
Abstract
Background:
Robotic laparoendoscopic single-site (LESS) partial nephrectomy is not widely used because of its limitations, and true single-site surgery has not previously been possible. To investigate the feasibility of partial nephrectomy using the novel SP surgical system, compare perioperative outcomes using this system and the previous Xi single-site platform (XiSSP), and describe how true single-site partial nephrectomy is possible with the SP system.
Methods:
Retrospective chart review of patients undergoing robotic partial nephrectomy by a single surgeon using the SP surgical system or XiSSP from December 14, 2016 to June 14, 2019. For the SP system, a GelPOINT access platform was placed through a single periumbilical incision. A 25-mm multichannel robotic port and assistant's ports were placed in the GelSeal cap. No additional incisions were required for the assistant or liver traction. The primary outcomes were intraoperative and postoperative complications.
Results:
Fourteen patients underwent single-site partial nephrectomy with the SP surgical system (n = 9) or XiSSP (n = 5). No limitations were noted for accessing tumors in the upper aspect of the kidney using the SP system. One case of tumor fracture occurred with the SP system, and one case of conversion to multiport robotic surgery occurred with the XiSSP. The postoperative course was uneventful in all patients; only Clavien–Dindo 1 complications occurred.
Conclusions:
True single-site partial nephrectomy was performed safely with the SP surgical system. The SP system resolved many limitations associated with LESS and the XiSSP.
Introduction
The development of novel surgical instruments has led to increasing use of minimally invasive surgery to improve cosmesis and decrease postoperative pain, while maintaining equivalent surgical outcomes and low complication rates, compared with open surgery. 1 Laparoscopic surgery, along with various mini-incision methods, is now commonly performed. Laparoendoscopic single-site (LESS) surgery has been developed as part of this trend, but it has not become popular because of the concomitant limited working space. 2 After the introduction of robotic surgery, various methods have been used to overcome the limitations of LESS, and a single-site platform for robotic LESS using a multichannel port, curved cannula, and semirigid instruments has been developed. 3
We have used and reported various methods and techniques for LESS partial nephrectomy. 4 –6 A single-site platform using the da Vinci Xi system (Intuitive, Sunnyvale, CA) with articulating needle drivers was the most feasible for overcoming the various limitations of previous conventional and robotic LESS partial nephrectomy methods. However, the technique had its own limitations, and true single-site surgery was not possible, as at least one more port site was required for access of the assistant's instruments and an additional port was necessary for liver traction in right-sided cases.
Recently, the da Vinci SP surgical system (Intuitive Surgical) has been approved for clinical use by the Korean Food and Drug Administration. This is a purpose-built robotic platform dedicated to single-site, single-port surgery. Kaouk and colleagues reported their successful initial clinical experience of performing pure LESS robotic partial nephrectomy using this novel system. 7
In this report, we present our initial experience of partial nephrectomy using the SP system and compare the perioperative outcomes with those obtained using the Xi single-site platform (XiSSP). We present our step-by-step approach for robotic LESS partial nephrectomy using the SP system and describe how additional ports are not required with this system, allowing true single-site partial nephrectomy.
Materials and Methods
Nine consecutive patients with a single contrast-enhanced renal mass underwent partial nephrectomy using the SP surgical system from December, 2018 to June, 2019. Written informed consent was obtained from all patients, after explanation of the novel surgical system was provided. No specific inclusion or exclusion criteria were used. Perioperative outcomes of these patients were compared with the outcomes of five consecutive patients who underwent partial nephrectomy using the XiSSP system from December, 2016 to February, 2018. Data regarding patient demographics and perioperative outcomes were collected after obtaining approval from the Institutional Review Board of Yonsei University (IRB Approval No. 1-2018-0074). The surgeries were performed by a single surgeon (W.K.H.) at Severance Hospital (Seoul, Korea). The XiSSP procedures were similar to those described in our previous report. 4 Partial nephrectomy using the SP surgical system is described below.
