
Abstract
Objectives:
To describe our surgical technique of robotic ureteroileal reimplantation (RUIR) for ureteroileal anastomosis strictures with the use of near-infrared fluorescence imaging (NIFI) after transnephrostomic antegrade injection of indocyanine green in patients previously treated with robot-assisted radical cystectomy and intracorporeal orthotopic neobladder.
Materials and Methods:
From March 2015 to December 2017, 10 consecutive patients underwent RUIR in our tertiary referral center. All patients previously underwent percutaneous nephrostomy and at least one antegrade stenting and stricture dilatation attempt. Clinical data were prospectively collected into our institutional dataset. Both perioperative and functional outcomes were assessed.
Results:
Median time from robotic cystectomy to ureteroileal anastomosis strictures diagnosis was 5 months (interquartile range [IQR] 2–6). Median stricture length was 1.5 cm (IQR 1–2). Median operative time was 140 minutes (IQR 81–155), and median length of stay was 5 days (IQR 3–9). Two patients experienced Clavien grade 2 complications (urinary tract infection requiring antibiotics and blood transfusion, respectively). One patient underwent ileum resection and anastomosis due to bowel perforation (Clavien IIIb). At a median follow-up of 19 months (IQR 14–39), one patient developed a stricture recurrence. No patient developed worsening of renal function (newly onset chronic kidney disease stage 3b-4).
Conclusions:
Robotic reimplantation for ureteroileal anastomosis strictures is a safe and highly effective procedure, with a high success rate and excellent perioperative and functional outcomes. NIFI provides an easy guide to identify and progressively dissect the ureter.
Introduction
Ureteroileal anastomosis strictures (UAS) after urinary diversions occur in 3% to 10% of patients after radical cystectomy (RC). 1 –4 Although endourologic treatment represents a minimally invasive first option in this clinical setting, it has a low success rate if compared with surgical repair, especially when stricture length is longer than 1 cm. 5 Therefore, open surgical ureteroileal reimplantation is the gold standard treatment for UAS, offering excellent success rate. 5 –7 However, it represents a challenging surgical procedure, often to be performed in morbid patients in a challenging surgical scenario, with considerable risks of peri- and postoperative complications such as blood loss and bowel perforation. 6 In the past decade, with the increasing adoption of robotic platform, a few centers reported their initial results regarding robotic management of ureteral reconstruction and UAS strictures in ileal conduits, 8 –11 aiming at reducing morbidity that a conventional open approach could trigger in such situations.
In this scenario, localization of ureteral strictures is critical, as the surgeon must excise the entire ischemic segment of the ureter to minimize the risk of stricture recurrence, while preserving sufficient length of the healthy ureter to realize a tension-free ureteroileal anastomosis.
Being an extremely challenging context, with a considerable rate of potential complications, 8 it was described as the use of near-infrared fluorescence imaging (NIFI) with indocyanine green (ICG) guidance to allow a quicker and safer identification of the ureter. 12 –14
In this study, we described our surgical technique and reported perioperative and functional outcomes of our initial experience with robotic ureteroileal reimplantation (RUIR) for UAS in patients previously treated with robot-assisted radical cystectomy (RARC) and intracorporeal orthotopic neobladder (iON) with the use of NIFI after antegrade transnephrostomic injection of ICG.
Materials and Methods
Inclusion and exclusion criteria
Our institutional review board (IRB) approved RARC database was retrospectively analyzed. Among the 145 patients who underwent RARC with iON, with a minimum follow-up length of 1 year, 10 consecutive patients underwent RUIR for benign strictures in our tertiary referral center, between March 2015 and December 2017. All patients previously underwent RARC-iON with the same standardized technique. 15 The neobladder performed was Padua Ileal Neobladder. Briefly, the main surgical steps of neobladder configuration are: isolation of about 42 to 45 cm of the ileum; detubularization of the right horn (8 cm) and incision of the left horn to insert motorized staplers; configuration of the neobladder neck with motorized titanium staplers (10–12 cm); detubularization of the proximal part of the ileum (24 cm); first folding of the proximal ileal segment, approximating two 8-cm segments that will configure the neobladder dome with the subsequent folding; second folding and configuration of the posterior plate; completion of the posterior plate of the neobladder; and closure of the anterior neobladder wall and final shape of Padua ileal bladder.
