
Abstract
Introduction:
Preoperative alpha-blockers have been proposed to improve intraoperative outcomes and patient stone-free status after ureteroscopy for ureteral stones.
Materials and Methods:
We searched six databases, including Medline, Embase, and Web of Science, for randomized controlled trials (RCTs) evaluating alpha-blocker use before planned ureteroscopy for the management of ureteral calculi. Meta-analysis was performed using DerSimonian and Laird method with inverse variance weighting. Quality of evidence was summarized using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) framework.
Results:
Of 3338 records, 26 were screened as full text and 12 RCTs were included totaling 1352 patients. Meta-analysis demonstrated a 61% risk reduction in need for intraoperative ureteral dilatation in patients administered preoperative alpha-blockers (relative risk [RR]: 0.39 [95% confidence interval, CI: 0.31–0.48], p < 0.00001), as well as increased stone-free status for patients at 4 weeks postoperatively (RR: 1.17 [95% CI: 1.08–1.26], p < 0.0001), and at final follow-up (RR: 1.18 [95% CI: 1.11–1.24], p < 0.00001; median final follow-up 4 weeks [range: 2–8 weeks]). Urologists were more likely to reach the stone with the ureteroscope in patients administered alpha-blockers (RR: 1.16 [95% CI: 1.10–1.23], p < 0.00001). A statistically significant reduction in operative time (mean difference [MD]: −6.05 [95% CI: −10.17 to −1.93] minutes, p = 0.004) and length of hospital stay (weighted MD: −0.34 [95% CI: −0.55 to −0.13] days, p = 0.001) was also demonstrated. Main reported side effects of treatments were abnormal ejaculation, postural hypotension, and dizziness. Outcomes were robust to sensitivity analyses. Results were rated moderate quality evidence using the GRADE framework.
Conclusions:
Among patients scheduled for semirigid ureteroscopy of ureteral stones, use of preoperative alpha-blockers demonstrated a significant reduction in the need for ureteral orifice dilation and an increase in patient stone-free status at follow-up, and facilitates higher rate of ureteroscopic access to stones, although reducing operative time. An adequately powered trial is needed to definitively address the safety and efficacy of preoperative alpha-blockers for ureteroscopy of ureteral stones.
Introduction
Ureteral stones are a common urologic condition affecting as much as 12% of men and 6% of women. 1 Several treatments are available for management with decision-making influenced by stone, clinical, anatomic, and technical factors. 2 Alpha-blockers have been investigated thoroughly in the literature for their role in medical expulsive therapy of ureteral stones. 2 Through the abundance of alpha-1 receptors in distal ureteral muscles and their role in reduction of ureteral muscle tone and peristalsis, they have become a popular option for many urologists to supplement noninvasive therapy of ureteral stones. 3 Recently, there has been increased interest in their potential role in facilitating ureteroscopy and instrumentation of the ureter based on the same pharmacological effects utilized for medical expulsive therapy. Technical studies have supported the use of alpha-blockers used before ureteroscopy by facilitating deployment of ureteral access sheaths without increasing ureteral injuries. 4 Accordingly, there has been a growing interest in evaluating intraoperative and postoperative outcomes in patients administered preoperative alpha-blockers for ureteral stones. Several randomized controlled trials (RCTs) have been conducted, evaluating the role of preoperative alpha-blockers. However, the majority these trials have been single center and suffered from small sample sizes. Accordingly, there has been no consensus on their use. Therefore, we conducted a systematic review and meta-analysis of RCTs to evaluate the safety and efficacy of preoperative alpha-blockers for patients undergoing ureteroscopy for ureteral stones.
