
Abstract
Objectives:
To report on long-term follow-up and outcomes of infants and small children who have undergone laparoendoscopic single-site (LESS) partial nephrectomy to manage upper urinary tract duplication and fusion anomalies.
Materials and Methods:
A retrospective review was performed evaluating outcomes of pediatric patients who underwent LESS partial nephrectomy for upper urinary tract duplication and fusion anomalies from January 2012 to July 2015, by a single surgeon at a tertiary pediatric referral center. Demographic and perioperative data were reviewed as well as follow-up imaging. Descriptive statistics were used for analysis.
Results:
A total of 18 patients were identified. Additional access was used for two patients to complete the procedure. Median follow-up was 39 months. No short-term complications were encountered. Three patients were noted to have abnormal postoperative ultrasounds: two perinephric fluid collections and one atrophy of the remaining ipsilateral moiety. One fluid collection resolved completely, and the other decreased in size. Complete atrophy of the ipsilateral moiety occurred. No secondary procedures were required.
Conclusions:
LESS partial nephrectomy is safe for renal duplication and fusion anomalies with good long-term outcomes. Although it can be safely performed, it is a technically demanding procedure and has been discontinued in favor of robotic partial nephrectomy.
Introduction
Upper urinary tract duplication anomalies occur in ∼1% of the population and are congenital conditions that may predispose patients to symptoms such as flank pain, incontinence, or infection. 1 Both extirpative and nonextirpative approaches have been safely performed, using conventional laparoscopic surgery and robotic surgery for management of these conditions. 2,3 The application of these minimally invasive surgical techniques in upper urinary tract surgery affords the ability to eliminate previously unavoidable hospital stays and reduce postoperative pain along with narcotic use. 4,5
Ongoing innovation in minimally invasive surgery has focused on further reduction in patient morbidity while preserving outcomes. Laparoendoscopic single-site (LESS) surgery has evolved as a surgical technique to minimize access points in the abdominal wall to reduce port site complications, pain, and improve cosmesis. 6 In short-term follow-up, several pediatric series have demonstrated safety and efficacy using LESS for upper urinary tract surgery; however, outcomes beyond the immediate perioperative period are lacking. 7,8 The aim of this study is to report on long-term follow-up and outcomes of infants and small children who have undergone LESS partial nephrectomy to manage upper urinary tract duplication and fusion anomalies.
Materials and Methods
The medical records for all patients who underwent LESS partial nephrectomy for upper urinary tract duplication and fusion anomalies by a single surgeon at a single pediatric institution were retrospectively reviewed. Procedures were performed from January 2012 to July 2015. Reconstruction with ureteroureterostomy for duplication anomalies was also performed during the study period, based on shared decision making between the family and surgeon, but were excluded from this study. Preoperative renal ultrasounds and nuclear renal scans were performed. Renal scans were not performed if the renal ultrasound unequivocally demonstrated complete loss of renal parenchyma. Axial body imaging, such as CT or MRI, was not routinely performed. No preoperative imaging was performed to define vascular anatomy. Indications for surgery included obstruction of a poorly functioning renal moiety in an upper tract duplication anomaly or failure to involute of a cystic dysplastic moiety in a fusion anomaly. Data collection included demographic information (age, weight, gender, diagnosis, and laterality), perioperative details (operative time, blood loss, length of hospital stay, postoperative analgesics, and complications), follow-up imaging findings, and need for secondary inventions. Descriptive statistics were used for analysis with all continuous variables described as medians.
Surgical technique for LESS partial nephrectomy, including operative equipment and patient positioning, has been previously described. 8 Ureteral catheter placement of the normal ipsilateral moiety was typically performed for intraoperative identification of the normal ureter. The ureteral catheter was removed at the end of the procedure. All procedures were performed through a transperitoneal approach using the umbilicus, with a single vertical umbilical skin and fascia incision. The study was approved by the institutional review board at our institution.
Results
Patient demographic information and perioperative data are presented in Tables 1 and 2. A total of 18 patients underwent LESS partial nephrectomy. Additional access was used for two patients (2/18, 11%) to complete the procedure, because of slow progress and technical challenges with exposure for safe progress. In one case a single additional access site was used, and in the other case two additional access sites were used to convert to conventional laparoscopy.
