
Abstract
Objective:
To assess the safety and efficacy of a novel vacuum-assisted access sheath (VAAS) in minimally invasive percutaneous nephrolithotomy (MPCNL).
Materials and Methods:
Seventy-five consecutive patients with single renal pelvic stone were treated with MPCNL combined with a novel VAAS. Patients' demographics and surgical outcomes, as well as perioperative and postoperative data, were recorded. Matched-pair analysis in a 1:1 scenario was done in patients who underwent MPCNL by peel-away access sheath (PAAS). All MPCNL was done with a rigid 12F mini-nephroscope and an 18F access sheath. MINDRAY-PM9000 monitor was used to record the renal pelvic pressure (RPP) data.
Results:
Patients' demographics, stone size, burden, and density (HU) were comparable between the two groups. Operative time was significantly shorter in the study group, at a mean of 32.4 ± 9.6 vs 46.2 ± 11.8 minutes (p < 0.001). The immediate stone-free rate was 89.3% for the VAAS group and 77.3% for the PAAS group (p = 0.049). Patients in the VAAS group had a lower visual analogue pain scale score at postoperative 6 and 24 hours. Mean perioperative RPP was lower in the VAAS group (10.3 ± 4.3 vs 17.8 ± 5.1 mmHg, p < 0.001). More than 50 seconds of accumulative time of high RPP (>30 mmHg) was shown in 13 patients of the VAAS group vs 30 of the PAAS group (p = 0.002).
Conclusion:
Combining VAAS with high-power holmium laser in MPCNL significantly improves the efficiency of stone retrieval with low RPP. This novel approach also reduces operative time, postoperative fever, and pain due to its simultaneous suction property.
Introduction
Percutaneous nephrolithotomy (PCNL) is recommended as the primary treatment for renal stones in size of >2 cm. 1 Minimally invasive PCNL (MPCNL), which involves use of a small access sheath (<22F), has been proved to be an alternative modality of conventional PCNL with lower risks of significant postoperative morbidity. 2 –4 However, the efficiency of stone fragments and dust extraction of MPCNL was more depressed than conventional PCNL due to its smaller access sheath, especially when treating patients with large stone burden. 4 Traditionally, stones were required to disintegrate into tiny fragments that can go through the sheath and flush out with the intermittent irrigation fluid or be removed by extractor one by one. 5
Recently, a novel and well-designed vacuum-assisted access sheath (VAAS, ClearPetra; Well Lead Medical, China) was introduced into our center. This sheath has the potential to suck out the fragments and dust due to its simultaneous suction property with continuous irrigation. Using this sheath may provide a new way of stone extraction in MPCNL.
In this study, we present the initial experience of using this access sheath in MPCNL, to assess the feasibility and safety of this sheath, as well as the efficiency of stone retrieval. To our knowledge, this is the first clinical report of this sheath.
Materials and Methods
This study was conducted between April 2017 and August 2018 after approval of the protocol by the Institutional Review Board. Written consent was obtained from all patients. Patients with the congenital renal anomaly, ureteropelvic junction obstruction, ureteral stricture, previous surgery, refractory infection, and pyonephrosis were excluded. Seventy-five consecutive patients with single renal pelvic stone who underwent MPCNL combined with VAAS were collected and compared with patients who underwent MPCNL with peel-away access sheath (PAAS; Create Medic, Japan) in a 1:1 matched-pair analysis. Matching criteria included stone size, location and laterality, gender, age, body mass index, and degree of hydronephrosis.
Stone size, location, and density (HU) were assessed preoperatively by CT scan. The stone size was measured by its largest diameter. The stone burden was obtained from data on 3D images of the stone, using 5-mm axial and 3.5-mm reconstructed coronal non-contrast CT (NCCT). We used the formula (length × width × height × π × 1/6) to calculate the stone burden. 6
The equipment used included a rigid 12F mini-nephroscope (Richard Wolf, Germany) (Fig. 1), 18F VAAS (Fig. 1) or PAAS, and a holmium laser (VersaPulse PowerSuit 100w; Lumenis, Germany).