Materials and Methods
We conducted this systematic review in accordance with the Cochrane Handbook for Systematic Reviews of Interventions
5
and reported it according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
6
We searched for RCTs evaluating patients administered alpha-blockers before ureteroscopic management of ureteral calculi. The following six databases were searched without language restriction or publication type (full text article or conference abstract) from inception to July 1, 2019: Medline, Embase, Web of Science, CINAHL, Cochrane Central, and CQVIP Chinese database. We also searched for ongoing trials on
Literature search results were downloaded as .RIS files and screened using Mendeley reference manager software (version 1.17.13). Two reviewers (A.K. and B.A.) independently and in duplicate performed study screening according to predefined criteria with disagreements resolved through discussion and consensus. Quality assessment of RCTs was performed with the Cochrane Risk of Bias tool. 7 Data extraction was performed independently and in duplicate by two authors (A.K. and B.A.), with disagreements resolved through discussion and consensus.
Meta-analysis was conducted if three or more RCTs reported defined outcomes. The following outcomes were meta-analyzed: requirement for intraoperative ureteral dilatation, ureteroscopic access to stone (defined as ability of ureteroscope to reach stone successfully), postoperative stone-free rate, operative time, and length of hospital stay. Dichotomous outcomes were reported with relative risk (RR), with corresponding 95% confidence intervals (CIs). Continuous outcomes were reported with weighted mean difference (MD), with corresponding 95% CIs. Random-effects meta-analysis was conducted using DerSimonian and Laird method with inverse variance weighting. 8 Between study statistical heterogeneity was quantified using I 2 statistic. 9 Sensitivity analyses were conducted for each outcome by removing studies with ≤3 days of preoperative alpha-blockers. We considered a p-value of <0.05 to be statistically significant. Statistical analyses were conducted using Review Manager (version 5.3). We also graded the level of evidence using Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach for each outcome. 10
Results
Of 3338 records, 26 articles were reviewed as full text, and 12 RCTs totaling 1352 patients were included in this systematic review with 11 RCTs included in the meta-analysis (Fig. 1; Table 1) after applying predefined criteria outlined in Methods. 11 –22 Two ongoing trials were identified (NCT03614052 and IRCT201702261853N13). Risk of bias is summarized in Figure 2, with most studies suffering from unblinded outcome assessor and unclear random sequence generation. Alpha-blockers administered before ureteroscopy included tamsulosin (n = 8), silodosin (n = 3), and alpha-blockers without reporting a specific drug name (n = 1). Median length of preoperative alpha-blocker use was 1 week. Included RCTs did not report postoperative alpha-blocker use. All reported procedures were elective.
