
Abstract
Purpose:
Malignant extrinsic ureteral obstruction (MEUO) is a challenging clinical problem. Many factors weigh into the decision to proceed with retrograde ureteral stent (RUS), nephrostomy tube (NT), or observation; however, there is no consensus for the optimal approach. The objective of this study was twofold. First, to determine practice patterns by correlating patient, hospital, and disease characteristics to manage MEUO; second, to describe treatment trends of MEUO over time.
Materials and Methods:
Using the National Inpatient Sample 2010–2015, we abstracted all adults with diagnoses of hydronephrosis and concurrent metastasis or lymphoma, excluding any record with a diagnosis of urinary tract stone. Multinomial regression assessed predictors of undergoing no decompression, stenting, or nephrostomy. Quarterly trends and annual percentage change of MEUO prevalence and percentage decompressed with stent vs nephrostomy were calculated.
Results:
There were an estimated 238,500 cases of MEUO from 2010 to 2015, of which 18.0% underwent decompression with RUS and 11.4% NT. On multinomial regression, prostate (odds ratio [OR] 1.5), bladder (1.6), cervical (1.6) cancer, academic hospitals (1.4), and acute kidney injury were among factors that most significantly increased odds of undergoing NT. Factors that significantly increased odds of undergoing RUS included colon (OR 1.4), rectal/anal (1.3), ovarian (1.2) cancer, Midwest (vs northeast) hospitals (1.4), and female gender (1.4), whereas decreased odds of RUS were associated with bladder cancer (0.7), nonwhite race (0.8), and weekend admission (0.8). While MEUO prevalence has been increasing on an average of 2.9%/year, decompression rates have been decreasing, driven solely by a decrease in RUS of 3.8%/year on average.
Conclusions:
There is substantial variation in approach for MEUO among patient, hospital, and disease types, with an overall decline in stenting compared with steady nephrostomy use. Further investigation into best approaches for certain patient characteristics and disease types is needed to standardize care and reduce disparities.
Introduction
Malignant extrinsic ureteral obstruction (MEUO) carries a markedly poor prognosis with studies reporting median survival times ranging from 3 to 7 months. 1 –6 The urologist is typically the primary consultant for decisions regarding observation or decompression with retrograde ureteral stenting (RUS) or nephrostomy tube (NT) placement. Management decision may be influenced by presenting illness, malignancy type with anatomic considerations, patient prognosis, as well as patient and surgeon preference. Surveys have shown lack of consensus for preferred management among urologists with RUS vs NT 7 and among management preferences between urologists and oncologists. 8
Previous studies of practice patterns and outcomes of MEUO have been limited to single-institutional, retrospective reviews with the largest series in Brazil comprising 208 patients. 4 The most common malignancies found to cause MEUO in this series were bladder (23%), colorectal (22%), and cervical cancers (21%). In contrast, Brigham and Women's series of 157 MEUO patients found ovarian cancer (17%) the most common cause of MEUO followed by lymphoma (11%) and cervical cancer (10%). 9 Based on the available literature, it is difficult to determine the relative incidence of cancer type causing MEUO as well as the initial rates of decompression with either RUS or NT as the majority of studies contain patients who were either entirely decompressed with NT 5,10 or all had an initial attempt with RUS with conversion to NT if RUS failed. 4,9 Studies comparing both modalities have shown relatively equal usage of RUS and NT, 11 and favoring NT 75% of the time, 12 but there are no clear indicators as to why one modality was chosen over the other.
In the present study, we utilize the largest database of inpatients in the United States to characterize disparities of decompression with RUS or NT among patients with MEUO of varying malignancies with regard to patient, hospital, and disease characteristics. The primary objective was to reveal national practice patterns that influence the decision to manage these patients with observation, RUS, or NT. Secondarily, we sought to characterize national trends regarding prevalence of MEUO and treatment with RUS vs NT.
