
Abstract
Introduction:
MOSES™ technology is a holmium:yttrium-aluminum-garnet laser pulse mode shown to minimize stone retropulsion. This may facilitate lithotripsy at higher power settings. However, power and heat production are proportional, and temperatures capable of tissue injury may occur during ureteroscopic lithotripsy. Although previous in vitro studies demonstrate the importance of irrigation and activation time on heat production, the impact of pulse type has not been evaluated.
Methods:
A flexible ureteroscope with a 365 μm laser fiber was placed in an 11/13 F access sheath inserted into a 50 mL saline bag to simulate a ureter, renal pelvis, and antegrade irrigant flow. A thermocouple was placed adjacent to the laser tip, and the laser fired for 30 seconds at 0.6 J/6 Hz, 0.8 J/8 Hz, 1 J/10 Hz, 1 J/20 Hz, and 0.2 J/70 Hz at irrigation pressure of 100 mmHg. Four runs were tested per setting using short pulse, long pulse (LP), MOSES-contact (MC), and MOSES-distance (MD) modes. The mean temperature changes (dT) were compared and thermal dose was calculated in cumulative equivalent minutes at 43°C (CEM43) using an adjusted baseline of 37°C. CEM43 ≥ 120 minutes was considered the tissue injury threshold.
Results:
At 0.8 J/8 Hz, LP produced the greatest dT, significantly higher than MC (p = 0.041). CEM43 did not exceed the injury threshold. At 1 J/10 Hz, dT was significantly higher for LP versus MC and MD (p = 0.024 and 0.045, respectively). Thermal dose remained below the injury threshold. No differences in dT were seen between pulse types at 0.6 J/6 Hz, 0.2 J/70 Hz, or 1 J/20 Hz. At 1 J/20 Hz, thermal dose exceeded the injury threshold for all pulse types within 3 seconds.
Conclusions:
Laser pulse type and length seemed to impact heat production in our ureteral model. LP produced significantly greater temperatures at 0.8 J/8 Hz and 1 J/10 Hz relative to MOSES settings. Fortunately, thermal dose remained safe at these settings. Both LP and MOSES technology have been shown to reduce stone retropulsion. At power ≤10 W, the latter may confer this advantage with decreased heat production.
Introduction
New Holmium:Yttrium-Aluminum-Garnet (Ho:YAG) laser technology has introduced a variety of settings, including higher energy and frequency and variable pulse length to increase lithotripsy efficiency during ureteroscopy, although the advantages of these new technologies have not yet been proven in vivo. 1 –3 MOSES™ technology is a manufacturer-specific laser delivery mode modeled on the “Moses effect,” in which the vapor bubble created by an initial laser pulse is used to improve the energy transmission of a closely following second laser pulse. Increased laser pulse length and MOSES modes have been shown to reduce stone retropulsion in vitro and thus may allow for lithotripsy at higher power without the need to constantly chase and re-engage the stone. 3,4
Because of their photothermal mechanism of lithotripsy, Ho:YAG lasers can produce significant heat at high power settings, risking thermal injury to the ureter even without direct contact between the laser fiber and the ureteral wall. In vitro studies have demonstrated potentially injurious temperatures may be achieved during ureteroscopic laser discharge using standard, short-pulse (SP) laser settings. 5,6 Although these studies have shown the importance of irrigation and laser activation time, we sought to demonstrate the impact of laser pulse length and type on laser-generated heat production in a benchtop ureteral model.