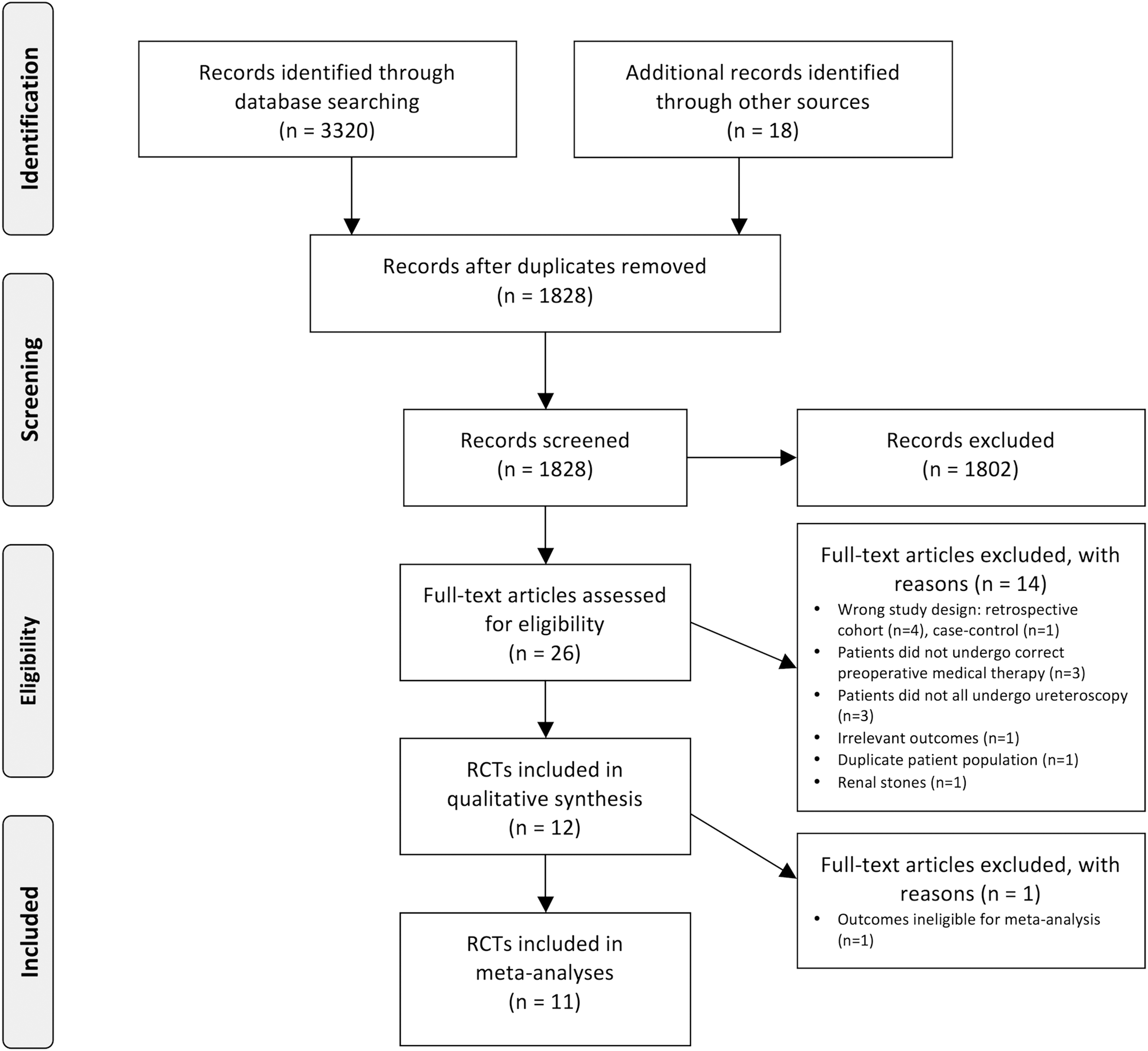
Flow chart of study selection.
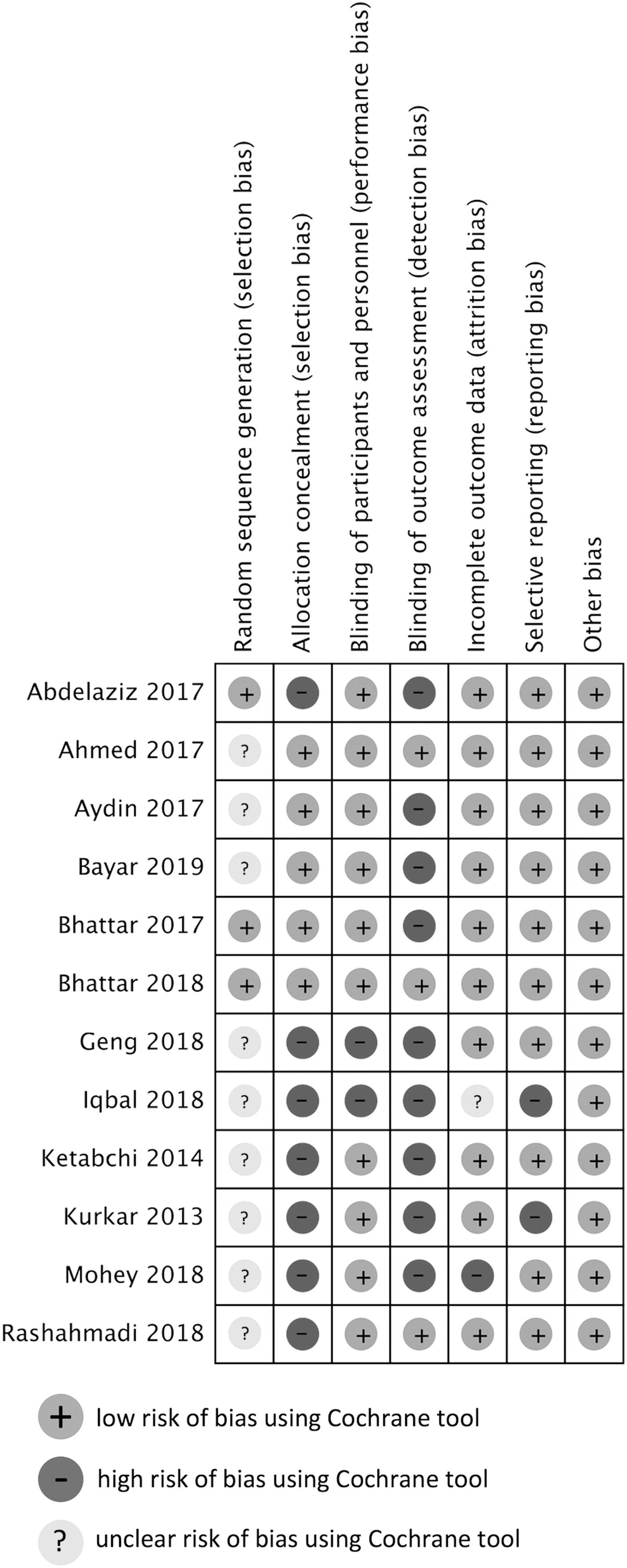
Summary of risk of bias of each study using Cochrane tool. Studies were rated as low, high, or unclear risk of bias for each risk of bias domain.
Summary of Included Randomized Controlled Trials
MCCS = modified Clavien classification system; SD = standard deviation.
Our meta-analysis demonstrated a 61% risk reduction of need for intraoperative ureteral dilatation (RR: 0.39 [95% CI: 0.31–0.48], p < 0.00001; I 2 = 0%; Fig. 3) for patients administered preoperative alpha-blockers compared to placebo/control. Sensitivity analysis removing one study with ≤3 days of preoperative alpha-blockers likewise revealed significant outcome for ureteral dilatation (RR: 0.37 [95% CI: 0.30–0.47], p < 0.00001; I 2 = 0%).

Forest plot for need for intraoperative ureteral dilatation.
Meta-analysis also demonstrated an increased ability to reach the stone ureteroscopically (RR: 1.16 [95% CI: 1.10–1.23], p < 0.00001; I 2 = 0%; Fig. 4) for patients administered preoperative alpha-blockers. Sensitivity analysis removing two studies with ≤3 days of preoperative alpha-blockers also revealed significant outcome for ureteroscopic stone access (RR: 1.18 [95% CI: 1.10–1.27], p < 0.00001; I 2 = 0%).
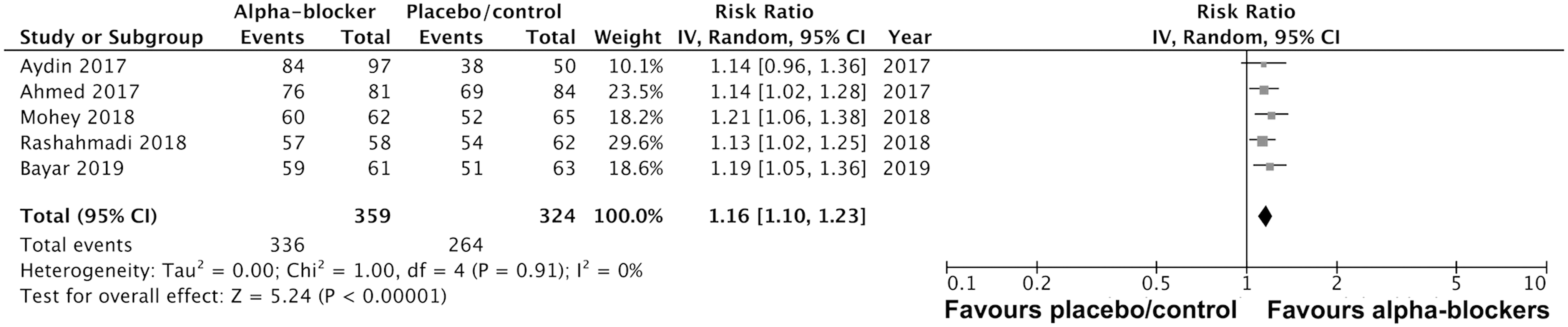
Forest plot for ability to access stone ureteroscopically.