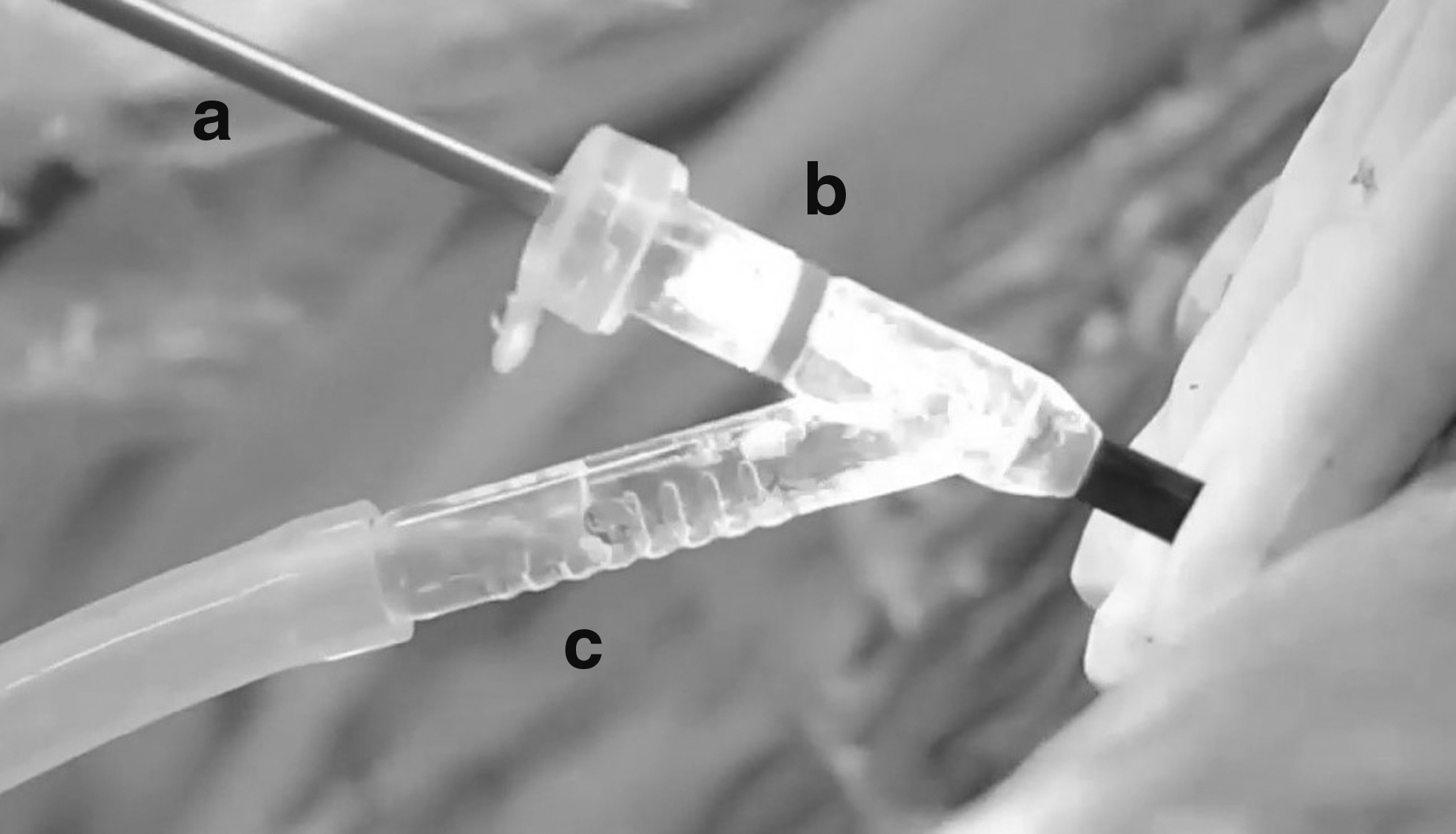
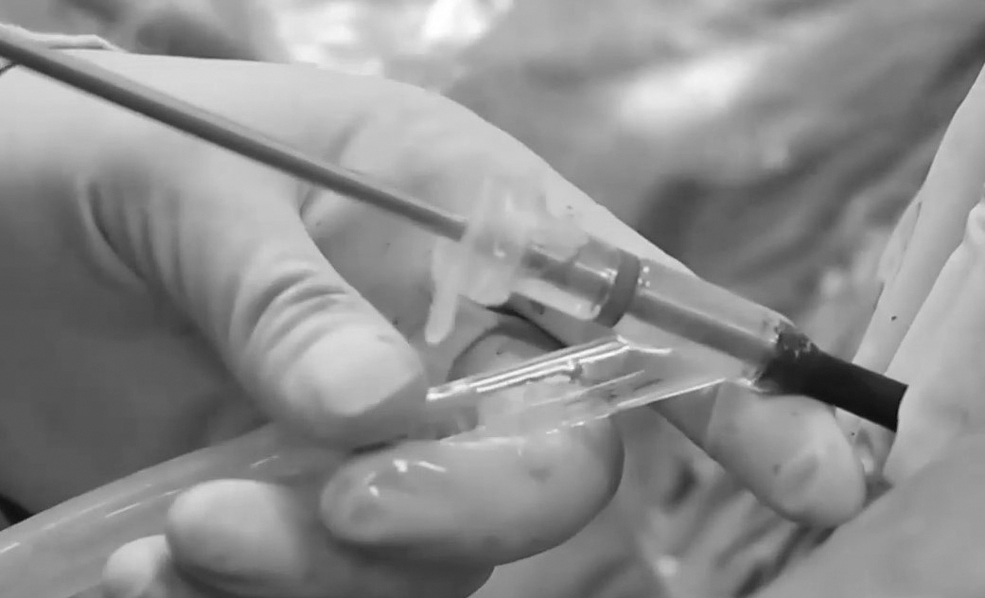
As a new disposable device, the VAAS differs from the PAAS by having an oblique egress sluice (Fig. 2). Longitudinal slit shape pressure regulating vent is located on the oblique sluice. The end of the oblique sluice was connected to the stone collecting bottle, which fits together with a negative pressure aspirator. A rubber cap with a central aperture (Fig. 1) was used to cover the straight end of the handle to achieve a closed system when inserting a mini-nephroscope into the sheath through the aperture. Irrigation fluid entered the renal collecting system through the working channel of an endoscope. Lithotripsy was done in the conventional fashion by introducing the laser fiber through the working channel of the endoscope (Fig. 3).
