to urinary retention by stenosis of the urethral meatus, which was treated with surgery (meatoplasty); and one patient was readmitted for the treatment of a severe urinary infection with intravenous antibiotics guided by urine culture. Another 12 patients (9.52%) required emergency hospital care without the need for hospitalization due to UTIs. Nineteen patients (15.07%) showed early urinary retention before hospital discharge and were discharged while using a catheter, which was withdrawn after 4 days. No patients required a blood transfusion or had TURP syndrome.
Prevalence of Surgery-Related Complications Based on the 2004 Clavien–Dindo Classification Before 1 Month Postoperatively
Retention during hospital stay after catheter removal.
NSAIDs = nonsteroidal anti-inflammatory drugs; TURP = transurethral resection of the prostate; UTI = urinary tract infection.
Long-term complications
In the long-term follow-up period, eight patients (6.34%) developed urethral stricture, seven patients (5.55%) developed bladder neck contracture, and six patients (4.76%) developed obstructive symptoms due to residual adenoma and required reoperation after the second year of follow-up. Temporary urinary incontinence occurred in six patients (4.76%), stress urinary incontinence in three patients (2.38%), and urge-incontinence symptoms in four patients (3.17%), and these symptoms were conservatively treated. One patient developed pubic symphysitis that was treated with anti-inflammatory and analgesic drugs. Irritative symptoms did not have a significant impact on QoL. The main long-term complications are summarized in Table 5.
Prevalence of Surgery-Related Complications Based on the 2004 Clavien–Dindo Classification After 1 Month Postoperatively a
After hospital discharge.
Discussion
TURP is still considered by most to be the standard surgical procedure for BPH up to 80 mL. 19 Over the past few years, the number of TURP procedures has slightly decreased despite the fact that the number of surgical treatments remains stable, indicating the replacement of TURP by laser therapies, which already account for ∼50% of all transurethral procedures in the United States. 20
Primary results
In our series, we observed benefits of the laser therapy, including reduced morbidity, with the same functional results as TURP. We highlight the significant improvement in the Qmax, IPSS, and QoL. We also found a significant reduction in the prostate volume (35%) and PSA level (63%). There were no intraoperative complications. No patients required a blood transfusion, and only 30.7% of the patients required postoperative bladder irrigation, thus demonstrating the effectiveness of this type of laser treatment, especially in terms of tissue coagulation.
Although no intraoperative complications were reported, 15.07% of the patients developed acute urinary retention after catheter removal. We observed that 27% of the patients were preoperatively dependent on indwelling catheters due to urinary retention refractory to medical treatment. The presence of detrusor hypocontractility was not evaluated before the procedure, but it is known that the bladder outlet obstruction associated with this condition might be a reason for patients to require catheterization. Considering the postoperative decrease in the prostate volume and improvement in the urinary flow, IPSS, and QoL, we attribute the high rate of acute urinary retention to transitory detrusor hypocontractility or urethral sphincter dysfunction because all catheters were withdrawn after a few days in all patients.
Comparison of outcome between PVP and TURP
TURP is still considered the gold standard for the surgical treatment of BPH because of its long-term effects and low incidence of complications. 19 However, despite recent studies showing a decrease in mortality over the years (0.1%), the morbidity rate is still high (11%). 21 In this sense, laser ablation of the prostate was developed as an effective alternative to reduce the morbidity rate and length of hospital stay.
There have been few comparative studies of 940-nm diode laser treatment and TURP. Razzaghi and colleagues 22 conducted a randomized study involving 115 patients with BPH and performed TURP and treatment with a 940-nm diode laser; the patients were followed for 24 months. The authors demonstrated that the catheterization time and length of hospital stay were greater in the TURP group. Regarding functional outcomes, there was no significant difference in the Qmax, IPSS, or PVR volume between the groups after 6 months. However, after 12 and 24 months, the average IPSS and Qmax were significantly better in the TURP group. No complications were reported in the diode group, whereas in the TURP group, four patients (7.7%) required a transfusion, three patients (5.7%) developed capsule perforation, and two patients (3.8%) developed TURP syndrome.
In our study, functional results comparable to those in the initial TURP series were found for all parameters studied up to 24 months. In addition, the most relevant complications in our study are similar to those found in the TURP series. 23,24
Perioperative bleeding
Perioperative bleeding remains the most common complication of TURP, especially in those patients treated with oral anticoagulation. 18,25 In our study, there were no cases of significant bleeding, and no patients required a transfusion; 35 patients (27.8%) were receiving treatment with antiplatelet agents, and 5 (3.9%) were receiving anticoagulant therapy. Probably, PVP may potentially provide a cost savings for those patients whose suspension of anticoagulants therapy is not recommended. 26
Study limitations
First, the main limitations of the study are the lack of randomization and a direct comparison against TURP as the gold standard. To overcome such failings, larger prospective and randomized studies are considered essential. Second, although in the majority of studies, the follow-up period has been confined to 1 year, this study was conducted for only 2 years. To verify the therapeutic efficacy, a longer postoperative observational period is crucial. Third, the small sample size may have affected the statistical power of our study, limiting the detection of certain differences among the variables studied at the considered follow-up intervals. Finally, in this study, a single surgeon operated on all patients. Data from multicenter studies including more surgeons are needed to generalize the findings of this study.
Conclusions
In conclusion, the findings of this study indicate that PVP with a 940-nm diode laser is a safe and effective procedure with low complication rate. The procedure allows early discharge and has a low rate of postoperative complications. Our patients continue to be followed for evaluation of the long-term results, and we expect randomized prospective studies to allow more solid conclusions regarding the technology to be made.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.