
Abstract
Objective:
At present, prostate cancer radical surgery still lacks an objective standard for predicting the anatomic difficulty of surgery through preoperative examination. Due to the poor prognosis and surgical complications caused by “Narrow Pelvis,” a pelvic model for prediction is urgently needed. The purpose of this study is to present objective preoperative assessing indicators to predict the surgical difficulty caused by pelvic anatomic abnormalities during laparoscopic radical prostatectomy (LRP).
Methods:
Patients undergoing LRP were retrospectively analyzed and separated into “Common Pelvis” or “Difficult Pelvis” groups according to the preset criteria. The clinical data and pelvic imaging data of the two groups were compared to obtain statistically significant differences. The results were compared and validated in 500 ordinary males. Logistic regression analysis was performed to optimize these indicators into a scoring model, “Laparoscopic Radical Prostatectomy Narrow Pelvic Predictive Index (LRP-NPPI)” for predicting “Difficult Pelvis.”
Results:
Of the 145 patients undergoing LRP, 22 (15.2%) were included in the “Difficult Pelvis” group. Patients in the “Difficult Pelvis” group were more likely to have a narrower, shorter, deeper, more flattened pelvis, greater body mass index, more history of previous pelvic surgery, and greater prostate volume. Moreover, the larger amount of intraoperative blood loss and longer operation time were related. Compared with the “Common Pelvis” group, patients in the “Difficult Pelvis” have higher score of LRP-NPPI (p < 0.05).
Conclusion:
With the model we proposed, it is possible to predict patients with pelvic anatomical difficulties during LRP.
Introduction
Prostate cancer is the second most common cancer in men, with a global diagnosis of ∼1.1 million in 2012, accounting for 15% of all cancer diagnosis. 1 The frequency of autopsy prostate cancer is roughly the same worldwide. 2 According to autopsy reports, the incidence of prostate cancer patients over 79 years of age was 59% (48%–71%). 3 Radical prostatectomy has become the prior treatment for patients with clinically localized prostate cancer. 4 Other minimally invasive operations are also available, such as robot-assisted radical prostatectomy and laparoscopic radical prostatectomy (LRP). Due to the bony limitations, depth, angle, and visibility, pelvic surgery itself is more difficult than abdominal surgery. 5 Even minimally invasive surgery techniques have failed to demonstrate the advantages of open surgery in randomized clinical trials. 6,7
Laparoscopic surgery is a classic minimally invasive pelvic approach, which is suitable for operation in a relatively small pelvic space. However, it is difficult to predict whether the pelvis has anatomical difficulties by imaging data preoperatively. Studies have shown that in other low-level pelvic surgeries (such as rectal cancer surgery), gender, body mass index (BMI), pelvic diameter, and tumor size were identified as risk factors for increased postoperative complications. 8,9 Xu and colleagues' 10 study found that preoperative prostate-specific antigen (PSA), positive biopsy cores, BMI, Gleason score, tumor T stage under MRI, age, tumor volume, surgeon experience, and other indicators could manage to predict postoperative positive tumor margin, but the study lacked reports of pelvic stenosis on the operative difficulty.
In our clinical experience, it was found that factors such as pelvic diameter and angle have an impact on difficulty of radical prostatectomy, but there is currently no clear research and evidence. In the LRP patients in our medical center, about 10%–15% of patients have problems such as relatively small operating space, pubic occlusion vision, and difficulty in urethral anastomosis. Due to other factors such as prostate volume, tumor stage, and so forth, the judgment by surgeon of “Difficult Pelvis” is based on the relative operational space, therefore, a more objective “Difficult Pelvis” evaluation index is needed.
A similar “Difficult Pelvis” preoperative assessing model was proposed by Iqbal, 11 which showed that patients in the “Difficult Pelvis” group had higher intraoperative blood loss, longer operative time, longer hospital stay, higher hospitalization costs compared with “Routine Pelvis” group in rectal cancer surgery. The purpose of our study was to evaluate the commonality of patients with “Difficult Pelvis” in LRP through imaging examination, and to explore preoperative predictions (such as improving Trocar arrangement and changing operational strategies) to reduce the difficulty of surgery, the operative duration, and the occurrence of postoperative complications.