Methods
A digital flexible ureteroscope (Lithovue; Boston Scientific, Marlborough, MA) was placed 15 cm into a 36 cm, 11/13 F ureteral access sheath (Navigator; Boston Scientific) to simulate the ureteroscope position for a mid-ureteral stone. To simulate the reservoir effect of the renal pelvis and calices, the distal end of the access sheath was placed into a full 50 mL saline bag. Room temperature (∼20°C) 0.9% saline irrigation was delivered through the working channel of the ureteroscope at a pressure of 100 mmHg using a programmable fluid management device (FluidSmart; Thermedx, Cleveland, OH). Irrigation flow was measured by capturing the irrigation leaving the system into a graduated vessel and was measured to be 13.1 mL/minute. A wire thermocouple (Omega Engineering, Norwalk, CT) was placed within the ureteral model parallel to and 3 mm from the tip of a 365 μm laser fiber that was passed through the working channel of the ureteroscope until the tip could be seen within the ureteral model lumen using the optics of the ureteroscope (Fig. 1). A 120 W Ho:YAG laser (Pulse 120H; Lumenis, Yokneam, Israel) was used to deliver laser energy at multiple combinations of energy and frequency; specifically 0.6 J/6 Hz, 0.8 J/8 Hz, 1 J/10 Hz, 1 J/20 Hz, and 0.2 J/70 Hz for 30 seconds each. These settings were tested four times for each pulse type available on the laser: SP, long pulse (LP), MOSES-contact (MC) and MOSES-distance (MD). Mean temperature change (dT) from a baseline adjusted to 37°C was recorded at 1-second intervals for the first 5 seconds, then every 5 seconds until 30 seconds had elapsed. Thermal dose at these time intervals was calculated in cumulative equivalent minutes at 43°C (CEM43) using the following equation as described by Sapareto and Dewey 7 :
where Δt is the time interval, and T is the average temperature during time interval Δt. R is an experimentally derived constant related to the temperature dependence of the rate of cell death: R(T < 43°C) = 0.5, R(T ≥ 43°C) = 0.25. As described in Sapareto and Dewey and as utilized by others, CEM43 of 120 minutes was used as a threshold for tissue injury. 7,8

The mean change in temperature and time to reach CEM43 of 120 minutes were analyzed for significance with one-way analysis of variance (ANOVA) performed with Tukey's honest significant difference post hoc test to make pairwise comparisons. Statistics were performed with SPSS (v25; IBM Corp., Armonk, NY). A value of p < 0.05 was considered statistically significant for all comparisons.
Results