Patient positioning, port placement, and docking
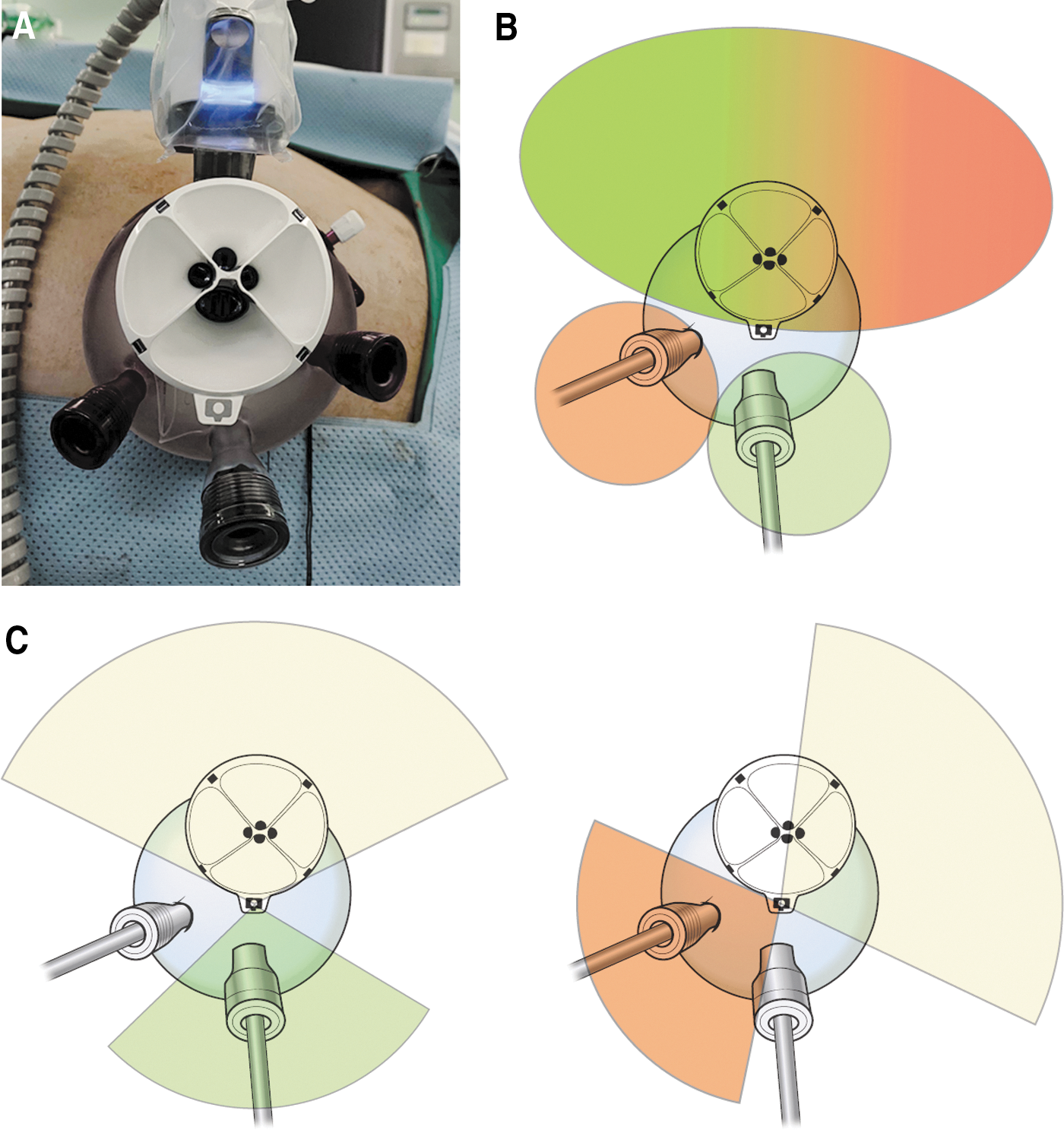
As in conventional multiport robot-assisted partial nephrectomy, the patient is placed in a semilateral position. A 3.5-cm umbilical incision is made, and a GelPOINT advanced access platform (Applied Medical, Rancho Santa Margarita, CA) is inserted after placing a dedicated 25-mm multichannel robotic port and assistant's ports. The 12- and 10-mm sleeves included in the GelPOINT package are used as assistant's ports. Movement of the assistant's instruments is mainly limited by collision with the extracorporeal robot arm (Fig. 1). To overcome this limited range of motion, the assistant's ports are placed in the GelSeal cap, as shown in Figure 2. To minimize collision, the 25-mm multichannel robotic port is placed at the kidney-side end of the GelSeal cap, and the 12-mm port is placed at the opposite end. The 12-mm port is used to introduce laparoscopic bulldog clamps (Aesculap, Tuttlingen, Germany). To widen the area of access for the assistant's instruments, additional 10-mm ports are placed. This allows the assistant to provide adequate traction and suction within the single access site. After the GelPOINT platform is inserted, the SP surgical system is docked.
