
Abstract
Objective:
The aim of this research was to verify the efficacy and complication of flexible ureteroscopic holmium laser incision for simple renal cysts (SRCs).
Patients and Methods:
We retrospectively reviewed 116 patients who not only had done flexible ureteroscopic holmium laser incision or laparoscopic decortication for SRC in our institution but also had sufficient data: preoperative information and >1-year follow-up records. The following variables were recorded: age, gender, side, cyst size, location (upper pole, lower pole, and interpolar), blood loss, operative duration, complications during and after surgery, pathology report, and presence or absence of flank pain. The primary endpoint was the efficacy of the treatment; secondary endpoints were safety, pain, and the resolution of other complications. All patients underwent radiologic imaging of the kidneys with a repeated CT, before the operation, 3 and 12 months after surgery. If there were no cysts on the most recent imaging, we defined it as a radiologic success.
Results:
No statistically significant difference in the background variable in patients of group A (64 patients, flexible ureteroscopic holmium laser incision) and group B (52 patients, laparoscopic decortication) was found, including age, gender, cyst's side, cyst's location, and cyst size before the operation. There were less blood loss by surgeons' evaluation and shorter operative duration (p < 0.001) in group A. In group A, there were three patients who had failed in the first time of operation (two patients failed to place flexible ureteroscope through ureter because of ureteral stricture, and one patient was unable to find the renal cyst in the view of flexible ureteroscope), and no severe postoperative complication was observed. The number of postoperative radiologic failure was five at 3 months and three at 12 months in group A, whereas all the procedures were completed laparoscopically, and no conversion was necessary for group B. But there was one patient who had obvious hematuresis for 1 month after the operation and then it was resolved spontaneously at 3 months. There was only one patient who had a radiologic failure in group B, with the cyst of ∼2 cm at 3 months, and his cyst cannot be seen in CT imaging at 12 months without further treatment. There was no statistically significant difference in the rate of effective operation and complication between the two groups.
Conclusion:
The operation of flexible ureteroscopic holmium laser incision for SRC had the advantages of less blood loss, short operation time, with a similar rate of operative success and radiologic success after the operation, compared with the process of laparoscopic decortication. It was a good option for urologists to deal with endogenous renal cysts.
Introduction
Simple renal cysts (SRCs) have been formed in adults commonly, and it increases in incidence with patients' age, with a prevalence of 20% at age 40 years and 33% at age 60 years. 1 –3 The small SRC is asymptomatic and does not have renal function damage. 4 The significant SRC needs treatment because it has symptoms, such as hematuria, pain, obstruction, and hypertension. 5,6
The management of SRC includes open surgery, laparoscopy, renal cyst puncture, and sclerotherapy. 3 With extensive use of flexible ureteroscopy in urology in recent years, a new operation method for SRC, flexible ureteroscopic holmium laser incision, has been carried out in some Chinese medical centers. As one of the earliest institutions that started the flexible ureteroscopic holmium laser incision for SRC in China, our hospital had accumulated >100 cases and rich follow-up data in the past 3 years.
To verify the efficacy and complication of flexible ureteroscopic holmium laser incision for SRC, we made a retrospective study and compared the results of patients who did flexible ureteroscopic holmium laser incision and patients who did laparoscopic decortication in the past 3 years.
Methods
Patients
It was enrolled in the research for patients who not only operated with flexible ureteroscopic holmium laser incision for SRC or laparoscopic renal cyst decapitation in our institution between January 2015 and December 2018 but also had sufficient data of preoperative information and >1-year follow-up records. And the standard of inclusion criteria and exclusion criteria was followed:
Inclusion criteria: (1) recurrent or persistent pain without improvement in conservative treatment; (2) repeated urinary tract infection combined with or without renal calculi, without increase in conservative treatment; (3) renal cysts suggested in CT imaging, with normal renal function or mild to moderate lesions; (4) renal cyst diameter >4 cm; (5) blood pressure and glucose controlled in normal range; (6) Bosniak classification of CT imaging was grade I and II.
Exclusion criteria: (1) history of renal tumor and nephrapostasis; (2) severe cardiac, hepatic, pulmonary and brain dysfunction, without tolerance to general anesthesia; (3) Bosniak classification of CT imaging was grade III and IV; (4) polycystic kidney.