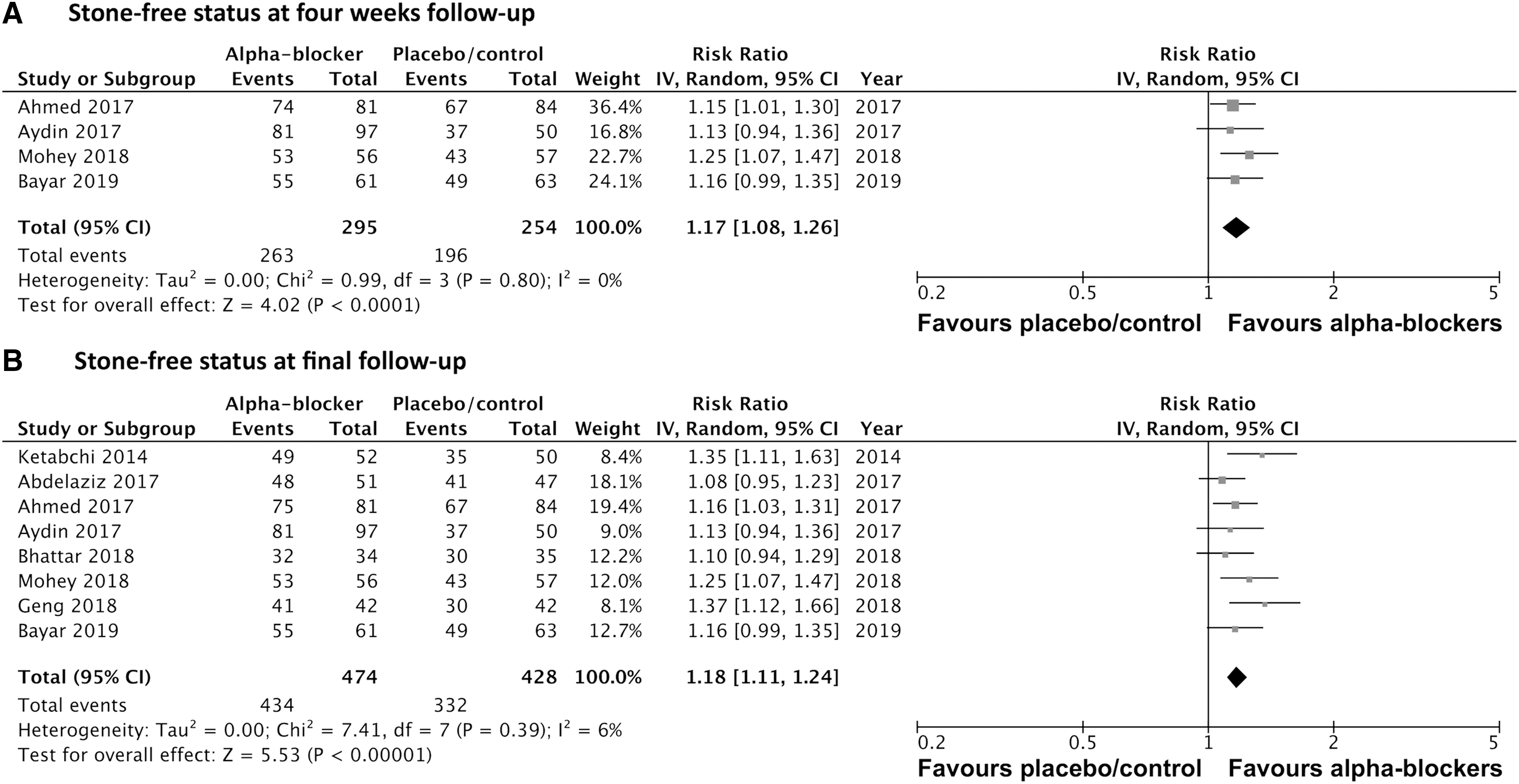
We also found a significant reduction in stone-free status in patients taking preoperative alpha-blockers compared to placebo/control. There was a significant increase in stone-free status at 4-week follow-up (RR: 1.17 [95% CI: 1.08–1.26], p < 0.0001; I 2 = 0%; Fig. 5A), as well as at final follow-up (RR: 1.18 [95% CI: 1.11–1.24], p < 0.00001; I 2 = 6%; median final follow-up 4 weeks [range: 2–8 weeks]; Fig. 5B). Sensitivity analysis removing one study for 4-week follow-up with ≤3 days of preoperative alpha-blockers revealed significant increase in stone-free status (RR: 1.18 [95% CI: 1.08–1.28], p = 0.0001; I 2 = 0%), as well as for final follow-up when removing two studies (RR: 1.16 [95% CI: 1.09–1.24], p < 0.0001; I 2 = 4%).