Patient Demographic Data
Perioperative Data
Figure 1 shows an intraoperative picture of the single-port device in position and a long-term postoperative appearance of the umbilical surgical site. Two patients (2/18, 11%) were lost to follow-up long-term. Figure 2 shows the postoperative appearance of an umbilicus in the long-term follow-up.
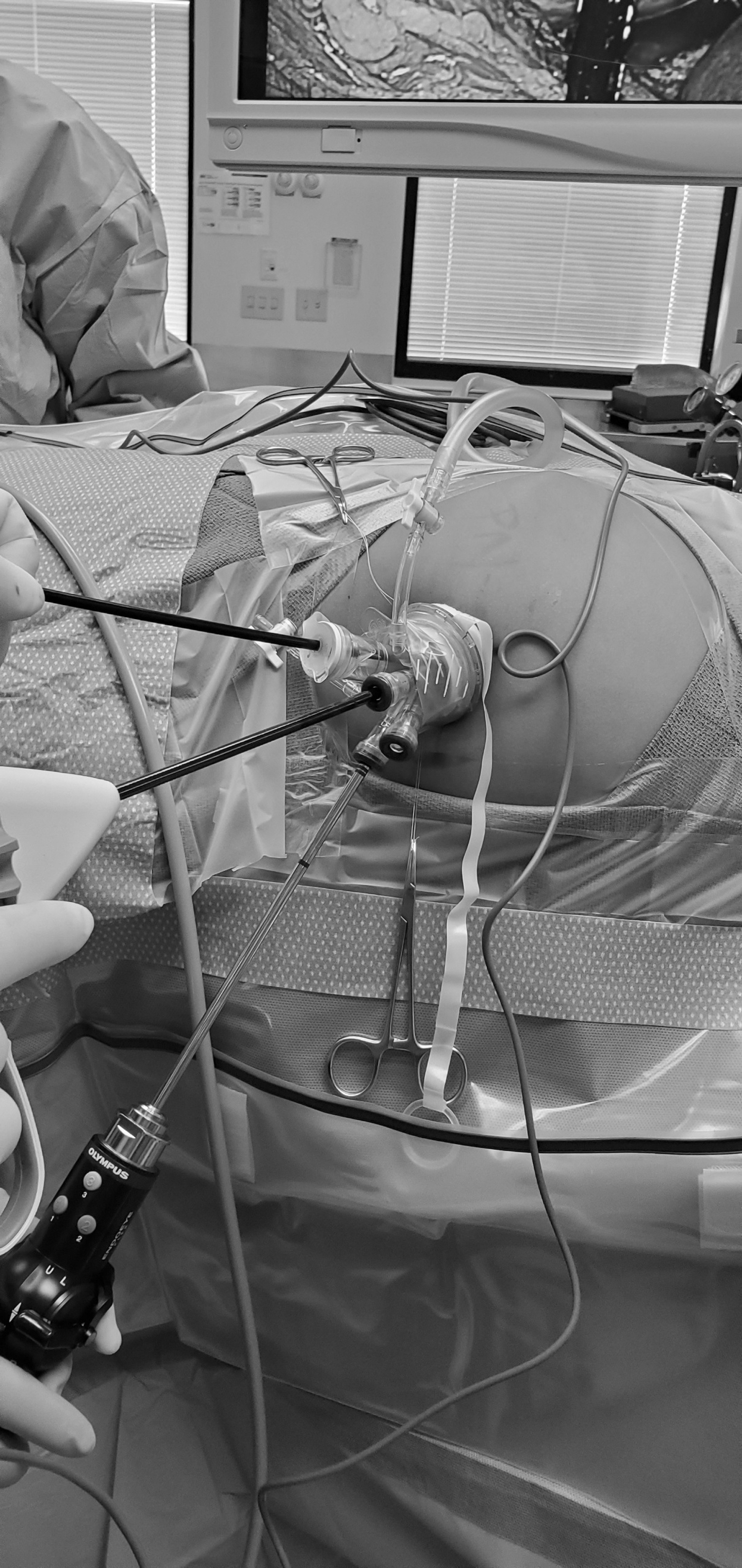
Intraoperative appearance of single-port device positioned in umbilicus.