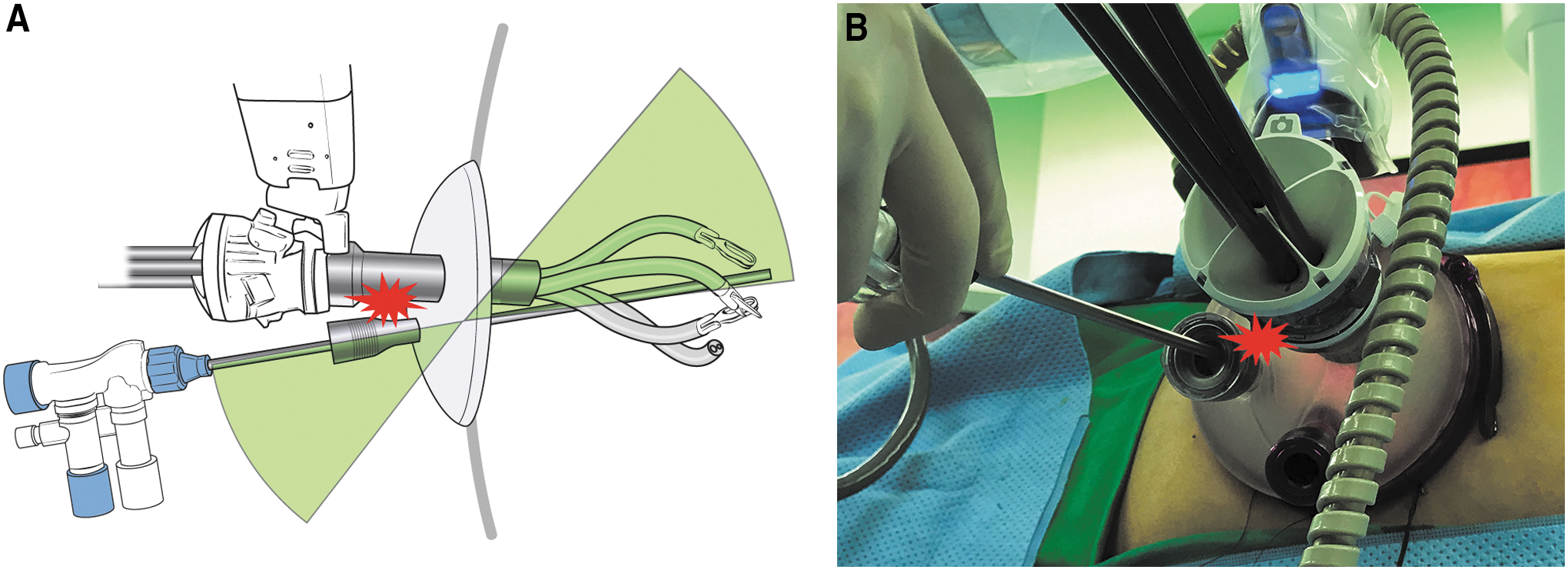
The range of motion of the assistant's instruments is limited because of collision with the extracorporeal robotic arm. Additional ports can be placed to widen the area of access for the assistant's instruments.
Surgical procedures
Partial nephrectomy using the multiport robotic technique is reproduced using the SP surgical system. Although the surgeon (W.K.H.) uses two arms when performing multiport robot-assisted partial nephrectomy, the SP system allows the use of a third arm without the need for an additional trocar and without collision between robotic arms. This additional arm can be used to elevate the liver when exposing the hilum and upper pole of the right kidney (Fig. 3 and Supplementary Fig. S1), making an additional port for liver traction unnecessary and thereby providing true single-site surgery even when operating on right kidneys.