Operative time was reduced in those patients administered preoperative alpha-blockers (weighted MD: −6.05 [95% CI: −10.17 to −1.93] minutes, p = 0.004; I 2 = 89%; Fig. 6). Sensitivity analysis removing one study with ≤3 days of preoperative alpha-blockers maintained significance for reduced operative time (MD: −7.06 [95% CI: −11.63 to −2.50] minutes, p = 0.002; I 2 = 90%). Finally, our meta-analysis demonstrated a small, however, statistically significant reduction in length of hospital stay in patients administered preoperative alpha-blockers (MD: −0.34 [95% CI: −0.55 to −0.13] days, p = 0.001; I 2 = 51%; Fig. 7), which did not include studies with ≤3 days of preoperative alpha-blockers.

Forest plot for operative time.

Forest plot for patient hospital length of stay.
GRADE assessment demonstrated the following quality of evidence of outcomes: ureteral dilatation (high quality), ureteroscopic access to stone (moderate quality; downgraded for risk of bias), stone-free rate at final follow-up (moderate quality; downgraded for risk of bias), operative time (moderate quality; downgraded for inconsistency), length of hospital stay (moderate quality; downgraded for imprecision), and stone-free rate at 4 weeks (moderate quality; downgraded for risk of bias).
Discussion
The utility of alpha-blocker use before routine ureteroscopy for ureteral stones is unclear and controversial. This systematic review and meta-analysis suggest that preoperative alpha-blocker use in patients undergoing ureteroscopy for ureteral stones significantly improves postoperative patient stone-free status, ureteroscopic access to stones, and need for ureteral dilatation. In addition, use of preoperative alpha-blockers reduces operative time by an average of 6 minutes and reduces patient hospital length of stay. Therefore, this meta-analysis suggests preoperative alpha-blockers as an effective therapy for patients undergoing ureteroscopy of ureteral stones.
The use of alpha-blockers alone or in conjunction with ureteroscopy or shockwave lithotripsy has been reported extensively in the literature. A 2015 multicenter RCT of medical expulsive therapy, including 1136 analyzed patients, reported tamsulosin and nifedipine as not effective in patient stone-free status at 4-week follow-up. 23 This result was different than previous meta-analyses of underpowered studies, which adds caution to our meta-analysis of relatively small RCTs. Several meta-analyses have demonstrated alpha-blockers as effective after shockwave lithotripsy for stone clearance 24 and for relieving patient discomfort after ureteral stent placement. 25 However, no systematic review or meta-analysis has been conducted evaluating the use of preoperative alpha-blockers for ureteroscopy of ureteral calculi.