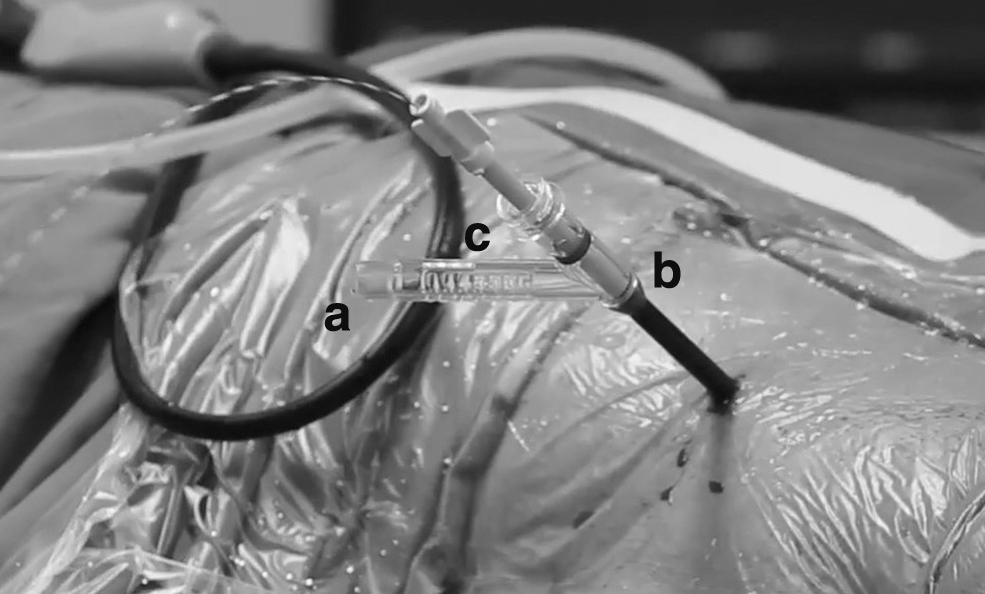

Irrigation fluid and dust were sucked out through the gap between the scope and sheath during lithotripsy and then passed through the oblique sluice to the stone collecting bottle (Fig. 3). If fragments entering the sheath were too large to cross the gap between the scope and the sheath, the urologist would withdraw the endoscope until seeing the red marker in the endoscopic vision (Fig. 4). This movement provided a non-obstructive passway for sucking out large fragments through the oblique sluice to the stone collecting bottle. The aspiration pressure could be increased by pressing the longitudinal vent if necessary (Fig. 5).