dT from baseline at 0.6 J/6 Hz was highest using LP; however, this finding was not statistically significant (Fig. 2a). Thermal dose remained under the threshold for injury at all pulse types (Fig. 3a). At 0.8 J/8 Hz, LP again generated the greatest temperature increase from baseline, which was significant relative to MC (p = 0.041) (Fig. 2b). Thermal dose remained below the threshold for injury (Fig. 3b). At 1 J/10 Hz, LP maintained significantly higher temperature increases relative to MC and MD (p = 0.024 and 0.045, respectively) (Fig. 2c). Thermal dose again remained below the threshold for injury (Fig. 3c).
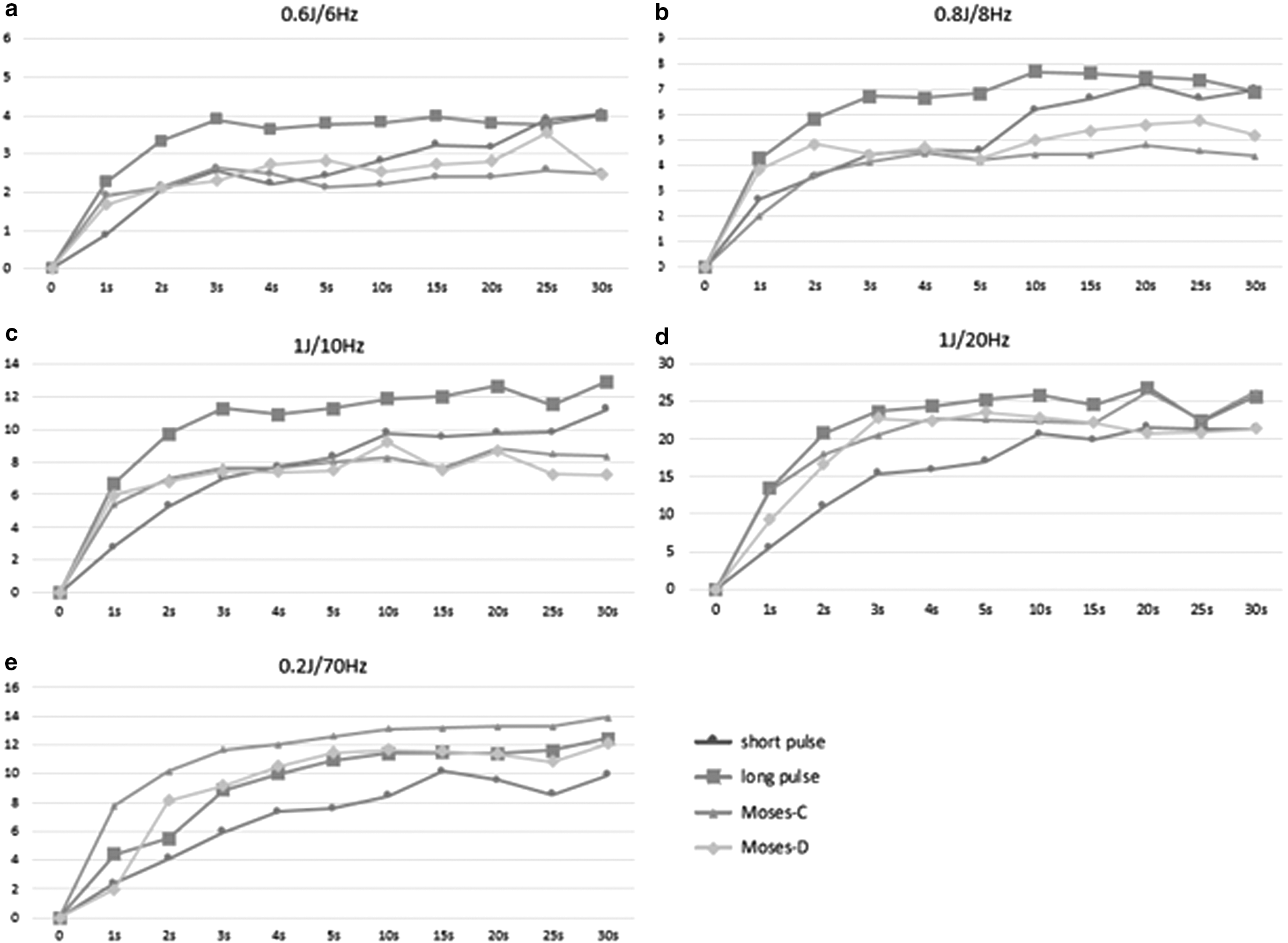
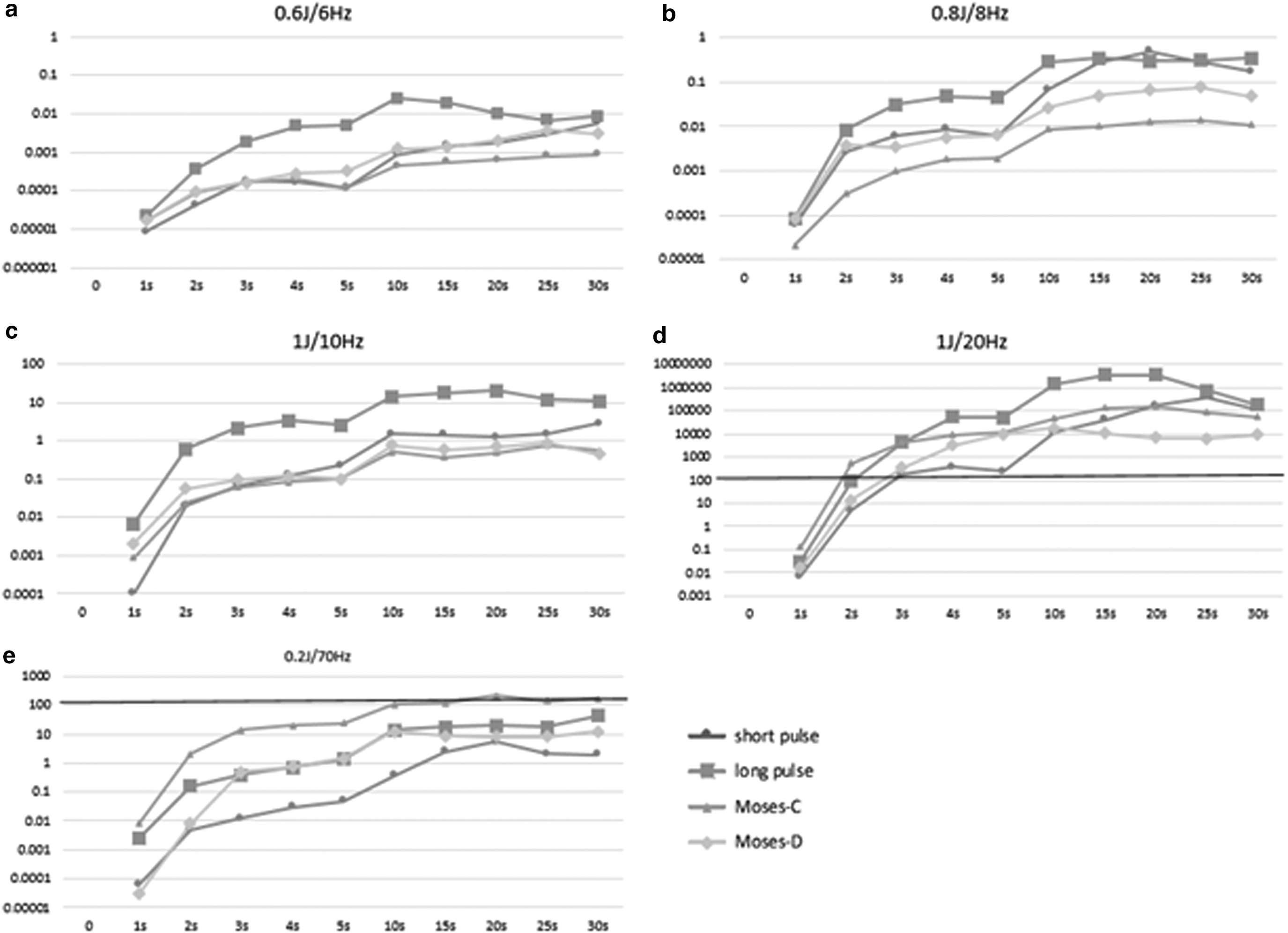
At 1 J/20 Hz, LP produced the greatest temperature change from baseline; however, this was not significant relative to any of the other tested pulse types (Fig. 2d). Similarly, no significant differences in temperature change from baseline were seen between pulse types at 0.2 J/70 Hz (Fig. 2e). All pulse types approached the thermal injury threshold with the exception of MC, which exceed the threshold by a small margin, at 0.2 J/70 Hz (Fig. 3e). At 1 J/20 Hz, thermal dose exceeded the injury threshold for all pulse types in <3 seconds of activation (Fig. 3d). Pulse type did not significantly impact the speed that these temperatures were reached.
Discussion
The latest laser technology has created new opportunities for the treatment of urinary calculi. Not only are many newer lasers able to deliver high energy and high frequency, but they also offer the ability to reduce stone retropulsion with stabilization modes such as MOSES and manipulation of pulse length. 3,4 This may enable the urologist to use higher power laser settings without fear of chasing a stone and risking ureteral injury or the need to change from rigid to flexible ureteroscopy because of proximal stone migration. However, higher power lithotripsy may increase the risk of thermal injury to the urinary tract.
The heat production associated with the photothermal mechanism of Ho:YAG lithotripsy was well described nearly two decades ago. 9 However, Ho:YAG lasers with the ability to deliver high energy, high frequency, and potentially high heat have only recently become clinically available. Thermal injury to tissues may occur at temperatures >43°C; however, injury is dependent on both temperature and exposure time. 10 Thermal dose or CEM43 takes into account both temperature and exposure time to give a standardized measure of injury potential. Tissue injury requires 120 to 240 minutes of exposure at 43°C, therefore we consider the threshold for injury expressed as any value greater than or equal to a CEM43 of 120 minutes. 7
