
Abstract
Introduction:
The Levita™ Magnetic Surgical System (LMSS) is a new device that can provide retraction using magnets and can reduce the number of ports used during laparoscopic and robotic procedure. It is U.S. Food and Drug Administration (FDA) approved for laparoscopic cholecystectomy, bariatric operation, and robotic radical prostatectomy. Our objective was to evaluate the safety and feasibility of the magnetic surgical system during renal procedure.
Methods:
We performed a prospective, single-center, single-arm, open-label study to assess the safety and performance of the LMSS. The system includes a deployable, single-use magnetic grasper and a reusable external magnet. Selected patients undergoing either laparoscopic or robotic renal procedure from April 2019 to August 2019 were included. Robotic procedures were performed with the da Vinci Xi or single-port (SP) surgical platforms. Preoperative demographic, intraoperative data, and postoperative data were collected and analyzed.
Results:
Ten procedures were performed using the LMSS. Cases included Xi robotic partial nephrectomy (n = 3), Xi robotic radical nephrectomy (n = 2), SP robotic partial nephrectomy (n = 2), SP robotic pyeloplasty (n = 1), laparoscopic donor nephrectomy (n = 1), and laparoscopic radical nephrectomy (n = 1). No cases required conversion to an open procedure. Issues included one small liver capsular tear from the device jaws necessitating fulguration and occasional robotic “recoverable fault” errors when the external magnet was placed too close to the robotic arms.
All patients were discharged home on postoperative day 1 or 2, and there were no readmissions within 30 days.
Conclusions:
This is the first report on the use of the LMSS for renal procedure. Its use for laparoscopic and robotic renal procedure appears safe and feasible. The grasper is especially useful for exposing the renal hilum during dissection and the ureteropelvic junction during SP robotic procedures, mimicking multiport techniques. Further study is required to optimize use of the LMSS and evaluate its cost effectiveness.
Introduction
Major technological innovations over the past 40 years are responsible for the transition from traditional open procedure to minimally invasive procedure. In the 1980s and 1990s, laparoscopy revolutionized operation by enabling major operations to be performed through small incisions. In the early 2000s, the robotic procedure platform improved laparoscopy by allowing surgeons to have greater dexterity, visualization, and mobility. Minimally invasive procedure has been shown to improve patient outcomes and decrease overall health care costs, and recent efforts to further reduce surgical morbidity have focused on reducing the size and number of surgical ports. However, reduced-port approaches can be limited by incomplete triangulation of instruments, instrument collisions, and poor visualization.
The Levita™ Magnetic Surgical System (LMSS) is a new retraction instrument that may mitigate some of the issues of reduced-port laparoscopic and robotic procedure. 1 The system works by introducing a spring-loaded grasper with a small magnetic end into the surgical space, attaching it to the desired tissue and then manipulating the grasper using a second stronger external magnet. The retractor and tissue can be pulled in any direction. This technique can avoid an extra incision and port that would otherwise be used for retraction. The system received U.S. Food and Drug Administration (FDA) clearance for use in cholecystectomy in June 2016, 2 bariatric operation in September 2018, 3 and prostatectomy in April 2019. It has been described for gallbladder retraction during laparoscopic and robotic cholecystectomy, liver retraction during laparoscopic bariatric procedure, and retraction of the colon, peritoneum, seminal vesicles, prostatic capsule, and bladder during reduced-port prostatectomy. 4,5
Our objective was to evaluate the safety and efficacy of the magnetic retractor for laparoscopic and robotic renal surgeries. In this case series, we are the first to report the use of magnetic retraction during minimally invasive renal procedure.
Methods
Study
This was a prospective, single-center, single-arm, open-label study to assess the safety and performance of the LMSS (Levita Magnetics, San Mateo, CA). Patients undergoing either laparoscopic or robotic procedure using the LMSS from April 2019 to August 2019 were included. All the cases were completed by a single experienced robotic surgeon (M.P.). This study was approved by the Institutional Review Board at the Mount Sinai Health System.
Patient selection
The study population consisted of selected nonrandomized adult patients who were scheduled for either laparoscopic or robotic renal procedure. We sought to enroll a variety of patients that reflect our typical surgical caseload including laparoscopic and robotic (Xi and single-port [SP]) radical nephrectomy, partial nephrectomy, and pyeloplasty. Patients were excluded if they reported having metallic implants (pacemakers or prostheses). Preoperative demographic data (gender, age, body mass index, and significant comorbidities), intraoperative data (operative time, estimated blood loss, number of trocars, and robotic arms used), and postoperative data (length of hospitalization, Clavien–Dindo complications, and final pathology report in the case of malignant tumors) were collected.