Long-term postoperative appearance of umbilicus.
The remainder of patients had follow-up extending beyond 1 year after surgery with a median follow-up time of 39 months (range 16–53).
The postoperative visit with an ultrasound was performed after 3 months. No patient had a complication requiring an emergency room visit or an unplanned outpatient visit. Three patients (3/16, 19%) had abnormal postoperative ultrasounds (Table 3). Two patients had perinephric fluid collections and one had eventual complete atrophy of the ipsilateral moiety. The atrophy occurred with the fifth procedure in the experience. Surveillance was utilized for all patients, and none required secondary invasive procedures for management. One perinephric fluid collection resolved spontaneously by 4 months after surgery. The second fluid collection has progressively decreased in size for 3 years. It is asymptomatic and was diagnosed as a dilated calix by radiologists.
Postoperative Imaging Data
The patient with the atrophic ipsilateral moiety was clinically well for >4 years and was discharged from surveillance. Atrophy of the ipsilateral moiety was secondary to an unrecognized vascular anomaly, with one main pedicle that branched into segmental arteries for the upper pole and lower moieties, after reviewing video of the procedure.
Discussion
Laparoscopic extirpative renal surgery was first developed in adults by Clayman et al.. 9 Further developments have been made in minimally invasive surgery and have subsequently been adopted in pediatrics. A wide variety of pediatric urologic procedures are performed with conventional laparoscopy or robotics, for ablative and reconstructive surgery. Advantages of minimally invasive surgery over open surgery have been demonstrated, regarding postoperative pain, length of hospital stay, and cosmesis, without compromising clinical outcomes. 4,5,10
LESS was developed in an attempt to further reduce surgical morbidity and has been utilized in pediatric urology for a variety of procedures. 8,11 –14 In 2009, Park and colleagues initially reported their experience with a homemade single-port device used to perform a nephrectomy in the management of an ectopic ureter for a pediatric patient. 15
Subsequently, other groups also reported LESS nephrectomy and partial nephrectomy can be safely performed in the pediatric population. 8,16,17 However, these series are small having only short-term follow-up. Ham and coworkers reported on six consecutive pediatric patients undergoing LESS nephrectomy and nephroureterectomy. 17 Mean operative times and blood loss were comparable to conventional laparoscopic pediatric nephrectomy series. However, given the size of the specimen, extension of the umbilical incision was required for specimen retrieval, likely reducing the benefit of single-site surgery.
Bansal and associates reported on their early initial experience of LESS used solely for partial nephrectomy. 8 Follow-up was <1 year. Safe and effective outcomes were demonstrated without complications; however, the series included only four patients. The current report includes procedures that required additional access sites, demonstrating the highly technically demanding nature of LESS complex renal procedures.
In pediatric laparoscopic partial nephrectomy literature, there is more robust long-term follow-up data, which is lacking regarding pediatric LESS partial nephrectomy. Esposito et al. reported on 125 children undergoing laparoscopic partial nephrectomy with mean follow-up of 4.2 years. 18 In their series, ∼50% (61/125) of patients developed a cystic structure at the operative site, which has been well described. 19,20 In long-term follow-up, 13/61 (21.3%) resolved at a mean of 4 years, 17/61 (27.8%) decreased in size, 26/61 (42.6%) remained stable, and 5/61 (8.3%) increased in size, with 10/61 (16.4%) associated with infections or pain. 18 Our experience of postoperative fluid collections after LESS partial nephrectomy is well within the reported incidence after pediatric partial nephrectomy.
Functional loss and atrophy of the remaining ipsilateral moiety have been previously described for both open and minimally invasive pediatric partial nephrectomy for duplication anomalies. 19,21 –23 Wallis and associates reported 2/23 (8.7%) patients experienced complete loss of function of the remaining moiety using a retroperitoneoscopic approach, with 1 requiring completion nephrectomy for hypertension almost 3 years after surgery. Both patients were <1 year of age at the time of surgery, and subsequently, at the time of publication, the group was opting to perform open partial nephrectomy for infants.