Increasing pressure by pressing the longitudinal vent.
Parenteral prophylactic antibiotics were administrated to all patients with a negative preoperative urine culture. Patients with positive urine cultures were treated with pathogen-selective antibiotics until the infection was under control. All procedures were performed under continuous epidural anesthesia. A 6F open-ended ureteral catheter was retrogradely inserted to the renal pelvis. After turning the patient into the prone position, the ureteral catheter tip was positioned at 1 cm above the ureteropelvic junction under fluoroscopic guidance and was connected to the pressure transducer in the invasive blood pressure channel of the PM9000 patient monitor (Mindray Medical Corporation, Shenzhen, China). Then, the sensor was settled onto the same level of the affected renal pelvis. After zero adjustments, continuous renal pelvic pressure (RPP) data were recorded per second. 7
The initial puncture was performed under fluoroscopic and ultrasonic guidance. We introduced either an 18F VAAS or PAAS by one-step dilatation, inspected the collecting system by a 12F mini-nephroscope, and adjusted the position of the sheath according to the stone location. The parameter of the micro-computer control (Jielun Medic, Guangzhou, China) perfusion pump was set at a pressure of 250 mmHg with an irrigation rate of 300 mL/minute. Holmium laser lithotripsy was performed in both groups by using 550 μm end-firing fiber (Lumenis), with energy set at 2 J and a rate of 20–30 Hz. In the PAAS group, stone fragments were either flushed out by pressurized irrigation fluid or removed by the stone extractor. In the VAAS group, stone fragments were aspirated. The aspiration pressure setting was 0.035 MPa. At the end of the procedure, a 6F Double-J stent was inserted anterogradely, and a 14F balloon nephrostomy tube was introduced for drainage. Operative time was measured from the time of initial percutaneous access to the removal of the access sheath.
The stone components were analyzed for each case. Low-dose renal non-contrasted CT was done on postoperative day 1 to assess the immediate stone-free rate (ISFR). Stone clearance was defined by no visible fragments in CT scanning. Patients with residuals (>4 mm) will require auxiliary procedures on postoperative day 5–7. The procedures included second-look MPCNL, extracorporeal shockwave lithotripsy, or retrograde intrarenal surgery (RIRS). After confirming clear drainage, the nephrostomy tube was removed, and the patients were discharged on the next day.
Final SFR was assessed with low-dose renal non-contrasted CT 3 months after the procedure. A visual analogue pain scale (VAS) was used to measure the degree of pain. Patients' demographics, perioperative and postoperative data, RPP, the distance between skin puncture point and target calix, operative time, complications, hemoglobin deficit, VAS, length of hospitalization, SFR, and auxiliary ancillary procedures were compared between two groups. Complications were assessed via the modified Clavien grading system.
Statistical analysis was performed by using the SPSS 22.0® software. Continuous variables were compared by using the Student t or Wilcoxon test. Discrete variables analysis was conducted by using the Pearson χ 2 statistic or Fisher's exact test for categorical data. p Values <0.05 were considered statistically significant.
Results
Demographics and stone characteristics were comparable in both groups. Positive urine culture rate was higher in the VAAS group, but the difference was not statistically significant (Table 1).
Demographics and Stone Characteristics of Patients
ASA = American Society of Anesthesiologists; PAAS = peel-away access sheath; SD = standard deviation; VAAS = vacuum-assisted access sheath.
Mean operative times were shorter for the VAAS group (32.4 ± 9.6 vs 46.2 ± 11.8 minutes, p < 0.001). There was no statistically significant difference between the two groups in terms of puncture renal calix, the distance between skin puncture point and target renal calix, fluoroscopic time, and hospitalization stay. Mean postoperative hemoglobin drop was similar in both groups, as well as preoperative and postoperative serum creatinine (Table 2).
