
Abstract
Objective:
The aim of this study was to introduce the “ultrathin parenchyma” resection in a robot-assisted partial nephrectomy (RAPN) via the retroperitoneal approach, and to assess the feasibility, security, and effectiveness of this technique.
Methods:
We collected and retrospectively reviewed the clinical data of patients with renal tumors who underwent ultrathin parenchyma resections in RAPNs via the retroperitoneal approach or traditional sharp dissection in RAPNs via the retroperitoneal approach from February 2015 to August 2018. The general data and other parameters, such as the operation time, blood loss (BL), warm ischemia time (WIT), positive surgical margin (PSM), glomerular filtration rate (GFR), and postoperative recurrence, were compared and analyzed between the two surgical techniques.
Results:
In ultrathin parenchyma resection groups, one case was converted to an open surgery, while the other cases were completed effectively. There were no significant differences in the general data, operation time, intraoperative BL, WIT, intraoperative complications, transfusion rate, PSM rate, hospital stay, and recurrence rate after the operation between the two groups (p > 0.05). The postoperative residual kidney volume percentage and the GFR (6 months postoperatively) were significantly higher in the ultrathin parenchyma resection group when compared with the traditional sharp dissection group (p < 0.05).
Conclusion:
The ultrathin parenchyma resection during robotic partial nephrectomy (RPN) is a safe and effective surgical technique for the resection of cT1 renal tumors. It can preserve the renal function under the premise of ensuring effective tumor control.
Introduction
The robot-assisted partial nephrectomy (RAPN) has more significant advantages than the open partial nephrectomy and the traditional laparoscopic partial nephrectomy in terms of perioperative indicators. 1 Similar to the concept of “trifecta” in evaluating the outcome of prostate cancer, Carneiro et al. use “trifecta” as surrogate markers to evaluate the efficacy of partial nephrectomy, which is defined as warm ischemia time (WIT) ≤25 min, no positive surgical margin (PSM), and complications ≤Clavien II, and their studies also indicate that RAPN has obvious advantages in the treatment of complex renal tumors. 2,3
The “push-cut” technique, or named as the “Ultrathin parenchyma” resection, which is used during the robotic partial nephrectomy (RPN), is originally performed in our center, and it can resect the tumor in entirety by leaving an ultrathin layer of normal tissue, about 0.2 cm, outside of the tumor pseudocapsule, thus avoiding PSM and greatly protecting the renal function. In this study, we retrospectively included 130 patients who underwent the ultrathin parenchyma resection or the sharp dissection during RAPN in our center, and compared the relative parameters of the two methods to evaluate the feasibility and safety of the ultrathin parenchyma resection.
Patients and Methods
Clinical data
We collected the data from 130 patients who underwent RAPNs via the retroperitoneal approach at our center from February 2015 to August 2018. Of these 130 cases, 63 patients underwent ultrathin parenchyma resections, and the other 67 patients underwent traditional sharp dissection. All of the cases met the inclusion criteria, including a single tumor and cT1 clinical staging. All of the operations were completed by the same surgical team. The clinical data and R.E.N.A.L (radius, exophytic/endophytic properties, nearness to the collecting system or renal sinus, anterior/posterior, and location relative to the polar line) scores of the renal tumors are shown in Table 1.
Clinical Data and R.E.N.A.L Scores in Two Groups
The renal GFR was measured with 99mTc-DTPA.
ASA = American Society of Anesthesiologists (ASA) Score; BMI = body mass index; GFR = glomerular filtration rate.
Surgical methods
Operative indications
The clinical stage was a cT1 renal neoplasm with a single tumor.
Preoperative preparation
The renal functions of the affected and healthy sides were evaluated, including the total and partial renal functions, routine electrolyte detection of the renal function, glomerular filtration rate (GFR), and renal plain scan plus enhanced CT and CT angiography examinations. A color Doppler ultrasonographic examination of the abdominal wall vessels was used to determine whether there were venous tumor thrombi. An abdominal color Doppler ultrasonographic examination and a chest CT were used to detect metastases. An indwelling catheter was placed before the operation.
Anesthesia
Each of the patients underwent general anesthesia with endotracheal intubation.