Magnetic surgical system
The LMSS includes a single-use deployable magnetic tissue grasper, a single-use laparoscopic deployment handle, and a reusable external magnet that is held in position by a locking arm (Figs. 1 and 2). The magnetic tissue grasper is placed into the surgical space and is opened and closed onto the desired tissue by spreading or squeezing the deployment handle. Once the tissue is firmly grasped, the deployment handle is squeezed further to release the tissue grasper from the handle. The external magnet is positioned over the patient using a bedrail-mounted locking arm. A bedside assistant can manipulate the external magnet over the patient's body to couple the magnets and retract the tissue effectively.

Levita™ Magnetic Surgical System:

Operative technique
All patients were positioned in the right or left lateral decubitus position, depending on the operative site. They were then secured to the operating room table using a bean bag immobilizer and cloth tape across the shoulders and hip area. The magnetic arm was attached to the surgical bed on the side of the assistant and was draped using a sterile C-arm fluoroscopy drape. The LMSS requires at least a 10 mm port for insertion. For laparoscopic cases, we routinely use three trocars—5, 11, and 12 mm. Robotic cases were performed using the Intuitive Surgical da Vinci Robotic Assisted Surgical Systems (Intuitive, Sunnyvale, CA), Xi and SP models. For Xi cases, we used 8 mm robotic trocars and a 12 mm assistant port, and for SP cases, we used a standard 25 mm robotic trocar and a 12 mm assistant port. If necessary, for right-sided cases, an additional 5 mm port was used for placement of a liver retractor. During operation, the LMSS was used to retract Gerota's Fascia during colon mobilization, retract the kidney laterally during hilar dissection, retract tumors during excision, and retract the ureteropelvic junction during pyeloplasty.
Results
Ten patients underwent operation using the LMSS. Table 1 provides the patient's baseline characteristics, operative indications, and procedures performed. The average patient age was 65.9 ± 6.4 years. Operation was performed for eight renal tumors with an average size of 5.2 ± 2.3 cm, one ureteropelvic junction obstruction, and one kidney donor. Cases included Xi robotic partial nephrectomy (n = 3), Xi robotic radical nephrectomy (n = 2), SP robotic partial nephrectomy (n = 2), SP robotic pyeloplasty (n = 1), laparoscopic donor nephrectomy (n = 1), and laparoscopic radical nephrectomy (n = 1).
Baseline Characteristics
LND = lymph node dissection; SP = single port; UPJ = ureteropelvic junction.
Surgical outcomes are given in Table 2. Laparoscopic cases required three ports, Xi robotic cases required five or six ports, and SP robotic cases required two ports. The average warm ischemia time for the five partial nephrectomies was 25 ± 14 minutes. The average estimated blood loss was 95 ± 120 mL and operating room time was 170 ± 35 minutes. No cases required conversion to an open procedure or experienced complications. All patients were discharged home on postoperative day 1 or 2, and there were no readmissions within 30 days. Final pathology analysis of the seven kidney tumor operations included renal cell carcinoma pT1a (n = 2), renal cell carcinoma pT1b (n = 4), mucinous tubular and spindle cell carcinoma (n = 1), and angiomyolipoma (n = 1). All margins were negative.
Intraoperative and Postoperative Patient Outcomes
AML = angiomyolipoma; RCC = renal cell carcinoma.
The LMSS grasper was especially useful for retracting Gerota's Fascia during colon mobilization, retracting the kidney laterally during hilar dissection, to retract tumors during excision, and to retract the ureteropelvic junction during pyeloplasty. It was particularly helpful during robotic SP cases (Fig. 3) No renal tissue damage or tearing was observed while using the magnetic retractor. When used to retract the liver, we observed a small capsular tear from the device jaws, which was easily fulgurated.