Materials and Methods
Selection and inclusion of general population
A total of 500 patients who underwent pelvic CT examination from September 2014 to September 2019 in the Zhongda Hospital affiliated to Southeast University were randomly selected for inclusion in our retrospective study. Inclusion criteria are as follows: (1) 18–89 years old, (2) gender male, (3) without pelvic trauma history, (4) without pelvic deformity, and (5) without pelvic therapeutic intervention. The study was approved by the Southeast University Review Board.
Selection and classification of patients who underwent operation
Patients diagnosed as prostate cancer and underwent LRP from September 2014 to September 2019 in the Zhongda Hospital affiliated to the University of Southeast University were included in this retrospective study. All included patients underwent the same operation with transperitoneal approach, managing dorsal venous complex with MONTSOURIS technique, and non-neurovascular bundle preservation. The dorsal venous complex is ligated with a 2-0 resorbable suture passed with a needle from one side of the complex to the other. Two continuous stitches were placed at surgeon discretion and tied. According to the preset criteria, the “Difficult Pelvis” group and the “Common Pelvis” group are: (1) all patients are stratified by tumor T stage, and the operation time is sorted in ascending order according to the interquartile range. One point is scored for every 25% (0–3), (2) one point is scored for unplanned reoperation due to postoperative pelvic complications, (3) prostate volume is graded from normal to IV°, and each degree is scored for one point, and (4) one point is scored if surgeon and first assistant confirm anatomical difficulty due to pelvic stenosis. The lowest total score is 0, and the highest score is nine points. Patients who scored more than five points are considered to be “Difficult Pelvis,” otherwise “Common Pelvis.”
Measurement of pelvic data
The pelvic CT scanning data of included patients were reconstructed in three dimensions, and the software was Neusoft PACS/RIS Version 5.5. The following data were measured: longitudinal pelvic inlet, longitudinal middle pelvic, longitudinal pelvic outlet, transverse pelvic inlet, transverse middle pelvic, transverse pelvic outlet, first sacrum/pelvic floor, first sacrum/coccyx, pubic inner side angle, pubic angle, umbilical tangential line, and posterior pubic angle (Fig. 1). All measurements were performed three times and averaged by the same measurer.
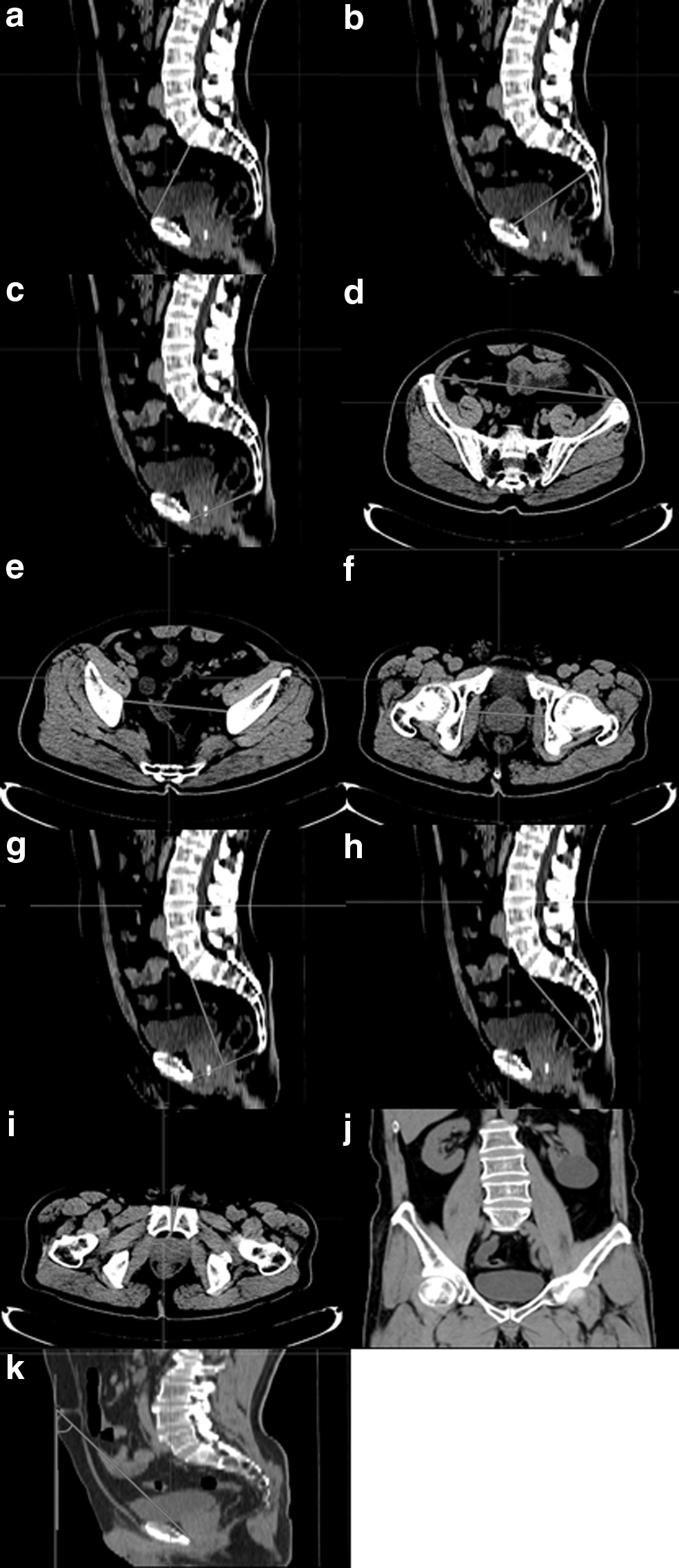
Pelvic diameters and angles measured with CT scanning (redline as measuring line, green line as adjuvant line).
Collection of clinical data, clinical outcomes, and postoperative complications of surgical patients