Materials and Methods
Data source
This study used the National Inpatient Sample (NIS), the largest all-payer inpatient care database in the United States, representing more than 97% of the population. The NIS is sponsored by the Agency for Healthcare Research and Quality and developed for the Healthcare Cost and Utilization Project (HCUP), and is designed to sample 20% of all discharges from U.S. community hospitals. Each weighted discharge record contains up to 30 International Classification of Diseases (ICD)-9 diagnosis codes and 15 ICD-9 procedure codes with numerous patients, hospital, socioeconomic, demographic, and outcomes of mortality rate, length of stay, and cost specified. Utilizing the provided code from the HCUP website, 13 Elixhauser comorbidity mortality rate scores were generated from diagnosis-related group and ICD-9 diagnosis codes.
Population
To identify the study population, all patients age 18 and older from 2010 to 2015, with diagnoses of hydronephrosis and concurrent metastasis or lymphoma, were identified using ICD-9 codes specified within the Elixhauser score for metastasis or lymphoma. Using the provided clinical classification software (CCS) codes on the HCUP website, 14 we excluded all patients with any diagnosis of kidney stone (CCS 160) and also classified patients by cancer type (genitourinary [GU], gastrointestinal [GI], gynecologic [GYN], lymphoma, and other/not defined). ICD-9 procedure codes were then used to identify whether hospitalized patients underwent RUS (59.8), retrograde pyelogram (RPG: 87.74), and/or NT placement (55.02 or 55.03). Next, disease characteristics such as acute kidney injury (AKI), urinary tract infection (UTI), and sepsis were generated from their respective ICD-9 codes (Table 1). To reduce the likelihood of internal malignant obstruction as a cause for hydronephrosis, we excluded all patients with procedure codes that indicated biopsy or resection of obstruction (Table 1).
International Classification of Diseases-9 Code Descriptors for Inclusion/Exclusion Criteria
AKI = acute kidney injury; ICD = International Classification of Diseases; UTI = urinary tract infection.
In patients who underwent both RUS and NT at some point during hospitalization, by comparing both procedures' days of procedure variable (PRDAYx), we were able to elucidate the first procedure type for analytic categorization (RUS and NT groups were mutually exclusive). On the rare occurrence when RUS and NT occurred on the same day, RUS was assumed to have occurred first as the more likely first choice followed by NT for RUS failure. Patients who had an RPG followed by a NT on the same or subsequent hospital day were analyzed within the RUS group.
Statistical analysis
All analyses accounted for NIS sampling weights with hospital strata and clustering design in accordance with published best practices. 15 For the purposes of descriptive analysis, cancer type (GU, GI, GYN, lymphoma, not specified/other) was used for stratification. Weighted frequencies were created for categorical variables and weighted means generated from continuous variables. Formal statistical comparison between each variable within the five groups is not presented as there was no preconceived hypothesis regarding differences; furthermore, preliminary testing using the Kruskal/Wallis test for nonparametric continuous variables and the chi-square test for proportions showed nearly all p < 0.001 as would be expected with such a large data set with different group populations.
Weighted multinomial logistic regression assessed predictors of undergoing no decompression, RUS, or NT. Covariates included patient demographics (age, sex, white/nonwhite race, weekend admission, insurance payer comorbidities of chronic kidney disease (CKD), congestive heart failure, coagulopathy, obesity, and weight loss), hospital characteristics (academic/nonacademic, rural/urban, hospital size, and hospital region), cancer type, and acute illness characteristics (AKI, UTI/pyelonephritis, sepsis). As decision for decompression in an acute hospital setting likely varies based on the interactions of the clinical parameters of AKI, UTI, and sepsis (i.e., all three present together would synergistically increase odds of decompression greater than their individual additive effects in isolation), interaction variables between these three parameters were generated for inclusion in the model. All variables included in the multivariable model were checked for multicollinearity using variance inflation factors (VIF). The VIF of all variables included in the model were below 2, with an average VIF of 1.2, indicating extremely low collinearity in the model. SPSS version 25 was used for all analyses.
Results
There were an estimated 238,500 cases of MEUO from 2010 to 2015. The proportion of cases within each cancer category is detailed in Figure 1 with GU malignancy having the highest frequency (29.7%), followed by GI (24.3%) and GYN (20.8%). Further breakdown of these categories is detailed in Figure 1, which shows the leading cancer type among all subtypes as prostate cancer (17.6%), followed by colon cancer (11.4%), lymphoma (10.3%), and bladder cancer (9.8%). Among all cases, there was no decompression, RUS placement, and NT placement in 70.6%, 18.0%, and 11.4%, respectively.
