
Abstract
Background and Purpose:
In this study, we evaluated the effectiveness and safety of photodynamic diagnosis (PDD) of upper urinary tract carcinoma (UTUC) using oral 5-aminolevulinic acid (5-ALA).
Materials and Methods:
Consecutive adult patients with suspected UTUC based on imaging and urine cytology findings were prospectively enrolled from May 2018 to January 2019. 5-ALA (20 mg/kg) was orally administered 2 to 3 hours before diagnostic ureteroscopy (URS). Sixty-three biopsy samples were collected from 20 eligible patients using white light (WL) and PDD-URS. The primary endpoint was sensitivity, and the secondary endpoints were specificity, positive predictive value (PPV) and negative predictive value (NPV), diagnostic accuracy, and safety.
Results:
The sensitivity of photodynamic URS was significantly higher than that of WL-URS (93.8% vs 62.5%, p = 0.0025). Although the specificity and PPV were not different between the two procedures, PDD-URS showed a significantly higher NPV (92.3% vs 69.2%, p = 0.027) and accuracy (0.86 vs 0.75, p = 0.0297) than WL-URS. With respect to safety, no grade ≥3 adverse events related to 5-ALA administration occurred in any patients.
Conclusion:
We found that PDD-URS with oral 5-ALA is a safe and superior diagnostic tool for detection of UTUC compared with conventional WL-URS.
Introduction
Upper urinary tract carcinoma (UTUC) accounts for ∼5% to 10% of all urothelial carcinomas (UCs). 1 Although the gold standard treatment in most patients with UTUC is radical nephrectomy, nephron-sparing surgery (NSS) is a treatment option for selected patients with low-grade and/or low-stage unifocal tumors to preserve renal function. 2 –4 When selecting patients for NSS, diagnostic ureteroscopy (URS) with or without biopsy provides useful information including tumor architecture, grade, and stage. 5 However, one study demonstrated that tumor lesions were missed in up to 25% of patients by diagnostic URS. In particular, flat lesions such as carcinoma in situ (CIS) were missed in ∼50% of these patients. 6 Therefore, novel imaging techniques are required to improve diagnostic accuracy when performing endoscopic evaluation.
Narrow-band imaging technology, which filters white light (WL) into specific light wavelengths that are absorbed by hemoglobin, has recently become readily available as a modality to enhance the diagnostic accuracy of tumors in the bladder and upper urinary tract. 7,8 Moreover, photodynamic diagnosis (PDD) using 5-aminolevulinic acid (5-ALA) or hexyl aminolevulinate as a photosensitizer has also been used in patients with UC of the bladder, which improves detection of the tumor lesion with a higher sensitivity of >90% compared with WL evaluation. 9,10 In particular, the PDD-guided procedure significantly improves detection rates of CIS lesions in the range of 23% to 78%. 11 To date, however, only a few single-center series have focused on the utility of PDD-URS for detecting UTUC. 12 –15 In addition, no well-designed prospective studies have been published. 16 Therefore, this prospective clinical trial was performed to compare the clinical superiority of detecting UC between PDD-URS using oral 5-ALA and conventional WL-URS in patients with suspected UTUC. The safety of 5-ALA used as a photosensitizer was also evaluated.
Materials and Methods
Ethics statements
This prospective single-arm clinical trial was registered with the University Hospital Medical Information Network (UMIN000035166) on May 1, 2018. This study was approved by the ethics board of Kansai Medical University (IRB No. 2017270), and all patients provided written informed consent.
Patient selection
From May 2018 to January 2019, adult patients (≥20 years old) with suspected UTUC were assessed according to the inclusion and exclusion criteria of this study. The inclusion criteria were as follows: (1) a tumor lesion in the upper urinary tract detected by imaging (CT/MRI) with negative urinary cytology, (2) positive or suspicious urine cytology with no suspicious tumor lesion in either the upper urinary tract or bladder, and (3) a plan to perform ureteroscopic treatment or follow-up URS after endoscopic surgery. The exclusion criteria were as follows: (1) a tumor lesion with positive urinary cytology requiring immediate radical nephrectomy, (2) suspected UTUC with a concomitant significant bladder tumor requiring transurethral resection of the bladder, (3) current or previous hypersensitivity to porphyrins, (4) definite or possible pregnancy or currently breastfeeding, (5) refusal to participate in the study, and (6) ineligibility for medical, psychologic, or other reasons as judged by the investigator.