Ureters were passed through the posterior aspect of the neobladder and spatulated. The left ureter is not passed behind the sigmoid, but it is left in place, in an orthotopic position. Ureteroileal anastomoses were performed according to the modified split-nipple technique with 4-0 Monocryl interrupted sutures. Guidewires and 6F/7F Double-J stents were inserted through a prepubic miniport trocar. Patients with malignant strictures, evidence of pelvic disease recurrence and patients who had previously undergone open radical cystectomy (ORC) were excluded. The study obtained IRB approval number 1125/18.
Preoperative evaluation
UAS were investigated in all patients reporting urinary tract infections (UTI), renal insufficiency and lumbar pain or radiological evidence of stricture at CT performed during RARC follow-up. Percutaneous nephrostomy, antegrade pyelography, and at least one antegrade stenting and stricture dilatation attempt were performed in all cases (Fig. 1a, b). All patients provided written informed consent to RUIR. In addition, all patients understood that although the adverse effect profile of intravenous ICG is favorable, the adverse effect profile of intraureteral ICG has not yet been completely elucidated. Baseline, perioperative, and follow-up data were reported.

Surgical technique
All the procedures were performed by using Da Vinci Si Surgical System (Intuitive Surgical, Sunnyvale, CA) by two surgeons (G.S. and M.G.) in a four-arm configuration with a transperitoneal approach, with the patient in a steep Trendelenburg position. Trocars ports were placed as previously described for our Padua iON technique. 15
ICG was prepared on receipt in the operating room by dissolving 25 mg of sterile ICG (Akorn, Inc., Lake Forest) in 10 mL of distilled water.
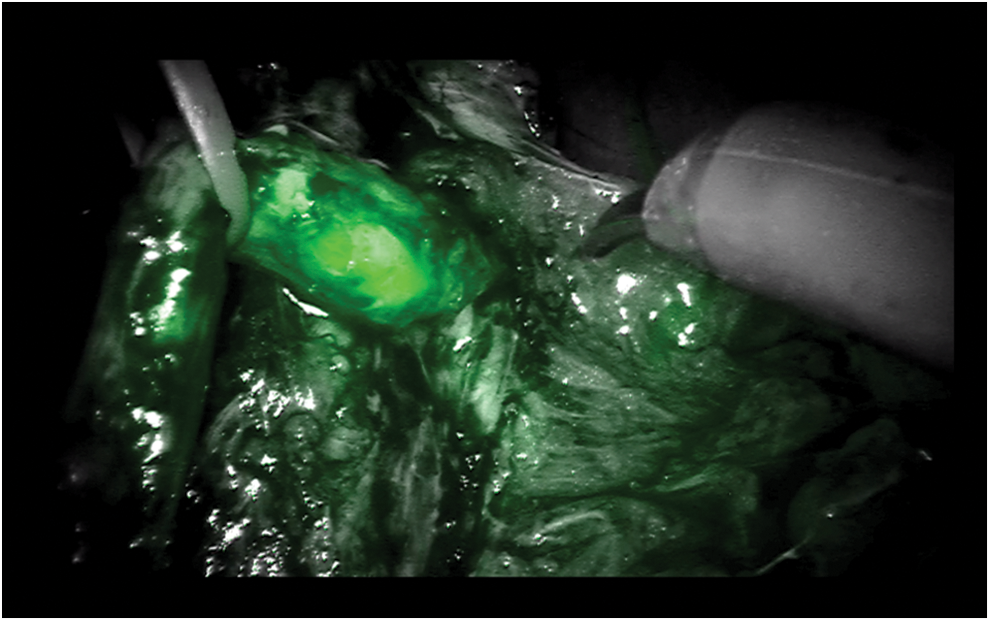
The main surgical steps were: - transnephrostomic injection of ICG to identify the lombar ureter with NIFI; - careful ureteral dissection on the surface of the ureter/s with alternate use of conventional imaging and NIFI (Fig. 2); once the ureter was isolated, a vessel loop was placed, to minimize ureteral manipulation and to attempt a “no-touch” technique (Fig. 3); when approaching the iliac crossing, intravenous ICG was administered to enhance visualization of iliac vessels; - localization of uretero-enteric anastomosis, identifying the stenotic tract, with a typical aspect of a white, thinner, and ischemic tissue (Fig. 4). Through ICG guidance, resection of the ureter was performed proximally to the stenosis; - spatulation of the ureter; - retrograde insertion of a Double-J stent and, eventually, uretero-neobladder anastomosis.