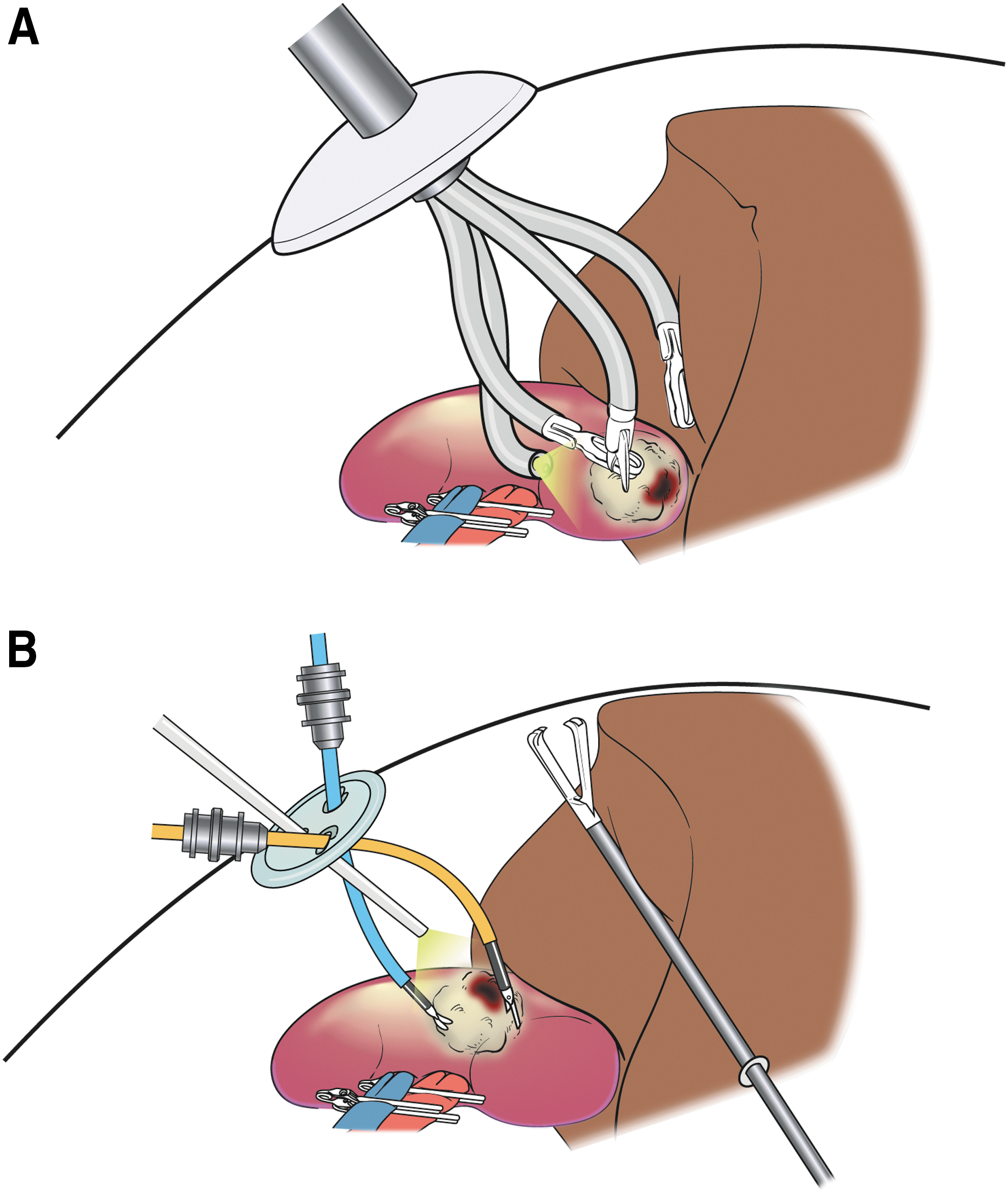
An additional arm can be used to elevate the liver to expose the hilum and upper pole of the right kidney. This contrasts with the need for an additional subxiphoid port when using the Xi single-site platform.