All the patients finished the renal contrast-enhanced CT and multiplane imaging reconstruction before operation (Fig. 1). According to the adjacent relationship of renal cyst, renal pelvic, and renal surface, renal cysts were classified to exogenous, mixed, and endogenous types. The endogenous renal cysts: there was at least one section of CT imaging in which the renal cyst was closely associated with renal pelvic. According to our surgical experience, only the junction between the renal cyst and renal pelvic was >10 mm in one section of CT imaging, and the renal cysts could be found in the flexible ureteroscopy in our experiences. The exogenous renal cysts: part of renal cysts was located on the surface of the kidney. The mixed renal cysts: renal cysts and renal pelvic, and renal surface were adjacent.
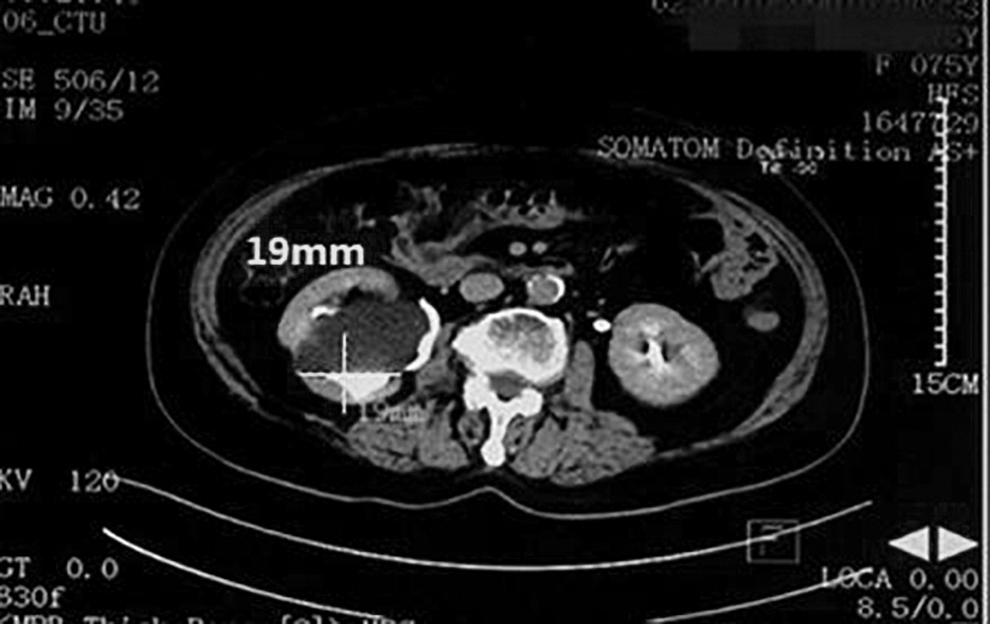
Multiplane imaging reconstruction of renal contrast-enhanced CT and the longest junction of this patient between the renal cyst and renal pelvic was 19 mm.
Our surgical options and grouping
The patients, with endogenous renal cysts and the junction between the renal cyst and renal pelvic >10 mm in CT reconstruction imaging, were done in the surgical procedure of flexible ureteroscopic holmium laser incision. The patients with exogenous renal cysts were done in the surgical procedure of laparoscopic decortication. According to the length of tight junction of renal cyst, renal pelvic, and renal surface, the patients with mixed renal cysts did in the surgical procedure of flexible ureteroscopic holmium laser incision, if the junction of the renal cyst and renal pelvic was longer. Or the patients did in the surgical procedure of laparoscopic decortication if the intersection of the renal cyst and the renal surface was longer. Depending on different surgeries, the patients were divided into group A (the group of flexible ureteroscopic holmium laser incision) and group B (the group of laparoscopic decortication).
Surgical technique flexible ureteroscopic holmium laser incision
The electronic flexible ureteroscope (8.5/9.9F, Olympus) was placed into the renal pelvis under general anesthesia, ultimately detecting the renal pelvis cavity and each renal calix. Intraoperative blue translucent renal pelvis in the view of flexible ureteroscope suggested that the location of the renal cyst was close to the renal pelvis. The fiber (200 μm, 1.0 J, and 30 Hz) was used to cut the thin wall ∼1.0 to 3 cm, to obtain the cystic cavity and renal pelvis cavity. The flexible ureteroscope was inserted into the cyst cavity to observe the cystic condition and exclude tumor. Postoperatively, an F6 Double-J stent and catheter were placed routinely, the catheter was removed 1 to 3 days later, and the F6 Double-J stent was removed by cystoscope 14 to 28 days later (Fig. 2).