All included patients with prostate cancer were collected with clinical data (age, history of previous pelvic surgery, BMI, prostate volume, PSA, Gleason score, and tumor pathological T stage), postoperative complications (postoperative hemorrhage, postoperative infection, perioperative death, and unplanned reoperation) and clinical outcomes (surgical tumor margin, intraoperative blood loss, operative duration, transferring into open surgery, days of postoperative hospital stay). Patients with missing data were excluded.
Development of predictive model
By comparing the “Difficult Pelvis” group and the “Common Pelvis” group, some pelvic data with significant differences were selected and compared with the pelvic data of the general population. Multivariate logistic regression analysis was used to calculate the OR value of risk factors for each pelvis indicator. On this basis, the LRP narrow pelvic predictive index (NPPI) was proposed. Johnson's 12 study showed that relative weights should be considered when calculating the independent influence of variables in multivariate analysis. The relative weights of pelvic-related risk factors were calculated by Relative Weight Analyses (RWA) Web, a calculating system introduced by Tonidandel and colleagues. 13 The performance of the predictive model to distinguish “Difficult Pelvis” was evaluated by using the receiver operating characteristic (ROC) curve in 145 patients with prostate cancer in our study.
Statistics analyses
All statistical analyses were processed with SPSS 22.0. The statistical methods were Student's t-test, analysis of variance, and Logistic regression analysis, where appropriate.
Results
Clinical data, outcomes, and complications of patients who underwent operation
A total of 145 patients diagnosed with prostate cancer and underwent LRP were included. According to the previously mentioned preset criteria, 22 patients were classified as “Difficult Pelvis” group as observation group, and 22 patients were classified as “Common Pelvis” group as control (Table 1). Both groups of patients had the same tumor T stage distribution by screening. The “Difficult Pelvis” group had an average BMI of 25.43 kg/m2, and 10 (45.5%) patients had history of previous pelvic surgery. The median prostate volume was 53.45 cm3. Compared with the “Common Pelvis” group, the “Difficult Pelvis” group had larger BMI, more history of previous pelvic surgery, and greater prostate volume. Compared with the “Common Pelvis” group, the “Difficult Pelvis” group had more intraoperative blood loss and longer operation time. The median amount of intraoperative blood loss in the “Difficult Pelvis” group and the “Common Pelvis” group were 300 mL (50–2900 mL) and 125 mL (50–400 mL), respectively. The mean operation durations were 267.95 minutes (175–450 minutes) and 170.73 minutes, respectively (120–240 minutes). No significant difference was observed in preoperative PSA, Gleason score, and postoperative complications (postoperative hemorrhage, infection, death, unplanned reoperation, transferring into open surgery, and surgical tumor margin) between the two groups.