After the kidney is exposed, the hilum is dissected, and renal vessels are isolated to prepare for clamping. Perinephric fat is dissected to expose the renal tumor. An ultrasound probe is introduced through the assistant's port to identify the limits and depth of the tumor. The resection margin is planned and scored by monopolar cauterization. Renal vessels are clamped using laparoscopic bulldogs that are introduced by the assistant. Tumor enucleoresection is performed using sharp and blunt dissection. A laparoscopic suction instrument can be introduced through one of the previously placed assistant's ports to provide traction and suction, giving a clear view of the resection area. Renorrhaphy is performed in two layers using a modified sliding-clip technique with V-lok barbed sutures (Medtronic, Minneapolis, MN) and Hem-o-lok clips (Weck; Teleflex Medical, Research Triangle, NC). 8 After renorrhaphy is completed, the clamps are removed and hemostasis is achieved. The specimen is placed in a laparoscopic retrieval bag, which is extracted through the single-site incision. A closed suction drain is inserted through the incision under direct vision. The incision site is closed layer by layer, followed by application of a topical skin adhesive (Supplementary Fig. S2).
Statistical analysis
Statistical analysis was performed using SPSS v.22 (IBM, Armonk, NY). Continuous variables are presented as median (interquartile range [IQR]) and were compared using the Mann–Whitney U test. Fisher's exact test was used to compare categorical variables.
Results
Nine and five consecutive partial nephrectomies were performed using the SP surgical system and the XiSSP system. One patient in each group had a T1b tumor (4.4 and 5.4 cm). In four of five cases performed using XiSSP, the tumor was located in the lower aspect of the kidney, whereas the tumors using the SP system, seven of nine cases were located in the middle and upper aspects of the kidney. One tumor in the SP group had a RENAL nephrometry score of 10. The nephrometry score of all other tumors ranged from 6 to 9. The docking time was shorter with the SP system than with XiSSP (median 6 [IQR, 5–9] minutes vs 13 [9–18] minutes, p = 0.007). Console time, warm ischemic time, suture time, and estimated blood loss were comparable between groups. No patient required an intraoperative or a postoperative blood transfusion.