Investigational agent and apparatus
Each patient was orally administered 20 mg/kg of 5-ALA (SBI Pharmaceuticals Co., Tokyo, Japan) dissolved in 50 mL of water 2 to 3 hours before URS. 17 All URS procedures were performed by one experienced endourologist (T.Y.). The PDD system used in this study was a D-Light C® (Karl Storz, Tuttlingen, Germany) with a removable protoporphyrin IX excitation eyepiece filter permitting blue-violet light (BL) (380–430 nm). The ureteroscopes used in this study were the URF-P6® (Olympus, Tokyo, Japan) and the Ultrathin® 6-Fr (Richard Wolf, Knittlingen, Germany). The Endoflow II pump was used with the TraxerFlow irrigation system (Rocamed, Monte Carlo, Monaco) to achieve a steady continuous irrigation pressure. The Piranha® (Boston Scientific Corporation, Marlborough, MA) was used as ureteroscopic biopsy forceps.
URS procedure
Each procedure began with observation of the ureter using a semirigid ureteroscope to evaluate the presence of urinary tract abnormalities (standard WL-guided cystoscopy was performed in all patients at an outpatient clinic before URS). A flexible ureteroscope (f-URS) was then inserted to the renal pelvis (if possible) using a guidewire with a fluoroscope. After reaching the renal pelvis, the guidewire was removed. The upper urinary tract, from the renal calices and pelvis to the distal ureter, was mapped first under WL and subsequently under BL for PDD. Biopsies were taken from all suspicious lesions detected by WL-URS, PDD-URS, or both. If no suspected lesions were detected, at least two random biopsy specimens were obtained from the normal-looking mucosa of the renal pelvis and ureter. After the operation, all patients were instructed to avoid exposure of their eyes and skin to strong light sources, such as direct sunlight or brightly focused indoor light, for 24 hours.
Evaluation
Clinical variables
Age; gender; body mass index; history of bladder cancer; voiding urine cytology (negative/suspicious/positive); imaging characteristics based on preoperative CT or MRI such as tumor side (right/left), tumor size, tumor location (renal pelvis/ureter/undetected), and clinical tumor stage; and number of biopsies were collected.
Endoscopic evaluation
The tumor appearance as shown by WL-URS was stratified into two types: no apparent tumor, which was WL-URS negative (normal mucosa or irregular flat lesion ± redness), and apparent tumor, which was WL-URS positive (papillary or sessile tumor). The PDD-URS appearance was evaluated according to whether the suspected lesion significantly glowed red (PDD-URS positive) or not (PDD-URS negative). Representative endoscopic images used for judgment are shown in Figure 1. The judgment was determined by two urologists (T.Y. and T.I.) intraoperatively. To prevent false-positive PDD due to tangential artifact, the f-URS was invariably bent to vertically observe such lesions.

Representative images of WL-URS and PDD-URS. Upper row: no apparent tumor (WL-URS negative: normal mucosa/irregular flat lesion). Lower row: apparent tumor (WL-URS positive: papillary/sessile tumor). Arrow indicates PDD-positive lesion. PDD-URS = photodynamic diagnostic ureteroscopy; WL-URS = white light ureteroscopy.
Pathologic evaluation
The biopsy specimens were fixed in formalin immediately after obtaining them. All specimens were reviewed by expert uropathologists. The tumor stage and tumor grade were evaluated according to the 2010 American Joint Committee on Cancer TNM staging system and the 2016 World Health Organization consensus classification, respectively. 18,19 For benign tissue, we discriminated the pathologic findings as normal mucosa, inflammatory change, or dysplasia. 19
Endpoints
The primary endpoint was sensitivity. The secondary endpoints were specificity, positive predictive value (PPV), negative predictive value (NPV), and diagnostic accuracy. For the safety analysis, adverse events (AEs) were evaluated according to the Common Terminology Criteria of Adverse Events v4.0 within 7 days after administration of the agent regardless of the presence or absence of a causal relationship with the agent.
Sample size
The sample size was calculated based on the largest retrospective study to date that investigated the utility of PDD-URS for UTUC. 15 The reported sensitivities of PDD-URS with 5-ALA and WL-URS are 95.8% and 53.5%, respectively. Thus, 21 samples were required with a significance level of 5% and a power of 80% using McNemar's test. When considering a possible dropout rate of 20% and an insufficient pathologic material rate of 30%, 33 samples were required. Therefore, 20 patients (at least 40 samples) were considered adequate in this study.