Clinical Data Outcomes and Complications of “Difficult Pelvis” Group and “Common Pelvis” Group
Bold values refer to p < 0.05.
BMI = body mass index; PSA = prostate-specific antigen; SD = standard deviation.
Pelvic data of patients underwent operation
All patients were scanned with pelvic CT in the perioperative period. After three-dimensional reconstruction of the imaging data, the previously mentioned pelvic diameters and angles were measured and the ratios between the diameters were calculated (Table 2). Our study found that patients in the “Difficult Pelvis” group had smaller longitudinal pelvic inlet, longitudinal middle pelvic, transverse middle pelvic, and first sacrum/coccyx in the pelvic diameter compared with the “Common Pelvis” group. In terms of pelvic angles, the “Difficult Pelvis” group had smaller pubic angle and larger umbilical tangential line and posterior pubic angle. In the pelvic diameter ratio, the “Difficult Pelvis” group had larger transverse pelvic inlet/longitudinal pelvic inlet.
Computed Tomography Imaging Pelvic Data of “Difficult Pelvis” Group and “Common Pelvis” Group
Bold values refer to p < 0.05.
Identification and validation of “Narrow Pelvis” in the general population
Currently, there is no pelvic anatomical definition of “Narrow Pelvis.” Based on the clinical experience of our medical center, we believe that 10%–15% of patients have pelvic stenosis during prostate cancer operation. Therefore, we ranked the pelvic data of general population in ascending order, and identified the data of <10% and >90% of the percentiles as extreme values, which were regarded as the pelvic anatomical risk factors of “Difficult Pelvis.” That is, “Anatomical Narrow Pelvis.” We selected clinically significant pelvic data with differences from the “Difficult Pelvis” group and the “Common Pelvis” group as research indicators. Among them, transverse middle pelvic and transverse pelvic inlet/longitudinal pelvic inlet were excluded due to the p value close to 0.05, and the pubic angle was excluded due to lack of clinical significance. The final selected pelvic data were: umbilical tangential line and posterior pubic angle, longitudinal middle pelvic, longitudinal pelvic inlet, and first sacrum/coccyx, studied for extreme values in the general population.
Development of “Difficult Pelvis” predictive model
The multivariate logistic regression analysis was used to calculate the OR values of each risk factor (Table 3). The pelvic-related risk factors were identified as umbilical tangential line and posterior pubic angle and longitudinal pelvic inlet. Logit (P) = −3.107 + 0.94 * umbilical tangential line and posterior pubic angle (°)−0.234 * longitudinal pelvic inlet (mm).
Logistic Regression Analysis of Pelvic Data in “Difficult Pelvis”
Bold values refer to p < 0.05.
CI = confidence interval.
By calculating the relative weights, we obtained the independent influence degree of the risk factors. The standardized relative weights of umbilical tangential line and posterior pubic angle (°) and the longitudinal pelvic inlet (mm) were 0.8 and 0.2, respectively.
Based on the results, we developed LRP-NPPI. We equally divided the two pelvic indicators into four portions among the general population as quartiles, and the intervals were scored as 0–3 (Table 4), respectively. The greater extent of pelvic stenosis came with a higher score. The final score calculation formula is: LRP-NPPI = umbilical tangential line and posterior pubic angle score * 0.8 + longitudinal pelvic inlet score * 0.2.