One case using the XiSSP system required conversion to multiport robotic surgery during tumor resection. Another case of tumor fraction occurred during resection while using the SP system; subsequent pathology revealed an angiomyolipoma. In all other cases, surgery was uneventful. The drainage tube was removed at 2 [2–3] days after surgery. The postoperative course of all patients was uneventful, with no complications greater than grade I, according to the Clavien–Dindo classification. Detailed patient demographic and perioperative outcome data are presented in Table 1 and Supplementary Table S1.
Tumor Characteristics and Perioperative Outcomes
RENAL nephrometry score (minimum 4; maximum 12).
EBL = estimated blood loss; WIT = warm ischemic time.
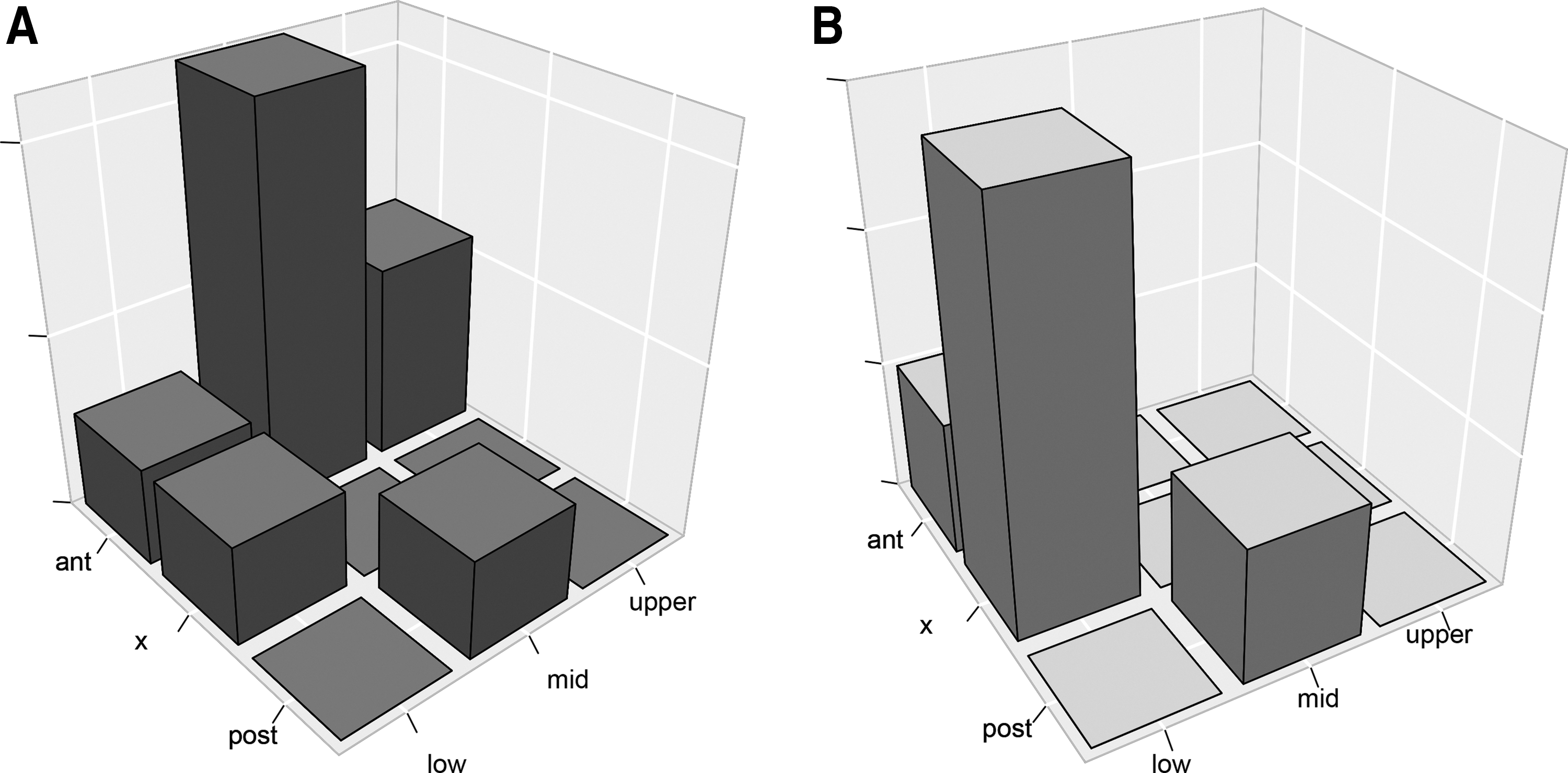
Partial nephrectomy using XiSSP system was operated mostly on tumors in the lower aspect of the kidney and none in the upper aspect. Tumors operated on using the SP system includes tumors in the upper and mid aspect of the kidney and is not restricted to tumors in the lower aspect. The distribution of tumor locations are presented in Figure 4.
Distribution of renal tumors locations for partial nephrectomy using the
Discussion
Partial nephrectomy through a single incision is now possible using the SP surgical system, which is the first purpose-built, single-port robotic platform approved for clinical use. Many of the limitations of previous single-site techniques have been overcome by the SP system.
We compared our initial experiences of robotic LESS partial nephrectomy using the new SP surgical system and the XiSSP system. All outcomes were comparable, other than docking time. However, we would like to underscore that the cases using SP surgical system were mostly in the mid and upper aspects of the kidney, whereas those using XiSSP were mostly in the lower aspects. During laparoscopic or robotic partial nephrectomy, renal tumors located in the upper pole are more challenging to operate on than tumors in other locations. 9,10 This was taken into consideration when selecting cases for partial nephrectomy with the XiSSP system, as it lacked articulating instruments and its traction strength was relatively weak. Tumor location was not an obstacle using the SP surgical system, and we were able to access upper pole tumors without difficulty. The docking time was shorter for the SP system, as docking of only one port was required. By contrast, the XiSSP system required docking of one camera and two arms.