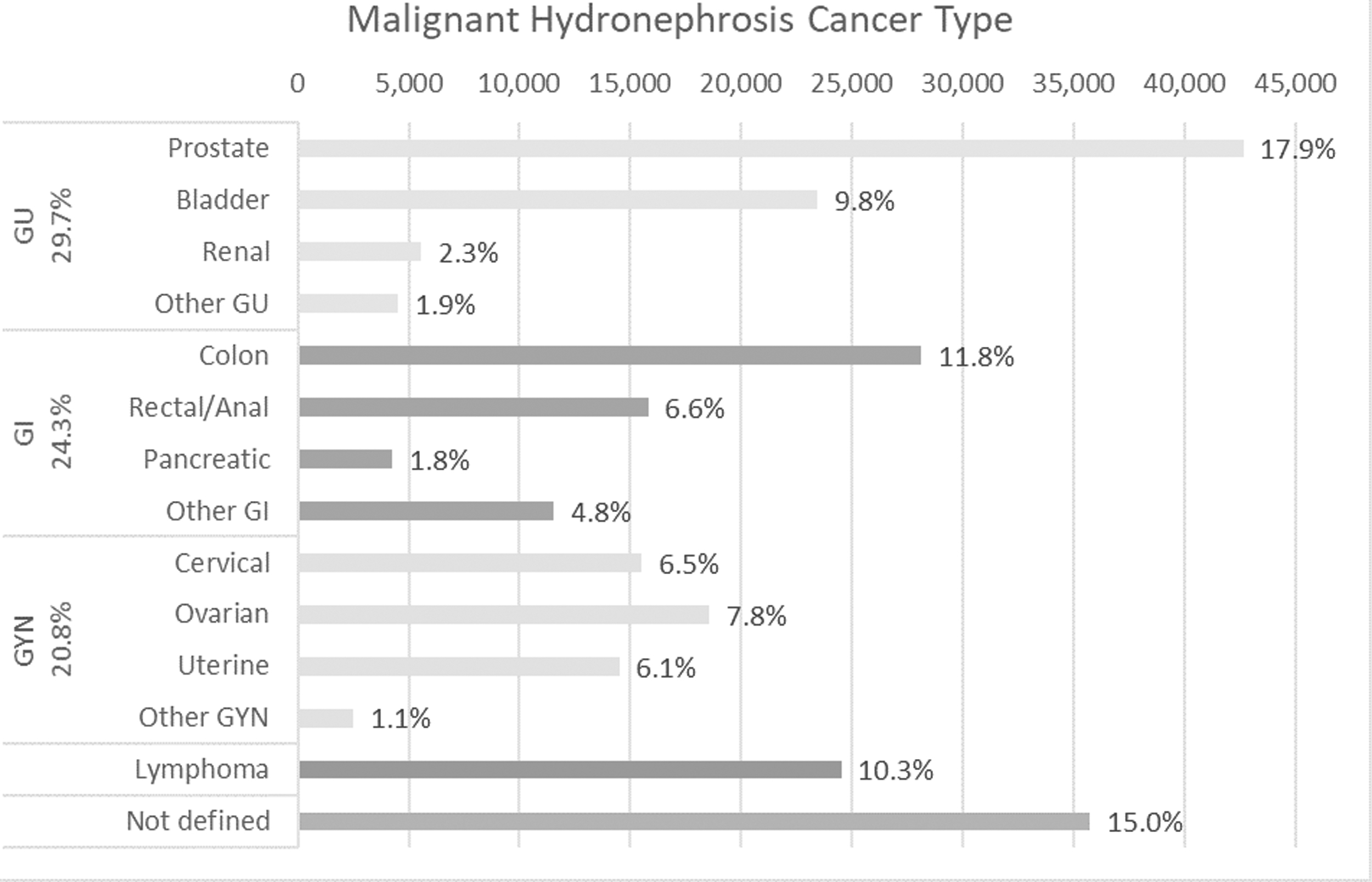
Malignant hydronephrosis prevalence by specific cancer type.