Laparoscopic Radical Prostatectomy Narrow Pelvic Predictive Index
Validation of LRP-NPPI in surgical patients
In the mentioned 145 patients who underwent LRP, we applied the predictive model and observed the scores of the “Difficult Pelvis” group and the “Common Pelvis” group. Our results showed that patients in the “Difficult Pelvis” group had higher score of LRP-NPPI (2.80, 0.40) compared with the “Common Pelvis” group (2.20, 1.40), and the difference was statistically significant (p < 0.001). Finally, we used the ROC curve to evaluate the performance of this predictive model for the “Difficult Pelvis” with an area-under-curve (AUC) of 0.780 (95% confidence interval: 0.698–0.862) (Fig. 2). Comparing to well-known variables, BMI, and prostate volume, the AUC value of LRP-NPPI was significantly higher (BMI: p = 0.064, prostate volume: p < 0.001).
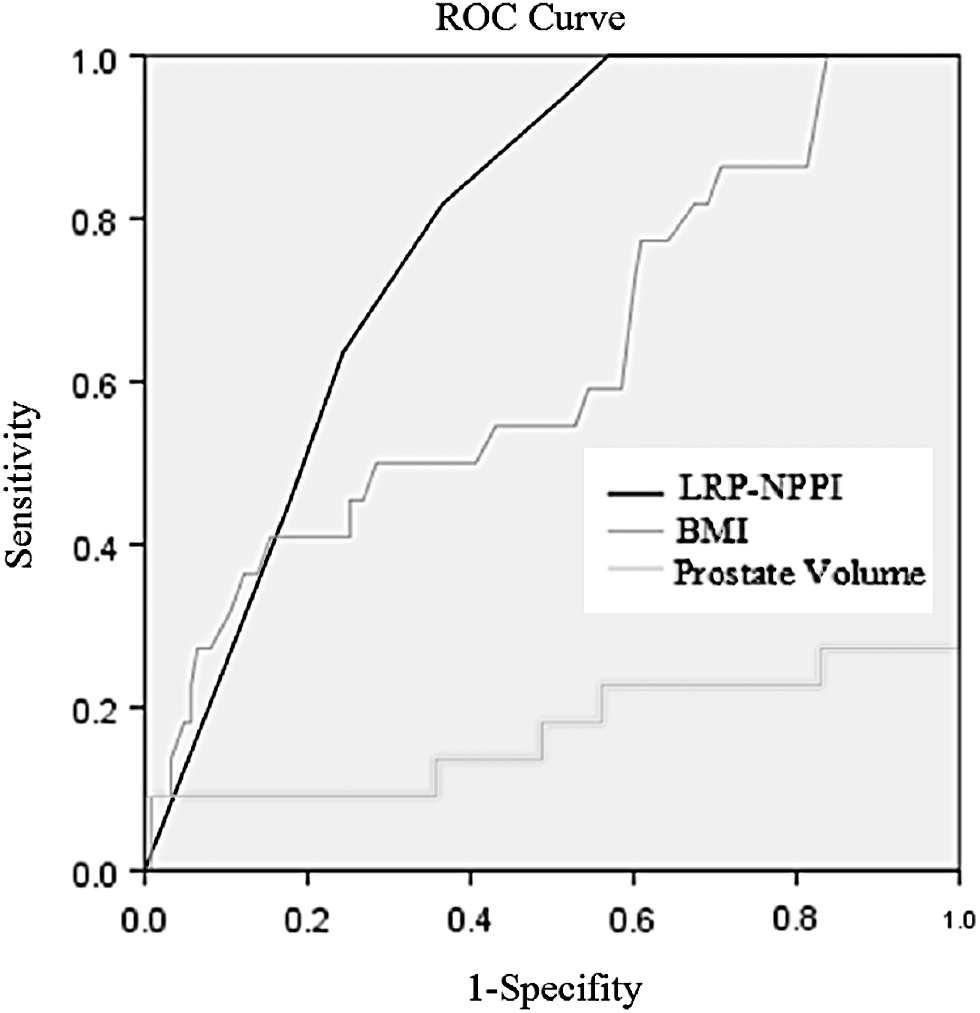
ROC curve of prediction of “Difficult Pelvis” using LRP-NPPI. LRP-NPPI = laparoscopic radical prostatectomy narrow pelvic predictive index; ROC = receiver operating characteristic.