Several guidelines for the management of ureteral calculi do not advocate for alpha-blockers as preoperative therapy for ureteroscopy as no comprehensive synthesis of evidence has been conducted on this topic. The 2016 American Urological Association guidelines for the management of ureteral calculi recommends alpha-blockers for medical expulsive therapy for distal ureteral stones <10 mm, 26 and perhaps to facilitate passage of fragments after extracorporeal shockwave lithotripsy. However, their use as an effective preoperative adjunct for ureteroscopy is not reported. The 2015 Canadian Urological Association guidelines report alpha-blockers, particularly tamsulosin, as an effective therapy when prescribed after shockwave lithotripsy to increase the success of treatment. 2 Similar to previous guidelines, their use in preoperative ureteroscopy is not mentioned. The European Association of Urology guidelines report medical expulsive therapy as effective when administered after ureteroscopy; however, it does not mention preoperative use of alpha-blockers. 26 Accordingly, intraoperative outcomes such as need for ureteral dilatation, operative time, and hospitalization cannot be explored with postoperative alpha-blocker therapy. The absence of reporting of preoperative alpha-blocker use in ureteroscopy is likely attributable to the majority of included RCTs in our meta-analysis being published after the release of relevant guidelines.
Perhaps one of the most clinically relevant outcomes of this meta-analysis is the significant reduction in the need for ureteral dilation. Failure to access the ureter has been reported to be in the range of 8%–10%. 27 Dilatation is usually needed to navigate a tight ureter or orifice, and is not without complications. 28 Many urologists prefer to stent and come back at a later time. Although many think this is the safest option, it results in inconvenience for the patient with increased costs to the health care system. Preoperative alpha-blockers can be further examined to delineate which patient groups benefit the most, and thus help reduce the risk of dilation-related complications or stenting.
An additional clinically significant outcome of this analysis is the increase in stone-free rate. Despite being treated only preoperatively, meta-analysis demonstrated a significant increase in stone-free rate during follow-up. Although alpha-blockers were used only preoperatively in included RCTs, their effect may continue after discontinuation. According to literature in benign prostatic enlargement, the effect of alpha-blockade does not abate immediately after stopping therapy, as many patients still experience improvement in their lower urinary tract symptoms months after treatment discontinuation. 29 Therefore, there may be a similar, long-term effect after discontinuation of these medications in the included study population.
We do acknowledge that some of the reported statistically significant findings are not as significant clinically. The reduction in operative time by 6 minutes cannot be used as a sole indicator for preoperative treatment. Similarly, the reduction in hospital stay is very minimal, and might be attributed to better pain control in the immediate postoperative period, resulting in faster discharge.
Literature exists studying the impact of preoperative alpha-blockers on ureteral access sheath insertion as well. In a randomized trial by Koo et al., 12F/14F access sheath insertion force was measured with a digital gauge. 30 They demonstrated that patients pretreated with alpha-blockers required significantly less force to insert the access sheath into the ureterovesical junction and up to proximal ureter. 30
The present meta-analysis has several strengths. First, a comprehensive search of six databases was conducted independently and in duplicate without language or publication type (full-text article or conference abstract) restrictions. Non-English articles, such as one that included RCT published in Mandarin, 17 were translated by a medical professional and were included in our analysis to ensure a comprehensive overview of all available relevant literature. In addition, we evaluated all our outcomes according to the GRADE framework, which provides a transparent approach in summarizing evidence for future guideline use. 10
Nevertheless, this systematic review and meta-analysis is not without limitations. First, included studies used various sizes of ureteroscopes, ranging from 6F 19 to 8/9.8F. 16 It is possible that preoperative alpha-blockers may be most effective for larger ureteroscope sizes, given the increased degree of ureteral relaxation required to facilitate a larger ureteroscope, and might be especially beneficial for distal ureteral stones causing ureteral orifice edema, inflammatory changes, and/or ureteral spasm, which might hinder a ureteroscopy. We were unable to quantify the size of ureteroscope for which alpha-blockers may be most effective when used preoperatively. Most studies used variable ureteroscope sizes and no studies reported outcomes for each size. Particularly relevant outcomes that may be interesting to explore in future subgroup analyses include need for intraoperative ureteral dilatation and ureteroscopic stone access. Included RCTs reported data were insufficiently granular to conduct such analyses. However, our meta-analysis demonstrates similar estimates of effectiveness between studies for these outcomes, suggesting that the superior effect of alpha-blockers is generalizable to the range of ureteroscope sizes of included studies.