Descriptive characteristics of the patient population stratified by malignancy type are presented in Table 2. Patient's with urologic malignancies were the oldest (mean 71.5 years), among the most comorbid, and had the highest rates of CKD (33.6%), AKI (53.5%), and UTI (39.0%) compared with other cancer groups (all p < 0.001). Despite the high degree of comorbidity in this group, patients with urologic malignancies had the shortest mean hospital stay at 7.6 days, least expensive hospital costs at 62K, and the lowest in-hospital mortality rates at 6.2%. In contrast, the highest mortality rate group (10.7%) was seen in the other/not defined group perhaps reflecting a portion having end-stage cancer in which biopsy was deferred in favor of a hospice approach.
Descriptive Characteristics of Cohort by Cancer Type
CHF = congestive heart failure; CKD = chronic kidney disease; GI = gastrointestinal, GU = genitourinary; GYN = gynecologic; IQR = interquartile range; NT = nephrostomy tube; RUS = retrograde ureteral stent; SD = standard deviation; s/p = status post.
There was noteworthy variation in the percentage of patients who were decompressed and the ratio of RUS/NT among different cancer types as detailed in Figure 2. Gynecologic malignancies were the most likely cancer type to be decompressed with a decompression rate of 32.6% followed by GI cancer (30.1%), GU cancer (28.1%), and lymphoma (26.9%). Metastatic urologic malignancies were the only cancer category that tended to prefer initial decompression with NT over RUS (RUS/NT = 0.82), indicating that when decompression was done, NT was used 1.2 × more frequently than RUS. Bladder cancer had both the highest absolute rate of decompression with NT at 17.6% and a 1.6 × preference for NT over RUS. Decompression with RUS was most strongly favored in lymphoma (RUS/NT = 2.98), followed by GI cancers (RUS/NT = 2.32).