Jayram and colleagues reported a multinational multicenter experience, of experienced laparoscopic surgeons, showing 7/142 (4.9%) had atrophy or significant loss of function after surgery, with 3 requiring complete nephrectomy. 22 In their experience, learning curve was not felt to be associated with the outcome, and no other factors were consistently identified, although young age, severely dilated moieties, and postoperative complications were postulated as factors.
Our experience of one patient with complete atrophy is consistent with previous rates of atrophy and functional loss after pediatric laparoscopic and retroperitoneoscopic partial nephrectomy for duplication anomalies. In our case, a rare vascular anomaly was not clearly defined during the surgical dissection, and additional exposure of the lower pole hilum would have helped prevent vascular compromise of the healthy moiety. The challenges of dissection utilizing the LESS approach were a factor in this case and may have been avoided. Robotic surgery may be a superior approach regarding atrophy and functional loss, as recent reports have demonstrated excellent outcomes with healthy moieties after partial nephrectomy. 5,24 –26
To our knowledge, Herz et al. reported the one case of a vascular injury of an upper pole during a pediatric robotic lower pole partial nephrectomy, in their series of 20 pediatric robotic heminephrectomies and other robotic procedures for duplication anomalies. 27
To the best of our knowledge, we present the largest series of LESS partial nephrectomy with long-term follow-up in infants and small children for upper urinary tract duplication and fusion anomalies. Our data demonstrate comparable perioperative outcomes regarding operative times, blood loss, length of stay, short-term safety, and long-term outcomes, to other pediatric laparoscopic partial nephrectomy series. Unique to this report, we provide long-term follow-up for patients undergoing LESS partial nephrectomy.
LESS partial nephrectomy can be safely performed, but is more technically challenging than conventional laparoscopy or robotic surgery. LESS procedures are particularly challenging with the limited space outside of the single-port device for the camera driver, especially with an inexperienced assistant, and the surgeon manipulating instruments often requiring exaggerated movements when crossing instruments to perform the procedure. Difficulty with good observation because of camera driving can be extremely frustrating.
With the evolution of surgical practice in urology heavily incorporating robotic technology, we strongly believe robotic surgery has advantages over conventional laparoscopy for partial nephrectomy, especially when partial nephrectomy for duplication is not a common procedure and many U.S. urology residents do not get exposure to conventional laparoscopy for complex procedures during training.
Although safely performed in this study, there is the potential that the results of LESS partial nephrectomy may not be consistently reproducible. A benefit of this study is to report an evolution of surgical practice. Often, initial early experience reports are published stating additional long-term data should be reported to define the role of new procedures, without such data being published. This study helps fill a void of long-term data by providing published data regarding the role of LESS partial nephrectomy.
Because of the technical challenges of LESS partial nephrectomy, relative infrequent occurrence of ablative procedures for duplication anomalies, and the concern about teaching pediatric urology fellows techniques and procedures that are reproducible and will be adopted in practice, the primary surgeon has subsequently transitioned away from LESS partial nephrectomy to robotic partial nephrectomy, with the goal of teaching a procedure that is practical for graduating fellows who are typically most comfortable with robotic surgery as they start practice.
There are several limitations to this study. All procedures were performed by a single experienced laparoscopic surgeon at a single tertiary referral center, which may affect reproducibility. Moreover, the inherent technical challenges associated with LESS may limit its application in routine practice. In addition, because a single technique using an energy device was employed for all procedures, comparison between outcomes and excisional techniques cannot be evaluated. However, this series begins to fill the void in the literature for long-term follow-up of pediatric patients who have undergone LESS partial nephrectomy for upper urinary tract duplication and fusion anomalies.
Conclusions
LESS partial nephrectomy is safe for renal duplication and fusion anomalies with good long-term outcomes. Although it can be safely performed, it is a technically demanding procedure and has been discontinued in favor of robotic partial nephrectomy.
Footnotes
Author Disclosure Statement
P.H.N. is a paid speaker for Intuitive. No competing financial interests exist for the other authors.
Funding Information
No funding was received for this article.