Second, the optimal length of preoperative alpha-blocker use was not possible to quantify. Clinical experts suggest use of preoperative alpha-blockers for several days, with the majority of included studies administering alpha-blockers for 1 week before ureteroscopy. 11,12,14 Some studies reported ranges of preoperative alpha-blocker usage, which precluded performance of a meta-regression in this study. 15,18,20 We aimed to minimize this limitation by conducting a sensitivity analysis for each meta-analyzed outcome by excluding RCTs with ≤3 days of preoperative alpha-blocker usage in the intervention arm. All sensitivity analyses were congruent with the primary analyses supporting the benefit of preoperative alpha-blocker use compared to placebo or no therapy. In addition, we were unable to determine the optimal length of preoperative alpha-blocker use. However, the median length of preoperative alpha-blocker use in the included studies was 1 week, which may be a convenient length of use for patients and be sufficient for improving outcomes. Accordingly, this length of preoperative alpha-blocker use may be the best approximation for an ideal regimen.
Furthermore, most of the reviewed RCTs did not report clearly on medication-related side effects because of preoperative initiation of alpha-blockers, which prevented a meta-analysis evaluating the safety of alpha-blockers for this indication. Urologists must balance the risk and benefits of any intervention. Although alpha-blocker use is safe for other indications, including management of lower urinary tract symptoms and medical expulsive therapy for calculi, a small number of patients experience significant side effects. Accordingly, this can stand in the way of a generalized recommendation for all patients to be pretreated.
In addition, publication bias was not evaluated statistically as there were fewer than 10 studies in each meta-analysis. Accordingly, the power of a funnel plot test would be too low to evaluate asymmetry. We aimed to minimize publication bias by conducting an extensive literature review of six databases without language or publication type (full text or conference abstract) restrictions, and searched databases (e.g.,
Finally, use of preoperative alpha-blockers in ureteroscopy of pediatric patients was not analyzed as no randomized trials have been conducted on this population. Pediatric populations may have an increased risk of vesicoureteral reflux, ureteral stricture, or ureteral perforation after balloon dilatation. Accordingly, there is a gap of evidence in this population. A 2017 retrospective cohort study of 41 patients published as a conference abstract reports the use of preoperative tamsulosin for ureteral navigation in ureteroscopy in pediatric patients. 31 The authors report that they were able to navigate the ureter in 19 of 22 (86%) patients administered preoperative tamsulosin and 10 of 19 (53%) patients without preoperative tamsulosin, with no significant patient age or weight differences between study arms. This study was limited by its retrospective nature, low sample size, and likely unbalanced patient prognostic factors. Future randomized studies are needed to evaluate the effect of preoperative alpha-blocker therapy in ureteroscopy of ureteral calculi in pediatric populations. Another area of future exploration is whether the use of alpha-blockers carries the same effect in an emergency setting, with short treatment duration and more inflammatory reactions expected. In a retrospective review of patients treated with ureteroscopy (semirigid and flexible ureteroscopy) in an emergency setting, patients receiving preoperative alpha-blockers were noted to have a higher stone-free rate postoperatively. 32
Conclusions
Among patients scheduled for ureteroscopy of ureteral stones, use of preoperative alpha-blockers is associated with a significant reduction in the need for ureteral dilatation at the time of ureteroscopy, increase in patient stone-free status at follow-up, and a higher rate of ureteroscopic access to stones, although reducing operative time. These findings offer clinicians and patients moderate quality evidence of the benefit of preoperative alpha-blockers for ureteroscopic removal of ureteral stones. A large, adequately powered RCT is needed to definitively address the safety and efficacy of preoperative alpha-blockers for ureteroscopy of ureteral stones.
Footnotes
Author Disclosure Statement
K.T.P. and J.Y.L. declare that Cook Urological provides support for their Endourology Fellowship Program. All other authors have no conflicts of interest to disclose.
Funding Information
No funding was received for this article.