To our knowledge, this is the first benchtop study to investigate the effect of laser pulse length and pulse type on heat production during laser activation. We found that laser pulse length and pulse type impact the production of heat in our ureteral model. LP laser settings produced the greatest heat at most tested energy/frequency combinations. Conversely, the MOSES modes produced the least heat at settings ≤10 W of power. The clinical relevance of these differences is debatable as the thermal dose for all pulse types remained under the threshold for injury throughout testing at settings ≤10 W where discrimination between pulse types was seen. Thermal dose reached potentially dangerous levels at 1 J/20 Hz, but without significant differences between pulse types. In addition, MC was the only pulse type to exceed the thermal dose threshold at 0.2 J/70 Hz, although this was not statistically significant relative to the other tested pulse types. These observations suggest thermal dose may be less dependent on pulse type at higher power and surgeons should continue to use caution at high power regardless of the pulse type used.
The etiology of these observed differences in heat production between pulse types is likely to be multifactorial and has not been completely elucidated. We emphasize that within the confines of a clinical setting, the surgeon can only control those settings on the user interface of the laser. The knowledge that using a certain pulse setting may result in greater heat generation is important for patient safety regardless of the underlying mechanisms.
Nonetheless, the existing knowledge on the subject offers some clues to our observations. Our group has previously demonstrated that high-power laser settings can create potentially dangerous temperatures in vitro, and that judicious use of irrigation and limitation of laser activation time may protect against tissue injury. 6,11 This study builds upon this work by examining the impact of laser pulse type. It is possible that the total power output of the laser varies significantly when pulse type is changed despite identical user-controlled settings for pulse energy and frequency. Per the Food and Drug Administration regulations, a medical laser must operate within ±20% of the indicated setting. 12 This allows for variability that could account for the results reported in this study. Unfortunately, on currently available systems, the operating urologist does not have the benefit of a power meter to indicate the actual power output of the laser in real time as settings are adjusted.