Surgical instruments
The surgical instruments used in the operations were as follows: 30° laparoscopy, fenestrated bipolar clamp, monopolar scissors, one robotic needle holder, two 8-mm manipulator metal casings, two 12-mm ordinary casings (or one 12-mm ordinary casing plus one 12-mm lengthened casing), bulldog vascular clamp, 3-0 barbed absorbable line (RB-1 sewing needle), and 1-0 barbed absorbable line (CT-1 sewing needle).
Patient position
The patient was placed at 90° full flank position with the operating side facing upward.
Trocar configuration
Four ports were adopted, including one camera port, two robotic arm ports, and one assistant port (Fig. 1A).

Patient position, trocar configuration, and OR setup for robotic partial nephrectomy via retroperitoneal approach.
Robotic cart docking and operation room configuration
The robotic cart was docked over the head.
Ultrathin parenchyma resection procedures
The ultrathin parenchyma resection was performed as follows (Fig. 2): (1) Trocars were placed after the retroperitoneal cavity was established, and the retroperitoneal fat was dissociated for better operative field, when excessive adipose tissue was filled in the extraperitoneal space beside the iliac fossa to avoid visual interference. (2) The Gerota fascia was incised obliquely along the psoas major muscle direction, upper to the subphrenic and down to the upper edge of the iliac fossa, fully exposing the kidney. (3) The renal separation was performed along the deep side of the psoas major, exposing the psoas major muscle and the medial arcuate ligament (MAL) at the junction between the psoas major muscle and the diaphragm. The renal pedicle was exposed according to the marks such as the diaphragm, the medial margin above the psoas major muscle, the MAL, and the renal artery pulsation. Then the renal arterial sheath was cut, and the renal artery was adequately dissociated. (4) The renal adipose capsule was cut open, and the location of the renal tumor was determined according to the preoperative CT scan. The tumor and its surrounding renal parenchyma were fully exposed, and the adipose tissues on the surface of the renal tumor had to be preserved to be removed together with the tumor. (5) The renal artery was blocked using a bulldog vascular clamp, and the ischemic time was recorded, which should be less than 30 min. Before blocking the renal artery, creatinine (1 g) was quickly intravenously injected to protect the renal function. (6) An electric scissor was used to make a circular excision line between the tumor border and the normal tissue using electrocoagulation. Tumor enucleation was performed using a push-cut technique, the ultrathin parenchyma resection, by leaving a 0.2 cm normal tissue capsule around the entire tumor. Intraoperatively, the thickness of parenchyma is confirmed by a clear visualization of the tumor pseudocapsule through the overlying transparent parenchymal tissue. The tumor pseudocapsule should not be cut open and the tumor was removed in entirety. The hemorrhage of the small vessels was blocked by electrocoagulation with monopolar scissors or fenestrated bipolar. The hemorrhage of the larger vessels and the injured renal collecting system were blocked by suture or Hem-o-lok clip. The contact between the Hem-o-lok clip and the collecting system's mucosal surface should be avoided. (7) The base of the renal parenchymal defect was continuously sutured using 3-0 barbed suture on RB-1 needle. Then, the blood supply of the kidney was restored by removing the vascular clips, and not bleeding was confirmed. The renal parenchymal defect was closed using 1-0 barbed suture on CT-1 needle 3-0 barbed suture. (8) The tumor samples were placed into a specimen bag. The blood on the field was removed using an aspirator, and the renal surface was washed with distilled water. A drainage tube was placed via a routine ventral puncture hole. Finally, the specimens were taken out and all of the incisions were closed.