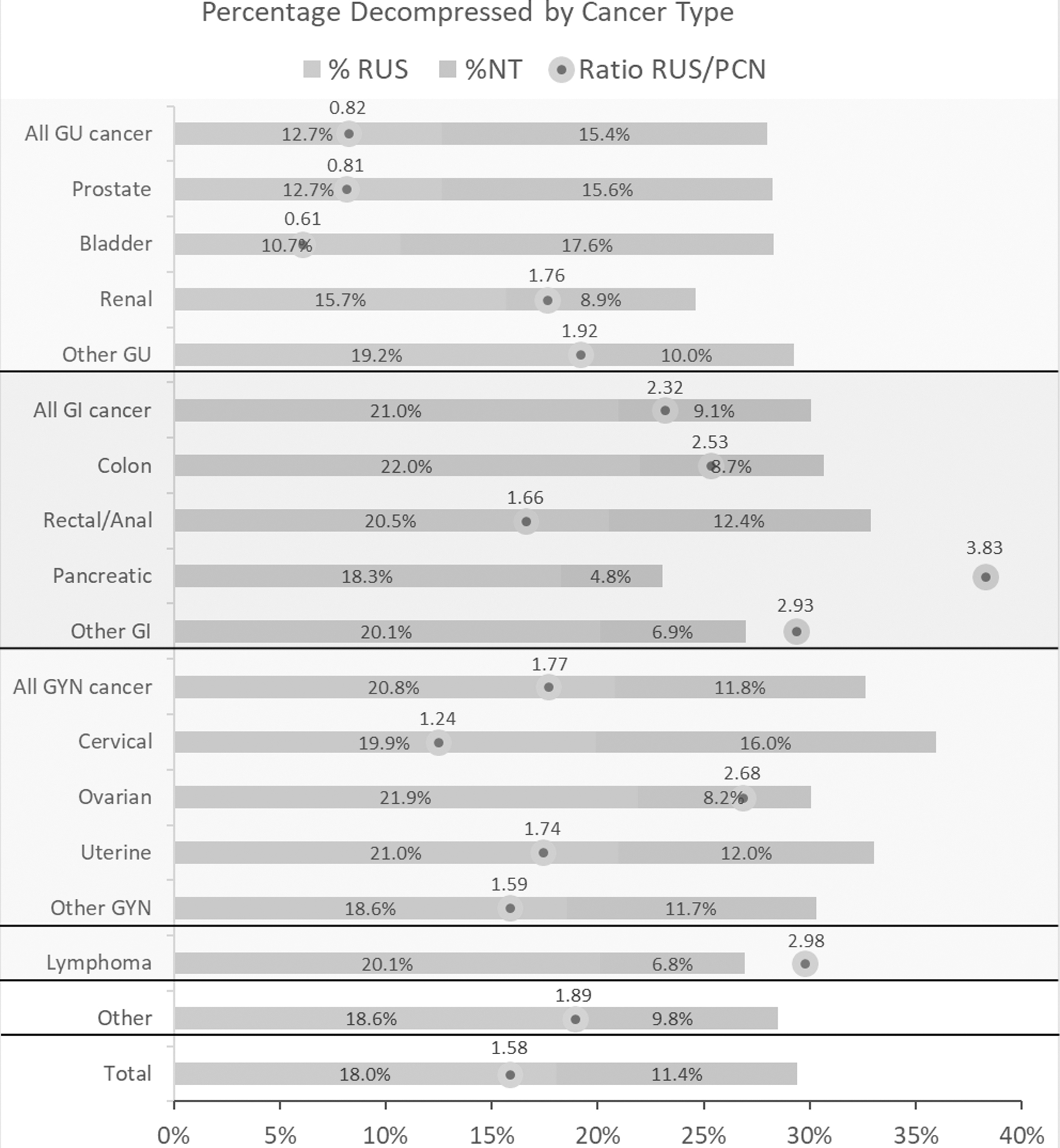
Percentage decompressed with RUS and NT by cancer type. NT = nephrostomy tube; RUS = retrograde ureteral stent.
Multinomial regression identified significant predictors for RUS vs NT vs no decompression, with no decompression as the referent (Fig. 3, * indicates significance at p < 0.05). Among the statistically significant findings (all odds ratios [ORs] listed here significantly were <0.05 unless stated otherwise, see Fig. 3 for 95% confidence intervals), there were increased odds of RUS among female patients (OR 1.42), obese patients (1.12), patients in the Midwest (1.39) and South regions (1.17), and in patients with lymphoma (1.14), ovarian (1.17) and colon cancer (1.38). Conversely, parameters that predicted decreased odds of undergoing decompression with RUS included Medicaid insurance (0.82) and patients with bladder cancer (0.67).
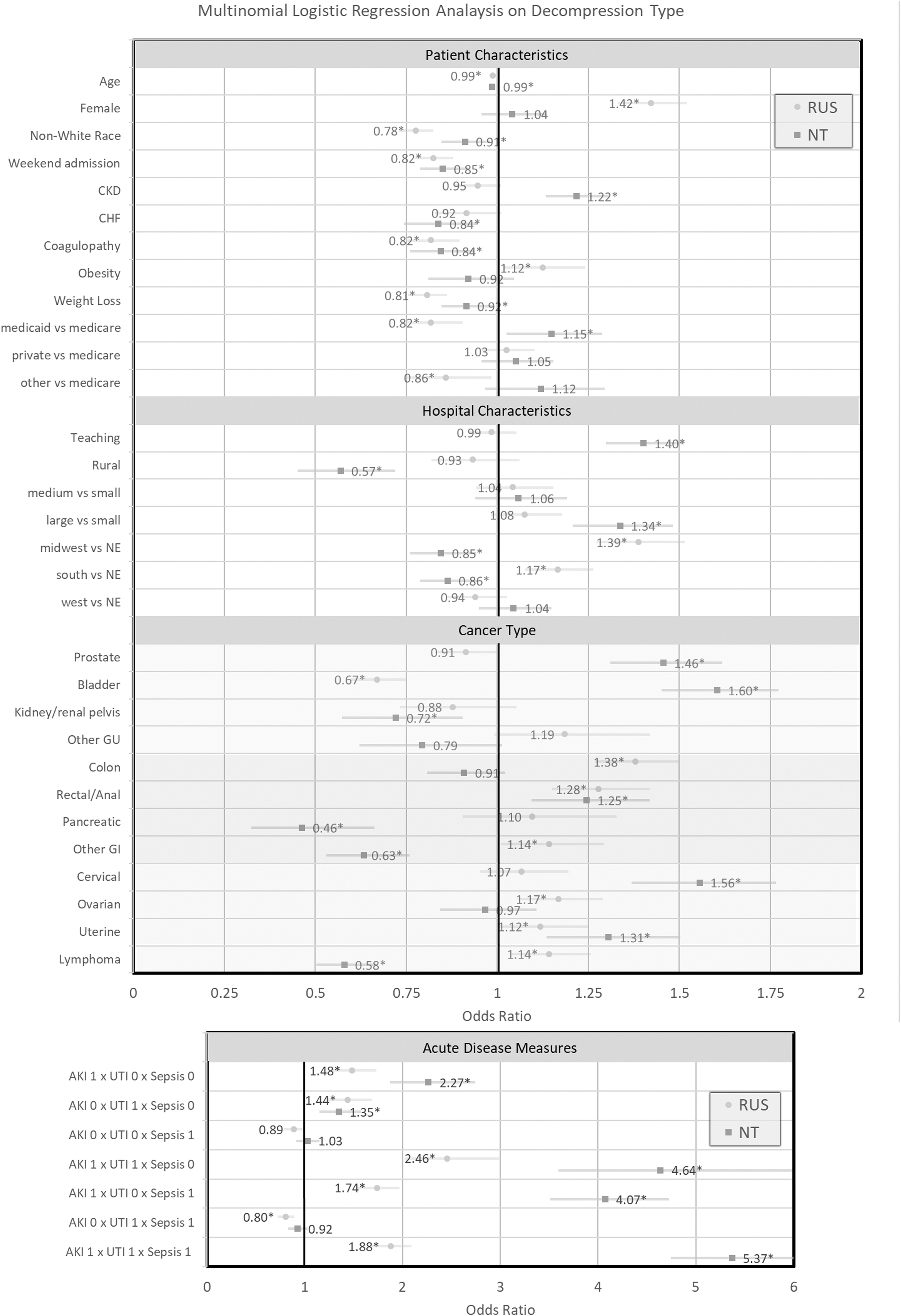
Forest plot of weighted multinomial logistic regression analysis on decompression type. No decompression is the referent. Bars represent 95% confidence intervals; *Indicates odds ratio significance at p ≤ 0.05. CKD = chronic kidney disease; CHF = congestive heart failure; NE = northeast; AKI = acute kidney injury; UTI = urinary tract infection.