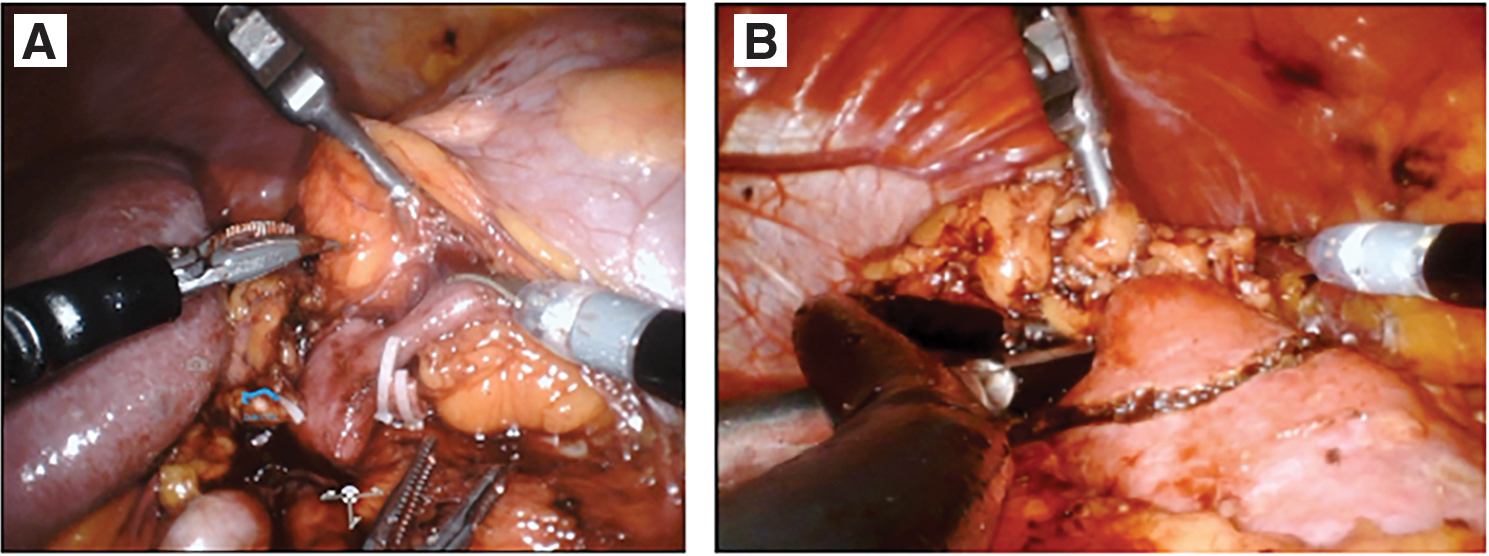
Intraoperative images of the magnetic retractor:
We encountered two primary intraoperative issues related to the LMSS. First, if the external magnet was placed too close to any of the robotic arms, it could trigger a “recoverable fault” error necessitating reconnection of the arm to the trocar. Second, inside the body, instrument tips and needles tended to become magnetized. Although this could be a nuisance, we did not experience any detrimental surgical consequences from the magnetized needles.
Discussion
This study is the first reported use of the LSMM for renal procedure. Our experience shows that magnetic retraction is safe and feasible during a variety of laparoscopic and robotic renal operations. The goal of minimally invasive procedure is to perform safe operations, abide by established surgical principles, and reduce surgical morbidity by reducing incision size. The primary disadvantages of minimally invasive surgical approaches compared with open techniques have been reduced visibility and limited instrument mobility. Since the advent of laparoscopy, many instruments have been developed to maintain and enhance exposure during operation. The LMSS is an innovative device designed to aid tissue retraction during laparoscopic procedure. The magnet overcomes the limitations of earlier instruments as it can be repositioned as needed and the vector of retraction can be easily adjusted without the need for new port placement.
Although this particular device is novel, there is a long history of use of magnets in opeation. In fact, the first use of magnets in operation dates back to the mid-1880s, when several British case reports described use of electromagnets for successful removal of foreign metal objects from the eye. 6 In 1953, an otolaryngologist in Philadelphia published the use of a sterile magnet as an instrument holder during rhinoplasty. 7 During the modern push for minimally invasive procedure, a renewed interest developed in using magnets during operations. 8 Magnets have since been used in operation in a variety of ways including esophageal sphincter augmentation, compressive bowel anastomosis, and retrieval of lost intra-abdominal surgical needles. 9 Finally, a similar device to the Levita was described in Korea in 2016 that used a 0.69 g internal magnet that was sutured to tissue and paired with a 1543 g external magnet. The device was successfully tested to retract the kidney in a pig model during 10 laparoendoscopic single site simple nephrectomies. 10
The Levita device was developed by a Chilean surgeon in the late 2000s and filed for U.S. patent in 2013. The first reported human use of the LMSS was in a case series of 10 patients who underwent laparoscopic cholecystectomy. 2 The authors reported no perioperative complications, and concluded that routine use of the magnetic system may reduce the total number of laparoscopic trocars used, leading to less tissue trauma and improved cosmesis. Soon after, a larger 50-patient magnetic-assisted laparoscopic cholecystectomy cohort was published. 11 In these cases, cholecystectomy was performed using three ports instead of the conventional four-port technique. No device-related serious adverse events were reported. The device has seen its most robust adoption in the field of bariatric operation, where it is being used as a liver retractor to reduce the number of laparoscopic surgical incisions. 1
In urology, the LMSS was first used successfully during a case series of three da Vinci Xi robotic radical prostatectomies performed at UT Southwestern. 5 The magnet enabled the surgical team to perform the cases using a reduced three robotic arms technique. The same group next published on the use of the LMSS during da Vinci SP robotic radical prostatectomy. 12 In 15 patients, a standard SP 25 mm robotic cannula and an additional 12 mm assistant port were used in combination with the magnetic retractor to facilitate tissue exposure and improve procedure ergonomics, mimicking the conventional multiport technique. No cases required conversion to multiport or open procedure, and no intraoperative or postoperative complications were reported.