Statistical analysis
All continuous data are shown as median and interquartile range. McNemar's test, the chi-square test, and the area under the receiver operating characteristic curve (AUC-ROC) were used to assess the endpoints. All statistical analyses were performed using EZR version 1.37 (Saitama Medical Center, Jichi, Japan). 20 A two-sided p-value of <0.05 was considered statistically significant.
Results
Study population and patient characteristics
The patient selection process for this study is shown in Supplementary Figure S1. Twenty-one patients met the exclusion criteria, and the remaining 20 patients underwent diagnostic URS and were analyzed. The patients' characteristics are given in Table 1. Of 69 biopsies obtained in this study, 6 (8.7%) had insufficient material for pathologic evaluation. Thus, 63 biopsies taken from the renal pelvis (n = 42, 66.7%) and the ureter (n = 21, 33.3%) were available. Of these 63 biopsies, 32 (50.8%) were malignant tumors, including UC (n = 29) and adenocarcinoma (n = 3).
Clinical Characteristics of the Study Cohort
Data are presented as median (interquartile range) or n (%).
Clinical stage was based on CT/MRI before ureteroscopy.
cT stage = clinical tumor stage.
Primary endpoint
The sensitivity of PDD-URS was significantly higher than that of WL-URS (93.8% vs 62.5%, p = 0.0025) (Table 1).
Secondary endpoints
There was no significant difference between PDD-URS and WL-URS in terms of the specificity (77.4% vs 87.1%, p = 0.31) or PPV (81.1% vs 83.3%, p = 0.13). However, the NPV of PDD-URS was significantly higher than that of WL-URS (92.3% vs 69.2%, p = 0.027) (Table 2). The AUC-ROC of PDD-URS was significantly higher than that of WL-URS (0.86 vs 0.75, p = 0.0297) (Fig. 2).
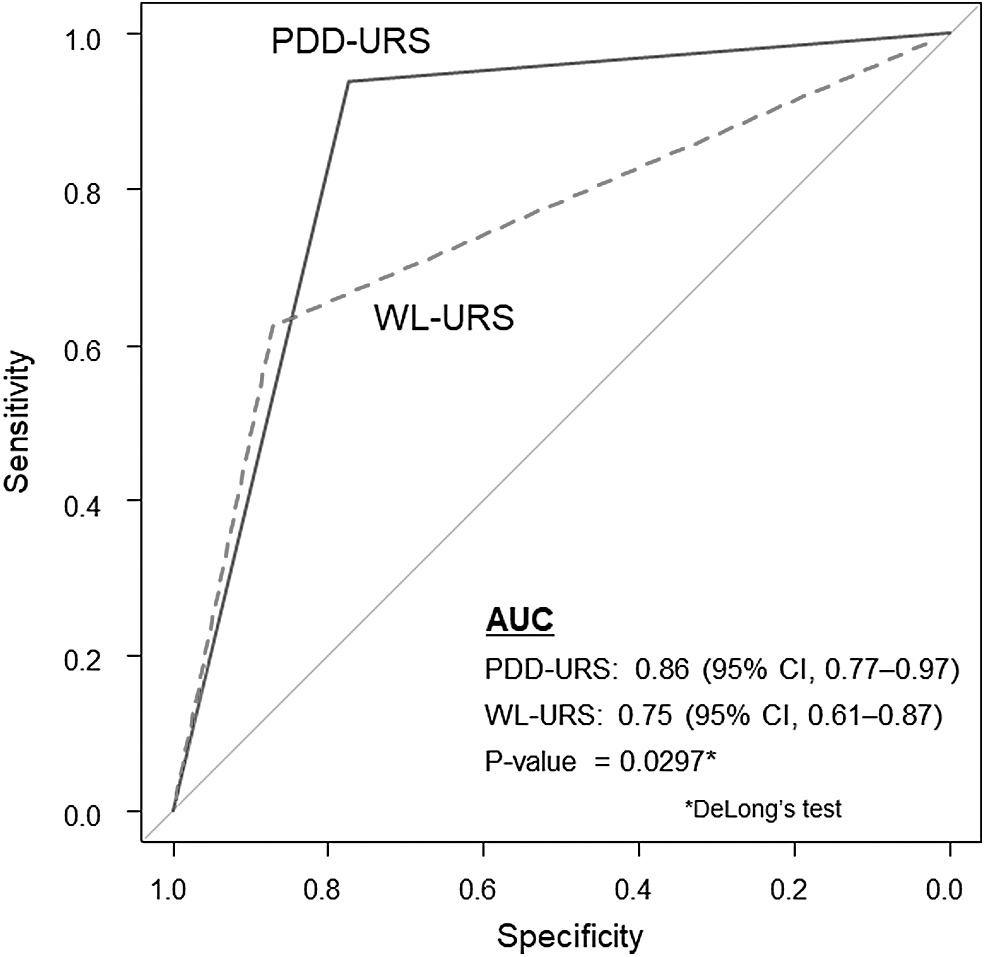
Comparison of diagnostic accuracy for upper urinary tract carcinoma between white light and blue light sources using receiver operating characteristic curve analysis. AUC = area under the curve; CI = confidence interval.