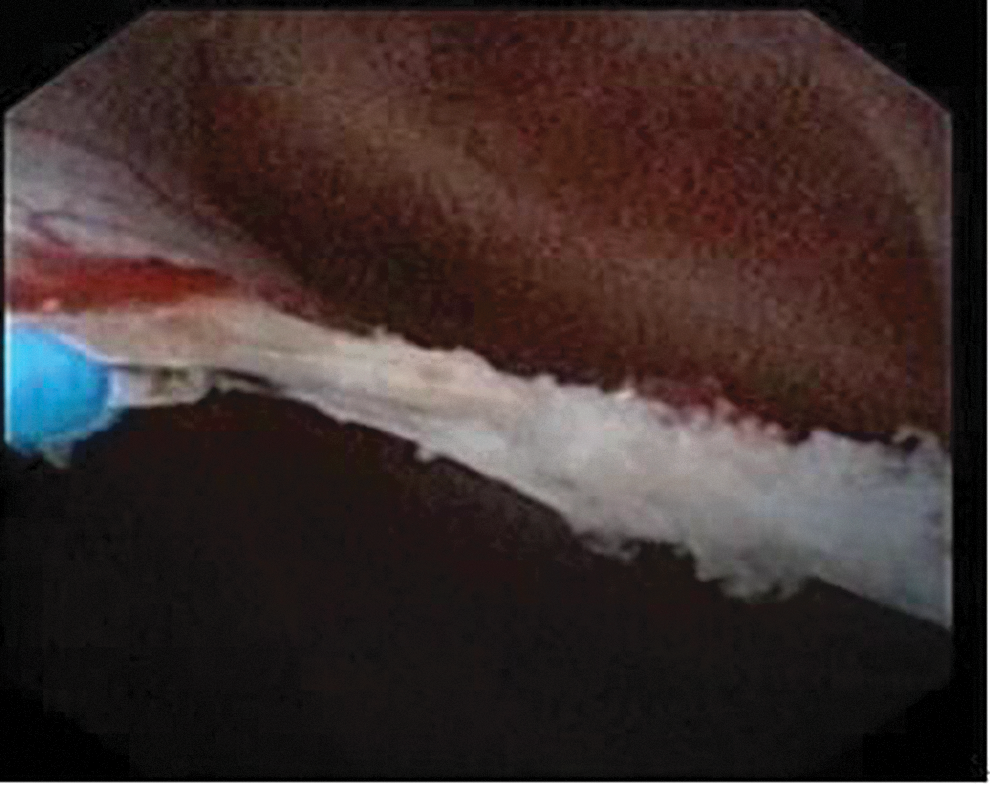
We used a holmium laser to cut the wall of renal cysts by flexible ureteroscope.
Laparoscopic decortication
Basically, we used a transabdominal approach, but if the cysts were dorsal to the kidney, we used a retroperitoneal approach. The procedure involved three trocars: one trocar of 12 mm and two trocars of 5 mm. Retroperitoneal fat tissue was dissected and the psoas muscle and ureter identified. After having identified the renal cyst, electrocautery scissors were used to open the exophytic wall. The cystic cavity was thoroughly examined for the presence of neoplastic changes, and if no suspicious lesions were found, the wall resected with warm scissors up to the limit of the regular renal parenchyma edges. The cystic wall was then submitted for formal histopathologic examination to exclude malignancy. The sides were fulgurated as near as possible to the base of the cyst. At the end of the procedure, a small 18F drainage was left in situ and removed on the first day after surgery.
Outcomes
The following variables were recorded: age, gender, side, cyst size, location (upper pole, lower pole, and interpolar), blood loss, operative duration, complications during and after surgery, pathology report, and presence or absence of flank pain. The primary endpoint was the efficacy of the treatment; secondary endpoints were safety, pain, and the resolution of other complications. All patients underwent radiologic imaging of the kidneys with a repeated CT, 3, and 12 months after surgery. If there were no cysts on the most recent imaging, we defined it as a radiologic success.
Pre- and postoperative lumbar pain scores of the patients were evaluated by the nurse of our department. The pain score was assessed by means of a 10-point visual analog scale ranging from 0 (no pain) to 10 (severest pain). Pain intensity was graded on a scale of 0 to 3 (slight), 4 to 6 (moderate), and >6 (severe). Patients with a pain score >3, or with a residual pain rating, were categorized having a symptomatic failure. The others were recorded as having symptomatic success.
Statistical analyses
SPSS19.0 statistical software was used to process the data, and t-test was adopted for calculation data comparison and χ 2 test for enumeration data comparison, where p < 0.05 was defined as a statistically significant difference.