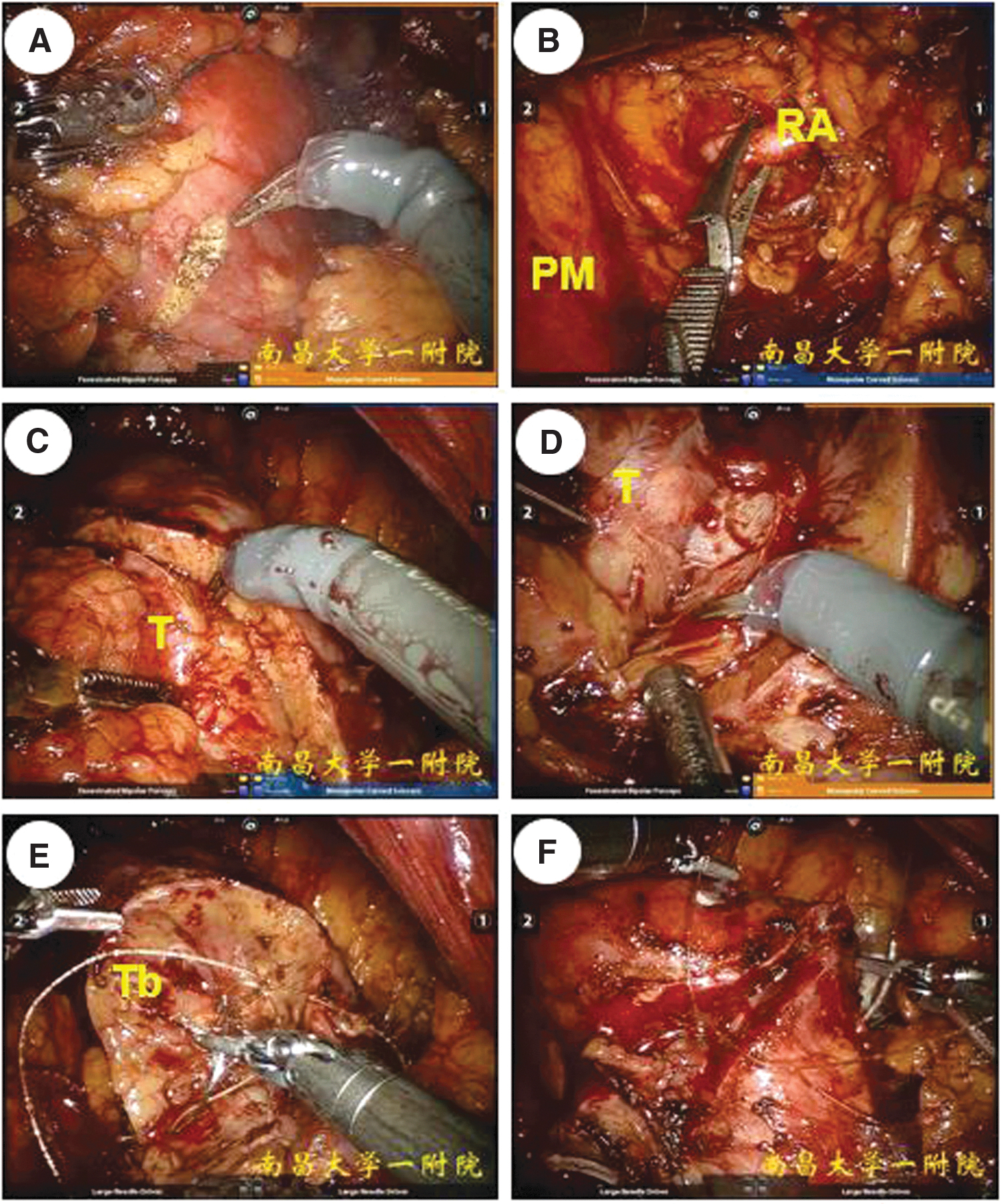
Surgical techniques of robotic partial nephrectomy via retroperitoneal approach.
Traditional sharp dissection procedure
During the tumor sharp dissection procedure, the normal tissues, which were greater than 0.5 cm thick, were left on the tumor surface. The other steps were the same as those in the ultrathin parenchyma resection procedures described above.
Tumor samples
The smaller tumors were taken through the camera port. For larger tumors, the assistant port was obliquely inward extended and the tumors were taken through the assistant port. Tumor samples were fixed, stained with ink, embedded in paraffin, and cut into 5 mm sections followed by the staining and observation under a microscope. The PSM criteria were the broken of the tumor pseudocapsule or the presence of tumor tissue on the outer margin of the ink staining.
Parameters of evaluation
The main relevant parameters were the operation time, intraoperative blood loss (BL), WIT, intraoperative complications, blood transfusion rate, PSM rate, hospital stay, GFR at 6 months postoperative, postoperative recurrence, and the percentage of residual kidney volume. The percentage of residual kidney volume was calculated by the following formula: the percentage of residual kidney volume = renal volume postoperation/renal volume before operation. 4 The renal volume postoperation and renal volume before operation were measured by the same radiologist.
Statistical analysis
All of the data were analyzed using SPSS 20.0 software. The data conforming to a normal distribution were presented as mean ± standard deviation, while the data not conforming to a normal distribution were presented as median (range). The differences among groups were compared using the Student's t-test. A p-value less than 0.05 indicated statistical significance.