One inadvertent intraoperative event occurred with each system. The lack of articulating scissors with the XiSSP system is a major limitation, especially during partial nephrectomy for tumor resection. This resulted in the need to convert to multiport conventional robotic partial nephrectomy in one case while using XiSSP. One case of tumor fracture occurred using the SP system for partial nephrectomy. This was attributed to the lack of a pseudocapsule, as the tumor was an angiomyolipoma, rather than to an issue related to instrument use.
The main hurdle for LESS procedures has been loss of triangulation between laparoscopic instruments, resulting in collision of instruments and mirror imaging of the operating hand and working instrument. 11 These limitations were previously resolved by the single-site platform developed for the Si and Xi da Vinci systems. The platform utilized two semirigid instruments inserted through curved cannulas, as well as programming to switch the connection between the left and right console controllers to the contralateral robotic arm. This was accomplished, however, at the expense of loss of instrument articulation, as well as a weaker traction force resulting from the use of semirigid instruments. 4 Nevertheless, this platform was a major advancement in LESS surgery, and we performed several partial nephrectomies using this single-site platform with both the Si and Xi systems. However, true single-site partial nephrectomy was not possible, as an additional port site was required for the assistant. The multichannel port for the single-site platform provides a port for the assistant, but movement of the assistant's instruments is extremely limited and not suitable for partial nephrectomy. Furthermore, an additional port is required for liver traction to expose the hilum and upper pole of the kidney in right-sided cases. The lack of articulating instruments and weaker traction force also posed limitations for upper pole tumors.
The aforementioned limitations have been resolved by the SP surgical system. An additional elbow joint allows intracorporeal triangulation, and articulation is possible with all instruments. 12 The traction force is enough to manipulate the kidney. An additional port for elevating the liver is not necessary, as one of the three arms inserted through the single-port trocar can be used for this purpose (Table 2).
Practical Comparison of the SP Surgical System and Xi Single-Site Platform
Movement of the assistant's instruments remains limited, but it is adequate to safely perform an entire partial nephrectomy. The main obstacle restricting movement of the assistant is the bulky extracorporeal configuration of the robotic arm. To bypass this limitation, multiple ports carefully placed in the GelSeal cap allow the assistant to access nearly all areas of the surgical field. Coordination between the surgeon and assistant is important, as it may be necessary for the surgeon to move the direction of the robotic arm to allow appropriate traction and suction with the assistant's instruments. Of note, it is not necessary for the arm to be directed straight at the targeted anatomy. Directing the arm at an area slightly distant from the target allows a wider range of movement for the assistant, while the articulating camera and instruments can accommodate the angulation, thereby allowing the surgeon to vision the targeted anatomy and freely manipulate the instruments. Surgeon and assistant coordination is also important because movement of the extracorporeal robotic arm can move the assistant's instruments, which may cause inadvertent organ injury, especially if the instruments were being used to support or push away a structure.
Limitations of the current study include the small number of patients enrolled in the study and the short follow-up period. Assessment of long-term oncological and functional outcomes in a larger group of patients is necessary in the future. Furthermore, the surgeon performing the procedures was highly experienced in both LESS and robotic partial nephrectomies, and initial outcomes may differ for other surgeons. There is certainly a learning curve for LESS partial nephrectomy, and our operation and ischemic times were longer than those achieved with multiport conventional robotic partial nephrectomy. However, many of the obstacles preventing LESS from gaining popularity have been resolved with the SP surgical system, and we expect the procedure time, and especially the ischemic time, to shorten as experience accumulates. Despite the learning curve, we found that partial nephrectomy with the SP surgical system can be performed safely without complications, and we plan to continue using the technique in more patients. The current report provides information to help other surgeons overcome the barriers of LESS partial nephrectomy.
In conclusion, true single-site partial nephrectomy is feasible and safe using the SP surgical system. Because of the articulating instruments and stronger traction force, it is more suitable for partial nephrectomy than the previous Xi-based single-site platform. Additional ports for the assistant or liver traction are no longer needed. The assistant's port is strategically placed in the GelSeal cap, with consideration given to movement limitations of the instruments and the need for coordination between the surgeon and assistant.
Footnotes
Acknowledgments
The authors thank MID (Medical Illustration & Design), a part of the Medical Research Support Services of Yonsei University College of Medicine, for all artistic support related to this work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Figure S1
Supplementary Figure S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.