Perioperative and Postoperative Data of Patients
RIRS = retrograde intrarenal surgery.
The immediate stone SFR was 89.3% for the VAAS group and 77.3% for the PAAS group (p = 0.049). Eight patients in the VAAS group and 17 cases in the PAAS group had residual stones. Six patients in the VAAS group and 12 patients in the PAAS group underwent second-look PCNL. RIRS was done in two patients in the VAAS group and five patients in the PAAS group. The final SFR improved to 97.3% for the VAAS group and 98.6% for the PAAS group (p = 0.56). There were no statistically significant differences in the stone compositions between the two groups (Table 2).
The complication rate via modified Clavien classification in the VAAS group was lower (16% vs 26.7%, p = 0.046). Six patients (8%) in the VAAS group experienced postoperative fever (>38°C) and required antipyretics, whereas 15 patients (20%) in the PAAS group had a similar complication (Clavien grade1). Two patients in each group had postoperative UTI (Clavien grade 2). Additional antibiotics were administered to these patients. Two patients required blood transfusion in the VAAS group and one required transfusion in the PAAS group (Clavien 2). Collecting system perforation (Clavien 3b) occurred in one patient in the VAAS group and in two in the PAAS group. They were treated with an indwelling Double-J stent for 8 weeks without sequelae. One patient in the PAAS group developed urosepsis (Clavien 4b) and was successfully treated with additional appropriate intravenous antibiotics and fluid resuscitation (Table 3).
Complications and Postoperative Pain Score
Patients in the VAAS group had a lower VAS score at postoperative 6 hours (3.3 ± 1.3 vs 5.4 ± 1.1, p < 0.001) and 24 hours (2.0 ± 0.9 vs 4.2 ± 1.2, p < 0.001). Statistically significant differences were not found after 48 hours (Table 3).
Mean RPP was lower for the VAAS group (10.3 ± 4.3 vs 17.8 ± 5.1 mmHg, p < 0.001). More than 50 seconds of accumulative time of high RPP (>30 mmHg) was observed in 13 patients of the VAAS group vs 30 patients for the PAAS group (p = 0.002) (Table 4).
Characteristics of Renal Pelvis Pressure Data
NA = not applicable; RPP = renal pelvic pressure.
Discussion
For the past decade, MPCNL has gained increasing popularity due to fewer reported complications with comparable SFR compared with conventional PCNL. 5,8 However, this technique has compromised operative efficiency and requires higher perfusion pressure. Stones are required to disintegrate into tiny fragments by either pressurized irrigation or stone extractor, to be removed through the smaller diameter access sheath. Allegedly, it results in prolonged operative time and high RPP. 8 –10 In this study, the use of VAAS in MPCNL showed the advantage of reducing the operative time and complications, along with the improved SFR and RPP.
During MPCNL, stone fragment and extraction is the most time-consuming step, especially when treating patients with large burden renal stones. In this study, we used the same high-power holmium laser (HP-HLL) and performed MPCNL on two groups of patients with comparable stone characteristics. Of note, mean operative time in the VAAS group was 29.9% shorter than in the PAAS group. The usage of VAAS was attributable to this improvement. In MPCNL with VAAL involved, small clots and dust could be simultaneously sucked out through the gap between the scope and sheath during lithotripsy during stone pulverization. A clearer vision was achieved during the procedure. Less time was spent on identifying the renal collecting system anatomy and chasing the residual stones.
Also, VAAS connected to a negative pressure aspirator facilitates the removal of stone fragments. Urologists can actively withdraw the endoscope to open a non-obstructive passway for sucking out the larger fragments. A size of near about 5-mm stone can be sucked out through the 18F VAAS. Less utilization of graspers or forceps was found in most of the cases.
Suction technique has been applied in the conventional PCNL device. Successful models in ultrasonic lithotripsy (US-L), such as Cyberwand and Swiss EMS, combined ultrasonic energy with suction technique. It has been reported that using these expensive devices can significantly increase the surgical effectiveness with shorter operative time due to its simultaneous suction property of tiny stone fragments.1112 However, the suction potential of these devices is achieved by the hollow lumen structure of the US-L probe. The small size of the probe tremendously affects the outcome of removing the fragments. Only the stone <3 mm in diameter can be sucked out.