Comparison of Sensitivity, Specificity, Positive Predictive Value, and Negative Predictive Value for Upper Urinary Tract Carcinoma Between White Light and Photodynamic Diagnostic Ureteroscopy (n = 63 Biopsies from 20 Patients)
Data are presented as n (%) unless otherwise indicated.
McNemar's test, WL-URS vs PDD-URS.
Chi-square test, WL-URS vs PDD-URS.
CI = 95% confidence interval; PDD-URS = photodynamic diagnostic ureteroscopy; WL-URS = white light ureteroscopy.
Sensitivity and specificity analyses according to tumor appearance
In cases of no apparent tumors, the sensitivity of PDD-URS was significantly higher than that of WL-URS (83.3% vs 0.0%, p < 0.001), but there was no difference in specificity between the two techniques (88.9% vs 100.0%, p = 0.075) (Table 3). In cases of apparent tumors, both the sensitivity and specificity of PDD-URS were equal to those of WL-URS (each p > 0.05) (Table 3).
Comparison of Diagnostic Accuracy for Upper Urinary Tract Carcinoma Between White Light and Photodynamic Diagnostic Ureteroscopy According to Endoscopic Findings
Data are presented as n (%) unless otherwise indicated.
McNemar's test, WL-URS vs PDD-URS.
Lesions including normal mucosa or irregular flat lesions ± redness by WL-URS.
Lesions including papillary or sessile tumors by WL-URS.
Differential diagnostic ability of PDD-URS in abnormal pathologic findings
After excluding 11 normal tissue samples, the differential diagnostic ability of PDD-URS between benign lesions (inflammatory change/dysplasia) and malignant tumors was evaluated (n = 52) (Table 4). The sensitivity and specificity of PDD-URS were 93.8% and 75.0%, respectively, with a false-positive rate of 14.2% (5/35). In UCs (n = 32), the PDD-URS judgment was not influenced by the tumor grade (p = 1.0) (Table 4).
Differentiation Ability of Photodynamic Diagnostic Ureteroscopy in Abnormal Pathologic Findings
Data are presented as n (%).
Chi-square test.
Malignant tumors included urothelial carcinoma (n = 29) and adenocarcinoma (n = 3).
According to 2004 World Health Organization classification system of urothelial carcinoma.
Adverse events
Of all 20 patients, 8 (40.0%) developed AEs, but no patients died or discontinued the study because of AEs. Grade ≥3 AEs were not observed. One patient (5.0%) with a grade 2 increase in the alanine aminotransferase concentration recovered using Stronger Neo-Minophagen C (a glycyrrhizin-containing preparation). However, other patients with impaired liver function immediately recovered without any treatment. With respect to skin disorders, no patients developed photosensitivity reactions. Although urticaria occurred in one patient (5.0%), whether it was associated with oral 5-ALA could not be determined (Table 5).
Adverse Events Based on Common Terminology Criteria of Adverse Events v4.0 in 20 Patients
Data are presented as n (%).
ALP = alkaline phosphatase; ALT = alanine aminotransferase; AST = aspartate aminotransferase.
Discussion
Accurate localization of UTUC is a clinical difficulty for urologic oncologists. Since the recent development of ureteroscopes and imaging systems, diagnostic URS has become a more practical and useful tool for detection of UTUC. Based on the success of PDD cystoscopy for UC of the bladder, some investigators have tried to establish evidence of the utility of PDD-URS for UTUC. 12 –15 Kata et al. 15,21 published several articles regarding PDD-URS for UTUC with updates in their data. Their largest retrospective study involving assessment of 106 upper urinary tract units demonstrated that PDD-URS had a significantly higher sensitivity for detecting UTUC lesion than WL-URS (95.8% vs 53.3%, respectively), whereas the specificity of PDD-URS was equivalent to that of WL-URS (96.6% vs 95.6%, respectively). 13 Our results are consistent with theirs in that PDD-URS was significantly superior to WL-URS in sensitivity but not in specificity.