At the end of the procedure, two drains were left in place.

Alternate use of conventional imaging and NIFI for lumbar ureter identification. NIFI = near-infrared fluorescence imaging.
Vessel loop adoption to minimize ureteral manipulation during the dissection (“no-touch” technique).
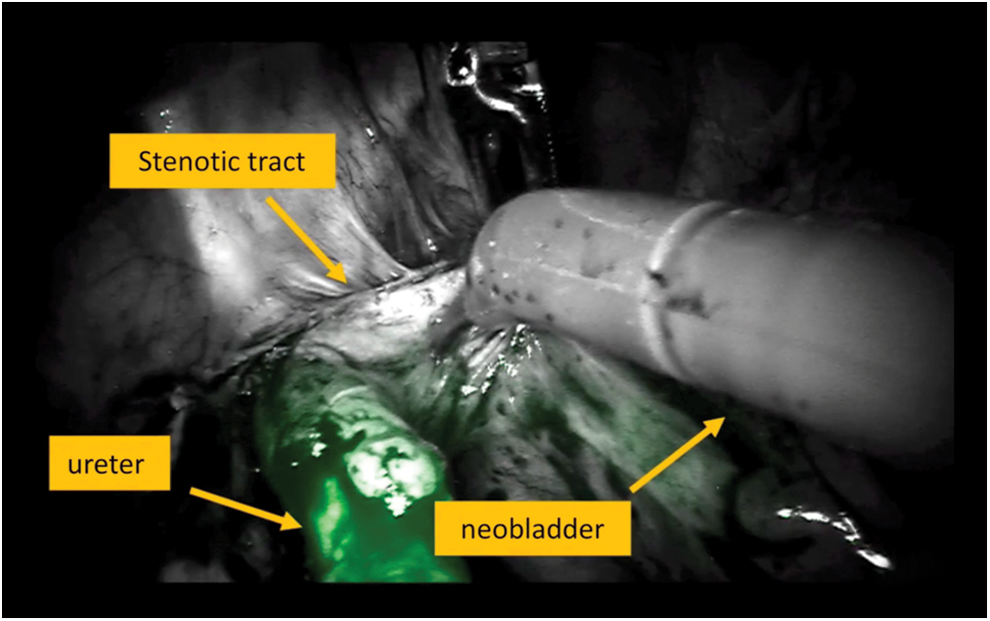
Localization of uretero-enteric anastomosis (through ICG antegrade injection), with identification of the stenotic tract and the neobladder wall. ICG = indocyanine green.
Postoperative management and follow-up
Deep vein thrombosis and antibiotic prophylaxis, with early ambulation, were pursued. The drains were removed when the 24-hour output was lower than 100 mL. Patients were usually discharged the day after flatus recovery.
Nephrostomy tubes were removed at the second post-op day, in the absence of clinical symptoms. Stents were removed at 12 weeks postoperatively. Patients were assessed postoperatively for clinical absence of suspect attributable to stricture recurrence and radiological success (absence of a ureteral stricture and/or hydronephrosis on ultrasound and CT-scan, performed 1 week and 1 month after stents removal, respectively). Follow-up visits were scheduled according to bladder cancer follow-up protocol.