In a previous randomized study, El-Nahas et al. compared the clinical outcomes between the US-L method and the HP-HLL method. 13 Small fragments from both procedures can be simultaneously removed from the kidney in different ways, that is, active aspiration in US-L and irrigation in HP-HLL. They found that HP-HLL showed comparable SFR in treating staghorn stone but only longer operative time when compared with US-L. 13 In this study, we integrated VAAS with HP-HLL in the treatment of renal pelvic stone. VAAS is a disposable and simple modification access sheath that has an oblique egress sluice for aspirator connection, but it markedly improved the surgical effectiveness of the HP-HLL method. Sufficient stone clearance and shorter operative time were achieved. In this study, we were unable to directly compare the outcomes of our novel technique with the ones of the US-L method. It is of interest to study and it is highly possible that this novel approach has higher efficiency than US-L.
In this study, we found that combined VAAS with continued pressure aspiration had lower RPP and the potential of reducing pressure-induced complication. RPP >30 mmHg has been shown to result in pyelovenous lymphatic backflow. It can lead to systemic absorption of bacteria or endotoxin-containing irrigation fluid and result in systemic inflammatory response syndrome or even urosepsis. Mean RPP of the PAAS group here was comparable to Zhong's study, 10 which was significantly higher than the VAAS group. But the mean RPP in both groups was less than 30 mmHg. Both suction and “vacuum-cleaner” methods performed well in controlling mean RPP.
We demonstrated that RPP has a transient increase in the PAAS group. Therefore, more caution is necessary when using pressurized irrigation to wash out the stone fragments. Forty percent of patients in the PAAS group had a long accumulated time of high RPP (>50 seconds). Interestingly, 17% of the VAAS group cases also had a long accumulated time of high RPP. This may be attributable to the stone position. All stones here were single renal pelvic stones. The direct high-pressure fluid from the mini-nephroscope influences the RPP primarily during the stone fragmentation and retrieval, as the ureteral catheter with the sensor for the pressure observation was placed in the renal pelvic area.
Some other reasons should also be taken into consideration. During the stone fragmentation, dust can be actively sucked out through the interspace between the sheath and the mini-nephroscope; temporarily high RPP was still recorded when tiny fragments obstructed this space. This situation can be solved by the withdrawal of the mini-nephroscope back to the red line marker to open up an unimpeded passage. In addition, we still got a higher record of RPP with VAAS, when the access sheath was torqued to reach a renal calix that was not in the straight line or when the mini-nephroscope went through a narrow infundibulum.
Prolonged operative time, high RPP (>30 mmHg), and long accumulated time of high RPP (>50 seconds) are risk factors for postoperative fever. 10 Alsyouf et al. demonstrated that patients who were exposed to high RPP during PCNL had significantly higher postoperative pain scores. 14 High RPP stretches the collecting system and stimulates the nociceptors located in the peripelvic renal capsule, leading to pain in the kidney area. 14 It is also possible to cause perforation of the collecting system, resulting in urine extravasation among retroperitoneum.
In this study, 20% of patients in the PAAS group had fever, which was comparable to the previous PCNL study for staghorn stones. Only 6% of patients had postoperative fever in the VAAS group. Patients in the VAAS group also had lower postoperative pain scores at postoperative 6 and 24 hours. These results suggest that the risk factors for postoperative fever and pain were managed better by using VAAS. The stable low RPP during MPCNL was maintained by a balance between suction and irrigation. The active vacuum suction design facilitates the removal of different sized fragments from either the gap between the sheath and the endoscope or the lumen of the sheath. Combined HP-HLL and this vacuum technique significantly shorten the operative time.
This study has some limitations. First, this study is its non-randomized design. Second, this is a single-center study with a relatively small number of patients and a short follow-up. A multi-center prospective randomized study with a larger sample size and longer time of follow-up would further warrant current findings.
Conclusion
Combining VAAS with high-power holmium laser in MPCNL significantly improves the efficiency of stone retrieval with low RPP. This novel approach also reduces operative time, postoperative fever, and pain due to its simultaneous suction property.
Footnotes
Acknowledgment
The authors thank Dr. Liang Xiao from Vanderbilt University Medical Center for proofreading the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.