In general, obtaining adequate tissues that include the interstitial and muscle layers for accurate tumor staging and grading is difficult when using small URS biopsy forceps. 22,23 In addition, the protoporphyrin IX concentration in the muscular layer is minimal compared with that in the other layers. 24 Therefore, we might not have truly discriminated the degree of tumor invasiveness in this study because of the tiny samples taken by the Piranha®, even under PDD-URS. Despite these limitations, however, in addition to our detection of UTUC (low-grade tumor/CIS/high-grade invasive tumor) in irregular flat lesions, we could detect carcinomas in 21.8% (5/23) of normal-appearing lesions. Thus, PDD-URS is considered a powerful diagnostic and margin-assessment tool especially for UTUC in the category no apparent tumor, regardless of the tumor grade (Table 4).
The false-positive rate due to acute/chronic cystitis or previous intravesical instillation is a problem associated with PDD in the bladder and ranges from 38.2% to 58.0%. 24,25 For PDD in the upper urinary tract, our study showed a false-positive rate of 14.2% (5/35), which was associated with the presence of dysplasia or inflammatory change (Fig. 1B). Kata and coworkers 15 also demonstrated a low false-positive rate of 3.4% (2/58) when using PDD-URS. Accordingly, the false-positive rate of PDD for the upper urinary tract could be significantly lower than that of PDD for the bladder. One possible reason for this is that the upper urinary tract has a lower risk of urinary tract infection, which can cause inflammatory mucosa, than the bladder. 24,26 Therefore, PDD can be used with the advantage of low false-positive rates in the upper urinary tract.
Another common reason for false-positive PDD is tangential artifacts. 27 This effect can be minimized by using a closely directed f-URS and deepening the approaching angle to the pelvis or ureteral wall. 28 Therefore, observation with an f-URS, not only a semi-rigid URS, is required even in the ureter. Our URS procedure is similar to that reported by Kata et al. 21 However, we used a continuous irrigation system to maintain the irrigation flow and a clear view. This is because if the biopsy forceps is inserted into the URS working channel (3.6F), the amount of irrigation will be obviously decreased and lead to poor visibility due to hematuria from the biopsied lesions. Thus, we switched to the optimal irrigation pressure according to our experimental data 29 when using biopsy forceps, and this provided adequate flow and clear visibility for precise biopsy.
5-ALA is a well-known natural amino acid produced by mitochondria in animals and plants, and its toxicity is, therefore, very low. 17 Indeed, in this study, the AEs related to oral 5-ALA were grade <2; in particular, hepatobiliary disorder required no treatment in most patients. Unexpectedly, our patients' AE profile was quite different from that in a previously described European cohort. 16 Hypotension and facial rash, which are known as major complications of 5-ALA, were not observed in most of our patients. A multicenter phase III trial of oral 5-ALA for bladder cancer in a Japanese cohort similarly demonstrated that only 1.6% of patients developed such AEs. 30 Conversely, that study showed that patients tended to have gastrointestinal disorders, such as nausea or vomiting, corresponding to the findings of our study. Therefore, the AE profile related to oral 5-ALA may differ according to race or ethnicity.
This study has some limitations. First, it was a single-center case series with a small sample size. In addition, randomized clinical trials are needed to examine the difference in the prognosis of UTUC between the two types of diagnostic URS. Second, we did not assess the interobserver reliability between the two investigators, which may have resulted in observational bias. To minimize this, we used the panel of endoscopic appearances as described in Figure 1 and referred to it during the URS procedure. Despite these limitations, to the best of our knowledge, this is the first prospective clinical trial to use a strict protocol for establishing evidence of the utility of PDD-URS for detecting UTUC.
Conclusion
We found that PDD-URS with oral 5-ALA was superior to WL-URS in terms of sensitivity, NPV, and accuracy of diagnosis of UTUC, especially that within the category no apparent tumors. This technique is safe and can improve the quality of diagnostic URS for UTUC.
Footnotes
Acknowledgment
The authors express their heartfelt gratitude to SBI Pharmaceuticals Co., Ltd. for supplying the investigational drug for this study.
Author Disclosure Statement
Dr. Takashi Yoshida has a scientific contract with SBI Pharmaceuticals Co.,Ltd. The remaining authors have no competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.