Discussion
At present, other urological tumor surgery has a preoperative predictive scoring model to assess the extent of surgical difficulty, such as the R.E.N.A.L score of renal cell carcinoma surgery, 14 but there is no corresponding predictive model for prostate cancer radical surgery. In previous studies, there were evidences that the risk factors associated with the difficulty of radical prostatectomy included tumor stage, prostate volume, BMI, and previous history of prostate surgery. 15 –19 Studies have also shown that obesity and BMI have no significant correlation with positive surgical tumor margin after prostate cancer surgery. 20 The history of pelvic surgery has no significant effect on the degree of prostate cancer surgery. 15 In this study, we proposed a set of preset criteria, including subjective factors and objective factors. By developing scoring system, our aim was to reduce the bias due to subjective judgment of the surgeon. Furthermore, 5 clinical data, 9 clinical outcomes, and 20 pelvic data were researched. Compared with the “Common Pelvis” group, “difficult pelvis” group has higher average BMI value (25.43 kg/m2), more history of previous pelvic surgery (45.5%), and larger prostate volume (53.45 cm3). This result is consistent with Montorsi and colleagues. 21 For patients with prostate cancer who have obesity, previous history of abdominal surgery, large prostate volume, and previous history of pelvic radiotherapy, the radical surgery is difficult and should be completed by experienced surgeons. In terms of clinical outcomes, more intraoperative blood loss and longer operative duration are bad clinical outcomes caused by “Difficult Pelvis.” However, there were no significant differences in surgical tumor margin between the two groups. Yuksel and colleagues 22 indicated that the surgical tumor margin of prostate cancer surgery is more related to the disease progression, such as the number of positive biopsy cores, Gleason score, risk grading, seminal vesicle invasion, and extracapsular invasion of the prostate. In addition, among the 20 imaging pelvic data, we found that 7 of them were different between the two groups. Through the analysis of the diameter, angle, and ratio, patients in the “Difficult Pelvis” group are more likely to have pelvis that is narrower, shorter, deeper, and more flattened.
However, there is no clear evidence of “Anatomical Narrow Pelvis” causing “narrow pelvis laparoscopic radical prostatectomy,” thereby reducing the operating space and surgical field. To further validate this hypothesis, we collected pelvic data of 500 male patients in the general population. We applied the pelvic cavity of 10% of the clinical experience as “Narrow Pelvis” in the general population, and identified this part of the population as “Anatomical Narrow Pelvis.” We hoped that through the preset criteria classification of “Difficult Pelvis,” it would be possible to distinguish patients with “Narrow Pelvis.” In this study, we used Logistic regression analysis to finally include the umbilical tangential line and posterior pubic angle and the longitudinal pelvic inlet as the pelvic risk factors for “Laparoscopic Radical Prostatectomy Narrow Pelvis.”
We developed these two selected pelvic indicators into “Laparoscopic Radical Prostatectomy Narrow Pelvic Predictive Index (LRP-NPPI).” It is widely recognized 23 that multicollinearity makes the partitioning of variance among multiple correlated predictors difficult. To eliminate this error and clarify the coefficients of various indicators in the predictive model, we adopted the concept of “relative weights” proposed by Johnson 24 in his research. Relative weight refers to the proportion of each predictor's contribution to the standard deviation of the total forecast, considering the contribution of the variable itself and its combination with other predictors. Through RWA Web, 13 we calculated the relative weights of the umbilical tangential line and posterior pubic angle and the longitudinal pelvic inlet in the predictive model, and finally determined their influence coefficients as 0.8 and 0.2. The results indicated that patients in the “Difficult Pelvis” group had higher LRP-NPPI score, and the predictive model has a good predicting performance for evaluating “Difficult Pelvis.”
Conclusions
In our study, the risk factors for difficult pelvis were identified as: BMI, previous pelvic surgery history, prostate volume, the umbilical tangential line and posterior pubic angle, and the longitudinal pelvic inlet. The predictive modeling formula is: LRP-NPPI = umbilical tangential line and posterior pubic angle score * 0.8 + longitudinal pelvic inlet score * 0.2. The model currently still needs further large-scale prospective studies for deeper verification.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was approved by the Institutional Review Board of Southeast University. This study was funded by Jiangsu Provincial Medical Youth Talent (QNRC2016821). The sponsors contributed to the writing of the report and submission of the article for publication.