The relationship between laser pulse length and temperature generation has been previously described. Lin 13 reported that if a laser pulse is assumed to be a square pulse in time, then the temperature of irradiated material will rise as one half power of the pulse length. Imagining a train of laser pulses, it is easy to observe that for a fixed number of pulses at a fixed pulse energy, a longer pulse length results in more active laser time over a given period than a shorter pulse length, leaving less time for cooling between pulses.
We observed no statistical difference in heat production between pulse types at 0.6 J/6 Hz, 0.2 J/70 Hz, and 1 J/20 Hz. For low pulse energies of 0.2 J and 0.6 J, this may be explained by recent work by Hardy and colleagues 14 using the same model Ho:YAG laser used in this study, demonstrating that pulse energy and pulse duration are correlated. They report a maximum pulse duration of 200 μs at a pulse energy of 0.2 J using the LP mode. This lengthens to 350 μs at 0.4 J, and continues in this way such that the longest pulse duration of 1100 μs was observed with a pulse energy of 4.0 J. Thus, at very low pulse energy, the pulse length of the various pulse settings is likely similar and may help to explain our findings of minimal difference between pulse types.
The impact of pulse length on temperature generation has been examined sparsely and to the best of our knowledge, no investigation has reported on the thermal properties of MOSES or other stone stabilization modes. Using a glass test tube submerged in a 37°C bath as a caliceal model, Hein and colleagues 15 compared the heat generated by SP versus LP at 15 and 100 W of power. They report SP produced between 6.5% and 9.5% higher temperatures relative to LP but provide no statistical analysis to determine the significance of these results.
We selected a ureteral model rather than a caliceal model to investigate laser-generated heat because the potential for injury in the ureter is increased secondary to less surrounding vasculature acting as a heat-sink and the narrow luminal working space that limits free flow of irrigation. In addition, reduction of stone retropulsion is highly desirable in the ureter because retropulsion of a stone proximally into the renal collecting system can significantly increase the time, number of necessary instruments, and therefore the overall cost required to complete the procedure. The use of LP and anti-retropulsion settings such as MOSES are therefore highly desirable during intraureteral lithotripsy.
Although smaller diameter fibers are often used during ureteroscopy, as in our previous study, 11 we chose to use a 365 μm fiber to provide the most conservative extrapolation to clinical scenarios. The larger diameter of the 365 μm fiber restricts the flow of cooling irrigation through the ureteroscope more than a small fiber of 200 or 273 μm. 16 The larger fiber may generate more heat as well. Buttice and colleagues 17 observed faster temperature elevations during laser activation in a kidney model using a 272 μm compared with a 200 μm fiber.
Similarly, we used a “moderate” irrigation pressure of 100 mmHg. Moderation or cessation of irrigation is often used during ureteroscopy to reduce stone movement and avoid possible pyelovenous backflow and sepsis. 18
There are several limitations to recognize in this study. First, we report our results as temperature changes from an adjusted baseline of normal body temperature, or 37°C. We recognize that intraureteral temperature is a complex result of the irrigation temperature, flow rate, and any heating or cooling that may occur within the patient. Of note, the use of irrigation that has not been heated will add a margin of safety proportional to the relative coolness of the irrigation and the flow rate. The use of continuous versus pulsed irrigation may additionally impact laser-induced heating. In addition, irrigation flow in a ureter capable of collapse, dilation, and peristalsis may differ significantly from that seen in this model. Thus, further study in vivo is required in this area. Second, our model does not incorporate a stone. Lithotripsy implies the presence of a stone and as the intended target of laser energy, the stone may absorb laser energy that would otherwise contribute to heat production. However, including a stone confounds our aim to directly compare the impact of pulse type on irrigation temperature, as the stone itself unpredictably changes irrigation flow as it is fragmented by the laser.
Conclusions
Laser pulse length and pulse type seem to impact the production of heat in our in vitro ureteral model. LP produced significantly greater maximum temperature changes from baseline at 0.8 J/8 Hz and 1 J/10 Hz relative to MOSES settings. Fortunately, thermal dose remained safe at these settings. Both LP and MOSES technology have been shown to reduce stone retropulsion. At power ≤10 W, the latter may confer this advantage with decreased heat production.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the American Urological Association or the Urology Care Foundation.
Footnotes
Author Disclosure Statement
G.P.: consultant, Boston Scientific; M.L.: consultant, Boston Scientific; all other authors have no competing financial interests.
Funding Information
This study was supported in part by the Urology Care Foundation Research Scholar Award Program and American Urological Association (AUA) Southeastern Section.