Results
The baseline clinical characteristics and R.E.N.A.L scores between the two groups
The results showed that there was no significant difference in the age, body mass index, American Society of Anesthesiologists (ASA) Score, preoperative ipsilateral GFR, maximum diameter of the tumor, and R.E.N.A.L score between the ultrathin parenchyma resection group and the traditional sharp dissection group (p > 0.05, Table 1).
The operative and prognostic parameters between the two groups
In the ultrathin parenchyma resection group, one patient was converted to an open surgery due to the severe perirenal adhesions and the difficulty of separation. Other patients effectively completed the RPN operation. As shown in Table 2, there was no significant difference in the operation time, WIT, intraoperative BL, blood transfusion rate, postoperative hospital stay, PSM rate, postoperative complications, and postoperative recurrence between the two groups (p > 0.05). The percentage of residual kidney volume at 6 months postoperatively in the ultrathin resection group was significantly higher than that in the sharp dissection group (77% ± 5.8% vs 72% ± 6.4%, p < 0.05). The ipsilateral GFR at 6 months postoperatively in the ultrathin resection group was significantly higher than that in the sharp dissection group (36.47 ± 3.82 mL/min vs 30.23 ± 3.96 mL/min, p < 0.05). The decrease of ipsilateral GFR during the 6 months was lower in the ultrathin resection group than that in the sharp dissection group (11.48% ± 3.05% vs 20.53% ± 4.61%, p < 0.001).
Clinical Data and R.E.N.A.L Scores in Two Groups
The renal GFR was measured with 99mTc-DTPA. △GFR6 = (1 − GFR6/GFR) × 100%.
SD = standard deviation.
The histopathologic subtype statistics showed 112 clear cell carcinoma cases (54 cases in the ultrathin resection group and 58 cases in the sharp dissection group). The remaining subtypes were hamartomas, papillary carcinomas, eosinophilic cell tumors, and cystic renal cell carcinomas (Table 2). There was no significant difference in the proportion of clear cell carcinoma between the two groups (p > 0.05).
There was no postoperative delayed bleeding or urine leakage complication in the two groups. There was no statistical difference in follow-up between the two groups.
During an average follow-up of 10 months (range from 6 to 17 months), no local recurrence or distant metastasis was seen.
Discussion
RAPN has many advantages, such as special oncologic characteristics and the effective protection of renal function. Therefore, it has become a favorable choice for many surgeons and patients. 5 In the treatment of renal tumors, the better protection of renal function has always been a key issue. 6 Although many assistive methods, such as cold ischemia, selective renal artery clamping, renal parenchymal clamping, and superselective embolization, have effects on protecting renal function, they also have their limitations. 7 In terms of long-term renal function protection, preserving as many nephrons as possible is more important than shortening the WIT under the premise of ensuring an effective range WIT, 8,9 because the long-term renal function mainly depends on the retention of effective nephrons. 10 Nephron-sparing nephrectomy can be roughly divided into three types, 11 –13 a sharp dissection with a distance more than 0.5 cm from the margin of the incision to the tumor pseudocapsule, a tumor enucleation with the greatest degree of preservation of the healthy renal parenchyma (separating along the tumor pseudocapsule and preserving all the renal parenchyma with a normal appearance), and an ultrathin parenchyma resection proposed by our center (tumor separation was performed ∼0.2 cm away from the tumor pseudocapsule by adopting the combination of blunt and sharp separation) (Fig. 3). There is no significant difference in the progression-free survival rate and tumor-specific survival rate between the sharp dissection and tumor enucleation, while the latter displays significant advantages with regard to the operation time, WIT, collective system integrity, and renal parenchyma preservation. 14,15 However, because the incidence of the pseudocapsule invasion of malignant renal tumors can be as high as 70% to 81%, and 15% to 25% of them break through the capsule and invade the renal parenchyma, patients undergoing tumor enucleation will be exposed to a higher risk of residual tumor. 16 To juggle the complete removal of the tumor and the preservation of the renal function, we proposed the ultrathin parenchyma resection in RPN with a preservation of the normal renal parenchyma of ∼0.2 cm in the current study.