Results
There were 116 patients who met the standard of inclusion criteria and exclusion criteria in the past 3 years. Sixty-four patients did in the surgical procedure of flexible ureteroscopic holmium laser incision, and they were divided into group A, whereas there were 52 patients in group B who did in the surgical procedure of laparoscopic decortication. All the 116 had the follow-up of >12 months: the mean follow-up was 16.7 ± 3.1 month. The two groups were comparable in terms of age and gender (Table 1). There were 3 patients who did the operation for bilateral cysts in one surgery in group A, and the other 113 patients (the rest patients in group A and all the patients in group B) did the operation for one side's cysts in one surgery. The mean cyst size at CT was 5.7 ± 2.6 cm in group A and 6.4 ± 2.9 cm in group B (p > 0.05).
The Characteristics of Patients, and the Perioperative Results and Follow-Up
SD = standard deviation.
There were three patients who fail in the operation of flexible ureteroscopic holmium laser incision. Two patients had a ureteral stricture, and flexible ureteroscope could not pass through the ureter and see the renal cysts. We placed F5 Double-J stent in the two patients, and we did the second operation of flexible ureteroscopic holmium laser incision for them 2 weeks later. One patient had the problem that we could not find the renal cyst in the view of the flexible ureteroscope. Intraoperatively we drew liquid from the renal cyst and injected ethanol into the cyst under the direction of B-ultrasonic scan.
There was no severe postoperative complication in group A. Postoperative a certain grade of hematuresis was relieved in some patients when their Double-J stent was removed. All the laparoscopic surgeries in group B were performed without any transition to open surgery. But there was one patient who had obvious hematuresis during 1 month after the operation and then it was resolved spontaneously at 3 months. The mean operative duration was 23 ± 7.6 minutes in group A and 47 ± 10.8 minutes in group B (p < 0.001). All patients were mobilized on the first day after surgery, and oral intake started on the first or second day. The mean hospital stay was 2.6 ± 0.8 days in group A and 3.1 ± 0.9 days in group B (p > 0.05).
There was no evidence of tumors in all cases of pathology analysis, but only the presence of chronic inflammation of the cystic wall. The data of intraoperative blood loss was from the surgeons' evaluation: there was no or little blood loss in group A, whereas there was ∼10 to 50 mL of blood loss in group B. The patients have not performed the operation if they had the condition of infections before the surgery. There were seven patients (three patients from group A and four patients from group B) who had fever condition after the operation (all their highest temperatures were <±38.5). The intravenous antibiotic was given for three patients from group A, and oral antibiotic was given for four patients from group B. All the seven patients' infective conditions were cured when they left the hospital. And no more severe condition of infections was found in those patients.
Seven patients in group A and five patients in group B had flank pain before surgery, with mean scores of 7.1 ± 2.3 and 6.8 ± 1.9, respectively, on the visual analog scale. At 3 months, the pain was reduced in all patients (all patients' scores were <3), with a mean score of 1.6 ± 0.3 for group A and 1.9 ± 0.5 for group B (p > 0.05, Table 1).
There were five patients who had a radiologic failure in group A, with cysts in CT imaging at 3 months after the operation, and the number decreased to three patients at 12 months (Fig. 3: the follow-up of one patient with flexible ureteroscopic holmium laser incision before and after the operation). Only one patient required further treatment because his cyst did not get smaller. We drew liquid from the renal cyst and injected ethanol into it, and this treatment was effective. The remaining two patients did not require further treatment. Compared to the condition of the cysts before the operation, two patients' cysts got obviously smaller after the operation, whereas there was only one patient who had a radiologic failure in group B, with the cyst of ∼2 cm at 3 months, and his cyst cannot be seen in CT imaging at 12 months without further treatment. The number of patients between two groups who had a radiologic failure did not have a statistically significant difference (p > 0.05, Table 1).

The CT imaging of one patient with flexible ureteroscopic holmium laser incision before the operation, 1 month after the operation and 18 months after the operation.
Discussion
Endogenous renal cysts were once a difficult problem for urologist. 7 Worrying about the kidney damage and bleeding, it was hard for urologists to choose the suitable therapeutic schedule, no matter laparoscopic decortication or renal cyst puncture, to cure endogenous renal cysts. Until we found the flexible ureteroscopic holmium laser incision that may be the right choice for urologists to deal with endogenous renal cysts, 8 and the peripelvic renal cysts were rare entities of renal cysts that may cause obstruction symptoms earlier than SRC, thus it needed to be treated in earlier stage and the treatment of flexible ureteroscopic holmium laser incision was still a suitable choice for peripelvic renal cysts.