Endpoints
Collected demographic parameters were age, gender, body mass index, and the American Society of Anesthesiologists (ASA) score. Clinical variables were stricture side, prior chemo or radiotherapy, time from RARC to stricture diagnosis, and stricture length. Perioperative parameters assessed were operative time, conversion to open surgery, complications according to Clavien-Dindo system, 16 and hospital stay. Clinical and radiological success were evaluated at any follow-up scheduled visit. Last estimated glomerular filtration rate was finally assessed.
Statistical analysis
Descriptive analyses were used. Frequencies and proportions were reported for categorical variables. Medians and interquartile range (IQR) were reported for continuously coded variables.
Results
Baseline clinical characteristics, perioperative and functional outcomes are reported in Table 1. All patients underwent RUIR in Padua iON. Six (60%), 1 (10%), and 3 (30%) patients had left-sided, right-sided, and bilateral strictures, respectively.
Baseline Clinical Characteristics, Perioperative and Functional Outcomes
ASA = American Society of Anesthesiologists; BMI = body mass index; eGFR = estimated glomerular filtration rate; IQR = interquartile range; RARC = robot-assisted radical cystectomy.
Median time from RARC to UAS diagnosis was 5 months (IQR 2–6). Median stricture length was 1.5 cm (IQR 1–2). Median operative time was 140 minutes (IQR 81–155), and median length of stay was 5 days (IQR 3–9).
All cases were completed robotically. Neobladder Boari flap was created in all cases to guarantee a tension-free anastomosis.
Median intraoperative blood loss was 50 mL (IQR 30–150). Two patients experienced Clavien grade 2 complications (UTI requiring antibiotics and blood transfusion, respectively). One patient underwent ileum resection and anastomosis due to bowel perforation (Clavien IIIb). At a median follow-up of 19 months (IQR 14–39), one patient (10%) developed a stricture recurrence. No patient developed worsening of renal function (newly onset chronic kidney disease stage 3b-4).
Discussion
UAS after urinary diversion might be associated with serious sequelae, which might lead to significant renal function deterioration, infectious complications, and the need for additional procedures; the majority of strictures occur within 2 years of surgery, with a median time to diagnosis reported as 7 to 25 months after surgery. 4
The exact etiology is hard to be determined, but it is likely to be a consequence of periureteral fibrosis and scarring secondary to ischemia at the level of anastomotic site, regardless of the anastomotic technique used. 4
The gold standard treatment for UAS is open repair, with a success rate up to 90%, 6 especially in strictures >1 cm, where endourological treatment is effective only in 26% of cases. 5 However, in a large open series with a long follow-up of 47 months, the success rate dropped to 78%. 7
Despite a high success rate, open UAS repair is often challenging and associated with considerable morbidity, due to adhesions from previous cystectomy or radiotherapy-related fibrosis. In a series of 151 open uretero-neobladder reimplantation, Packiam and colleagues reported a 40% overall complication rate, with half of these being related to bowel injury during the ureter identification. 6
The recent increase in the adoption of RARC has given rise to questions about the potential increased risk of developing ureteroileal strictures compared with open series. Anderson and colleagues compared two cohorts of ORC and RARC, failing to detect a statistically significant difference in terms of stenosis occurrence among the two groups (ORC 8.5% vs RARC 12.6%, p = 0.21). 17 This outcome was corroborated by data of a large robotic series, in which Hussein and colleagues analyzed the outcomes of RARC-specific complications in 406 patients treated in their institution between November 2005 and May 2015, reporting a 7.6% rate of UAS at a follow-up of 27 months. 18
In this clinical scenario, the development of UAS after RARC requiring surgical repair has given rise to the interest in surgical procedures aimed at reducing the morbidity of open surgery, with the adoption of the robotic approach to manage distal ureteric strictures. However, due to surgical challenges of this procedure, there are a few existing series, with a low number of cases, mostly selected and focused on ileal conduit diversion. 9 Accordingly, robotic ureteral reimplantation was initially performed for distal ureter pathologic conditions, such as ureteral injury after gynecological surgery or distal ureter malignancies, 8 with excellent outcomes in terms of success rate, even for long lesions requiring the mobilization of the bladder in a cephalad direction, and the performance of a psoas hitch and/or Boari flap. 11 However, despite the minimal invasiveness of the robotic approach, complications rates were not dramatically lower than open series, as expected; as a matter of fact, Musch and colleagues, in their preliminary experience with 16 cases of robotic reimplantantions for various ureteral pathologic conditions, reported an overall 75% 90-day complications rate, 8 and potentially more discouraging outcomes could have been derived in a reoperation setting, such as reimplantation after RC. To minimize challenging intraoperative difficulties regarding ureter identification and isolation from adhesions with the bowel, iliac vessels, or neobladder, we delivered ICG with an antegrade transnephrostomic injection.