A 54-year-old male bearing a 4.8 × 4.5 mm solid mass
In the present study, the ultrathin parenchymal resection during RAPN was safe in the cases. Our results showed that there was no significant difference in the low PSM rate (0%), intraoperative and postoperative complications, and postoperative recurrence, between the ultrathin resection group and the sharp dissection group. In addition, there was no significant difference in the WIT, an important parameter closely related to perioperative renal function alterations, 17 between the two groups. In terms of long-term renal function protection, the ultrathin parenchyma resection showed a higher percentage of residual kidney volume and less reduction in the renal function when compared with the sharp dissection group. We designed a model for roughly calculating the more preserved nephrons by the ultrathin parenchyma resection than the sharp dissection before operation, based on the ratio of the tumor diameter to the intrarenal tumor volume (Fig. 4). When compared with tumor enucleation preserving the healthy renal parenchyma at the greatest degree, the ultrathin parenchyma resection removed kidney parenchyma of ∼0.2 cm (Fig. 5A, B), establishing a barrier to the renal capsule partially invaded by the tumor (Figs. 5B and 6).

A 41-year-old male bearing a 4.8 × 4.3 mm solid mass
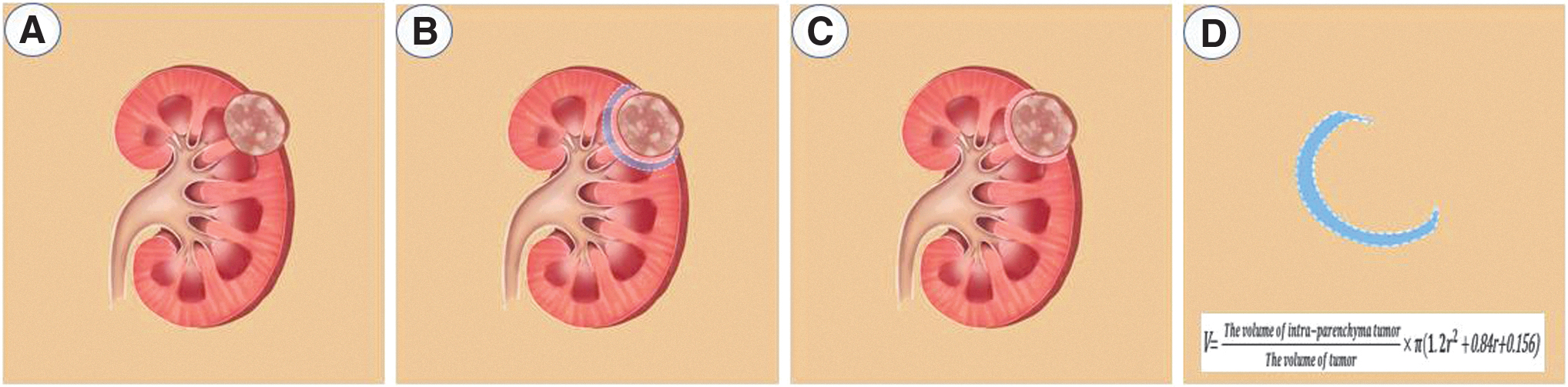
“Ultrathin parenchyma” renal tumor resection model and normal renal parenchyma compared with sharp dissection.
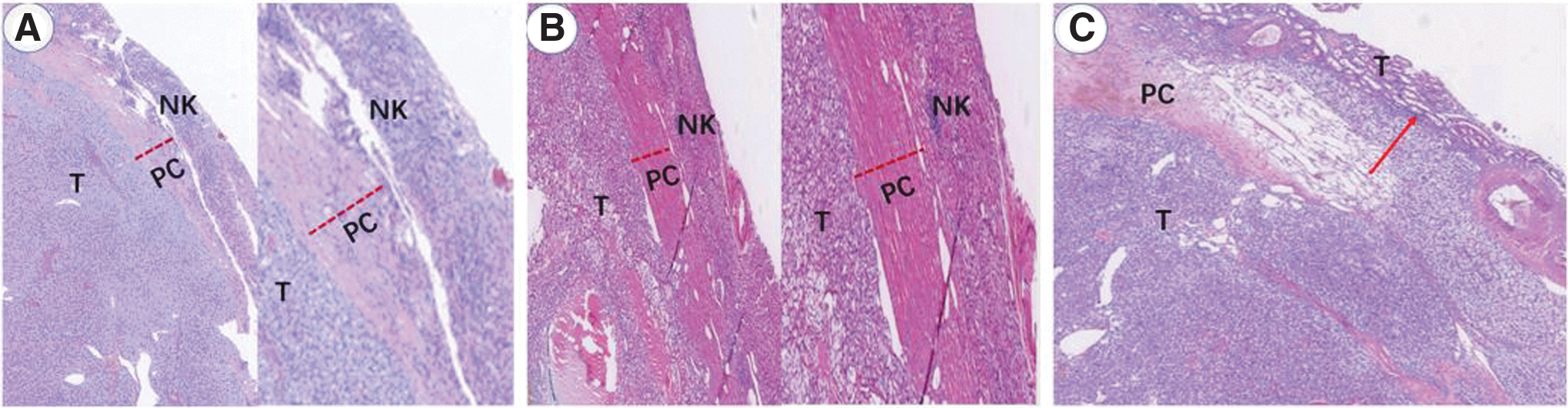
Renal tumor HE staining.