Compared to other treatment of SRC, flexible ureteroscopic holmium laser incision had been proven to be safe and feasible in different researches. 8 –10 Compared to pure aspiration with sclerotherapy, this treatment had better curative effects. And compared to laparoscopic decortication, the flexible ureteroscopic holmium laser incision had less blood loss and shorter operation time that we had seen similar results in our research.
Liaconis and Basiri first reported ureteroscopic treatment of parapelvic renal cyst with flexible and semirigid ureteroscope. 11,12 So far, there were many institutions and urologists to use flexible ureteroscopic treatment for SRC. Luo et al. reported the disappearance of parapelvic renal cyst in 10 of 15 patients at 6 or 12 months after flexible ureteroscope. 13 Professor Zhao had reported 27 patients (totally 28 patients) have satisfied results after flexible ureteroscope (the range of follow-up time: 10–72 months). 14 Professor Mao's team reported all 21 patients with operative efficacy, under the use of flexible ureteroscope with a holmium laser (the average follow-up time: >15 months). 15 Professor Wang in our institution had reported that multi-planar reconstruction (MPR) image post-processing technique-computed tomography (CT) urography (CTU) combined with intraoperative ultrasonography-guided would increase the rate of success for flexible ureteroscope in the treatment of renal cystic disease. 16 Another professor Wang proved that intraoperative methylene blue injection was a useful and straightforward method for urologists to locate the position of renal cyst in the view of flexible ureteroscope and increased the success rate of operation. 17
The critical point of this operation is to find a renal cyst in the view of flexible ureteroscope in order not to injure renal parenchyma or operation failure. The selected patients were key step. 16,17 According to our experience, if we could find the maximum diameter of tight junction between renal cyst and renal pelvic >10 mm in any layer of the reconstruction of renal contrast-enhanced CT (it consisted of three-dimensional lays: transverse lay, longitudinal lay, and tubular lay), there was a significant possibility for us to find renal cyst in the view of flexible ureteroscope.
Compared to other treatment for SRC, such as pure aspiration with sclerotherapy and laparoscopic decortication, flexible ureteroscope was a different surgery option in urology. Queried the database of PubMed, we did not find the article about the efficacy between the flexible ureteroscope and laparoscopic decortication for SRC. Because it was widely accepted by urologists to choose laparoscopic unroofing for SRC. It was an excellent method to prove the value of flexible ureteroscope for SRC by comparing the efficacy and complication between flexible ureteroscope and laparoscopic unroofing for SRC.
In our retrospective research, it had been proved that flexible ureteroscope's group had less blood loss and shorter operation time, compared with the laparoscopic group. After the operation of flexible ureteroscope, all seven patients, who had lumbago before the surgery, had recovered and had a low grade of visual analog scale (<3). It was satisfied that all the patients in group A did not have serious complication after the operation. However, the group of flexible ureteroscope had a high rate of radiologic failure at 3 and 12 months after the surgery. When we revived the information of five unsatisfied patients of group A, we found two main reasons: three patients had big renal cysts before the operation (the maximum diameter of cysts: 8.5, 9.1, and 8.7 cm); the other two patients had small incision of cyst wall in operation. When we focused the rate of operative success, the ureteral stricture was the problem we had to face and deal. It was an excellent way to place the ureter stent before the operation to solve minor ureteral stricture. And the patients with severe ureteral stricture were not suitable for flexible ureteroscope.
There were some limitations of flexible ureteroscopic holmium laser incision for SRC: (1) We had some tools to get the sample under flexible ureteroscopy. This operation did not have the sample, and histopathology of cysts could not be tested if the sample was so small. (2) Our research was a retrospective study, and there was a selection bias that may affect the results.
Conclusion
The operation of flexible ureteroscopic holmium laser incision for SRC had the advantages of less blood loss, short operation time, with a similar rate of operative success and radiologic failure after the operation, compared with the process of laparoscopic decortication. It was a good option for urologists to deal with endogenous renal cysts and 61 out of 62 patients who did the operation of flexible ureteroscopic holmium laser incision in our research had satisfactory results after the operation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by a plan of the Medical and Health Platform of Zhejiang Province in 2016 [Discipline Leader Program (Category A)]. No. 2016DTA011. A Clinical Study on Ultrasound-Guided Flexible Ureteroscopic Holmium Laser Internal Drainage in Treatment of Polycystic Kidney Disease. A key public welfare project of Huzhou Science and Technology Bureau in 2016. No. 2016GY23. Clinical study of drug concentration of famine and reproductive function in the treatment of chronic viral hepatitis B.