In this series, we identified the versatility of the LMSS in different surgical scenarios. First, the magnet was useful during live left donor nephrectomy. The tissue grasper can safely retract the perirenal tissue during dissection of the ureter and vascular structures, aiding removal of the kidney while also maintaining its integrity. We did not change our technique or the number of trocars we usually insert; however, the device improved visualization of the organ. The LSMM could play an important role during right nephrectomy because the magnetic grasper can retract the liver, avoiding an extra trocar for a liver retractor tool.
Second, the LSMM was also useful during robotic partial nephrectomy. In all cases, the magnetic grasper was introduced through the 12 mm assistant port. During da Vinci Xi cases, the magnetic retractor could eliminate the need of a fourth robotic arm, thereby conferring cost savings of ∼$280 per case associated with use of an extra robotic instrument and trocar. 13 The LSMM device itself costs ∼$300, making the total expenditure equivocal. Furthermore, using fewer incisions and trocars may lead to quicker postoperative recovery, decreased analgesic requirements, improved cosmetic outcome, and decreased risk of wound infection.
Finally, we found the greatest utility of the LMSS during da Vinci SP robotic cases because the LMSS can help mimic the mechanics of a conventional multiport technique. The elbowed instruments of the da Vinci SP platform change the motion dynamics, and triangulation of the instruments into a surgical field can be challenging. Some of this effect is mitigated by the new camera control options that allow shifting of the surgical workspace; however, retraction can still be challenging. The LMSS can retract along vectors that would be impossible or awkward for the SP arms and would require placement of an additional trocar. Although the SP technology is still evolving, the LMSS may be a useful tool toward true SP procedure.
We found that there is a short learning curve for using the magnetic device. After initial placement and draping of the articulating arm and external magnet, the deployable magnetic tissue grasper can be placed with the hand piece. The precise force generated between two magnets was determined through the strength and orientation of both magnets as well as the magnetic moment and magnetic field of each. Through some trial and error, a surgeon can quickly get a feel for the magnetic retractor and its retraction force. Care must be taken when positioning the external magnet intraoperatively and after operation. Intraoperatively, it cannot be placed too close to the robotic arms as the magnet can trigger a recoverable fault in the connection between the arm and the robotic trocar. It should also be placed away from any loose instruments that can theoretically be drawn to the magnet and move in unexpected ways. After operation, the magnet should be properly stored in its carrying case, away from electronics that can become magnetized and loose instruments.
In the future, the LMSS may become a useful tool in the armamentarium of robotic kidney procedure. As increased emphasis builds toward reduced port and SP minimally invasive procedures, the LMSS may become critical for proper retraction. Modifications that would improve the technology include a more precise hand piece to ease deployment of the tissue grasper and a more powerful external magnet to generate more force. Perhaps an electromagnet would make the external magnet less bulky and generate a more precise and powerful magnetic field. Further innovations in the space of magnetic-assisted operation will continue to drive instruments like this into the future.
Conclusion
In our series, the use of the LMSS during minimally invasive renal procedure proved to be safe and feasible. The grasper is especially useful for exposing the renal hilum during dissection and the ureteropelvic junction during SP robotic pyeloplasty, mimicking multiport techniques. It is important that the bedside assistant feels comfortable and confident both with the use of the clamp and with the manipulation of the external magnet. Future studies should focus on optimizing use of the magnetic retractor during renal procedure and evaluate its cost-effectiveness.
Footnotes
Acknowledgments
This study was performed in its entirety at the Icahn School of Medicine at Mount Sinai with no outside support. Levita Magnetics provided the devices for use in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.