On the basis of skilled mastery of laparoscopy and RAPN via the retroperitoneal approach, the ultrathin parenchyma resection during RAPN can be attempted. With regard to the ultrathin parenchyma resection technique, we have summarized the following experiences. The first is the grasp of surgical indications. With the widespread application of surgical robots and the improvement of surgical techniques, there was no clear definition of the tumor size and location in the indication for the nephron-sparing partial nephrectomy. The ultrathin parenchyma resection technique is theoretically applicable to all renal tumors with pseudocapsule. Nevertheless, because the tumor separation is close to the tumor pseudocapsule, the risk of capsule rupture is higher for the patients with wider tumor basements. In view of this, it is advisable to select patients with small tumors during the initial stages of attempting this technique. The second is the exposure of the surgical field. The key of this surgical technique is to close the tumor pseudomembrane and adopt the combination of blunt and sharp separation to resect the tumor, which requires a high clearness of the surgical field. Thus, the cooperation of the robotic assistant is particularly important and the skilled cooperation can fully expose the separation plane to ensure a smooth push-cut operation. The effective hemostasis is also helpful for exposure of the surgical field. Generally, unipolar and bipolar coagulations are effective methods for small arterial or venous hemorrhages, and suturing is the most reliable method for massive venous hemorrhage. The third is the selection of the surgical approach. It is known that an RPN can be performed via a transperitoneal or a retroperitoneal approach. The superiority of the former approach lies in the large operational space, clear anatomical markers, and a better exposure of the abdominal vessels. The advantage of the latter approach lies in a more direct and rapid exposure of the renal artery, the obvious effect of gas pressure hemostasis, no need for the dissociation or blocking of the renal veins, and avoiding the interference to the abdominal organs and the interference of the abdominal organs on the surgical field. Some researchers believe that the transperitoneal approach is suitable for large or completely ventral kidney tumors, while we have safely and effectively completed the procedure for kidney tumors more than 7 cm and completely ventral kidney tumors via the retroperitoneal approach. Taken together, our experience of the ultrathin parenchyma resection indicates that the correct separation plane and the skillful cooperation of an assistant are particularly important.
In summary, the results of our study suggest that on the premise of strictly grasping the operation indication and correctly implementing the procedure, the ultrathin parenchyma resection can ensure effective tumor control and preserve the renal function in comparison with the traditional sharp dissection. Therefore, it is a safe and effective surgical technique for the resection of cT1 renal tumors. Moreover, with the accumulation of experience, our team has carried out the technique of “ultrathin parenchyma resection with off-clamp of renal pedicle” and the preliminary clinical results confirmed that this technique is effective and feasible. However, this technique is more difficult and the indications are relatively narrower. The data of this technique are still in the collation, waiting for publication in following studies.
Ethical Approval and Consent to Participate
The Ethics Committee of the First Affiliated Hospital of Nanchang University approved this study. Patients' informed consent was obtained verbally over the telephone and was recorded during phone calls (verbal and recorded consent was approved by the ethics committee of our institution); the patients received an information letter before the informed consent; informed consent to participate in the study was recorded on the phone calls; and patient's identity, answers, and information on medical records were kept confidential.
Consent for Publication
The authors declare that they have obtained consent to publish the identifying information (individual details, images, or videos) contained in this article.
Availability of Data and Material
The data sets generated and/or analyzed during the current study are not publicly available due [follow-up research needs protection], but are available from the corresponding author on reasonable request.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the National Natural Science Foundation of China (grant no. 81860454) and the Jiangxi Provincial Science and Technology Program (grant no. 20181BAB205053). The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the article.