ICG has been already widely employed in other urologic procedures, such as the identification of sentinel lymph nodes in prostate cancer, 19 super selective arterial clamping for nephron sparing surgery, 20 and preoperative marking of endophytic renal tumors in robotic partial nephrectomy. 21 As concerns ureteral stricture management, in 2013, Lee and colleagues used ICG in a small series of seven patients with ureteral stenosis requiring ureteroureterostomy, instilling ICG above and below the level of stenosis through a ureteral catheter or a percutaneous nephrostomy tube, or both, aiding the surgeons in discerning a healthy ureter from diseased tissue, with a successful robotic ureteral repair. 12
Later, in 2015, the same group reported a case series of 26 ICG-guided robotic ureteral reconstruction in different clinical settings, including ureterolysis, pyeloplasty, ureteroureterostomy, and ureteroneocystostomy, 13 and more recently, they reported their results of 8 patients (7 ileal conduits) who underwent ICG-guided RUIR, with a 80% success rate at a median follow-up of 29 months. 14
In this article, we report the largest series of RUIR in iON, highlighting the surgical advantages achievable with percutaneous antegrade ICG injection to immediately identify the ureter, precisely locate the stenotic tract, and safely perform a ureteroileal anastomosis.
This approach provided a quick and precise identification of the ureter, enhancing visualization of the dissection plane between the ureter and the iliac vessels. On the other hand, an obvious drawback of this approach is the proper identification of ureteric vascularity through intravenous administration of ICG, a technique emerging as a potential standard during RARC to identify the devascularized distal ureteric segment before performing ureteroileal anastomosis. Therefore, our approach is based on a meticulous identification of the ICG-enhanced ureter, leaving the resection strategy on a conventional white light vision. When looking at the main outcomes of this surgical procedure, this series had excellent results: No patient had vascular injuries, all procedures were successfully completed robotically with creation of a Boari neobladder flap, and only one patient had reintervention due to bowel perforation occurring during the postoperative course. Moreover, at a median follow-up of 19 months, a single recurrence occurred. These data support the limited role of intravenous ICG administration in this surgical setting, probably due to the need to perform an extended resection of the ureter beyond the proximal ischemic tract.
A combined use of transureteric and intravenous ICG delivery is still a viable and reasonable option to identify the ureter, as described earlier, and iliac vessels at the ureteric cross, respectively. This combined use of ICG seems a reasonable balance between the need to overcome potential vascular injuries 10 due to complex identification of iliac vessels without compromising the more difficult surgical step that is certainly the precise and safe ureter isolation from its lumbar tract toward the neobladder. The high success rate and the low complication rate reflect the effectiveness of our surgical technique.
However, our study is not devoid of limitations. First, the small sample size of the cohort and the limited follow-up duration preclude conclusions about the long-term effectiveness of this surgical approach. Also, due to intrinsic complexity of this surgical procedure, its reproducibility must be confirmed in further studies.
Conclusions
RUIR for UAS is a safe and highly effective procedure. NIFI imaging provides an easy guide to promptly identify and progressively dissect the ureter, reducing the risks of intraoperative vascular and bowel injuries. Thanks to the high success rate, to the favorable perioperative course, and to the excellent functional outcomes, ICG-guided RUIR represents a viable treatment option to adopt in patients developing UAS after RARC, when endourologic treatment attempt fails.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.