There were increased odds of undergoing NT among patients with CKD (OR 1.22), Medicaid insurance (1.15), in teaching hospitals (1.40), larger hospitals (1.34), and in patients with prostate (1.46), bladder (1.60), cervical (1.56), and uterine cancer (1.31). Conversely, parameters that decreased the odds of NT included hospitals in a rural setting (0.57), the Midwest (0.85) and South (0.86) regions, in addition to cancer types of kidney/renal pelvis (0.72), pancreatic (0.46), and lymphoma (0.58).
As the multinomial regression used observation as the referent, it was possible for parameters to exhibit both increased or both decreased ORs for RUS vs NT. Factors that decreased the odds of decompression with either modality included nonwhite race (RUS OR 0.78 vs NT OR 0.91), weekend admission (0.82 vs 0.85), comorbidities of coagulopathy (0.82 vs 0.85), and weight loss (0.81 vs 0.92). Analysis of the interaction terms of the acute disease parameters of AKI, UTI, and sepsis revealed AKI to be the strongest driving force for decompression with increasing ORs as UTI and sepsis were also present, with the highest OR observed when all parameters were present (1.88 vs 5.37). Greater degree of acute illness favored decompression over no decompression with NT generally preferred over RUS.
Regarding temporal trends (Fig. 4), there was an increase in the overall prevalence of MEUO from an initial average quarterly n = 9610 in 2010 to n = 11,070 in 2015, representing an average annual percentage increase of 3%. On the contrary, the percent of MEUO that was decompressed in the inpatient setting was found to be decreasing, with a mean annual percent decrease of decompression of −2.4%. This change was driven almost entirely by a decrease in the proportion of patients decompressed with RUS (mean annual percent decrease of −3.8%) as the proportion of patients decompressed with NT held steady.
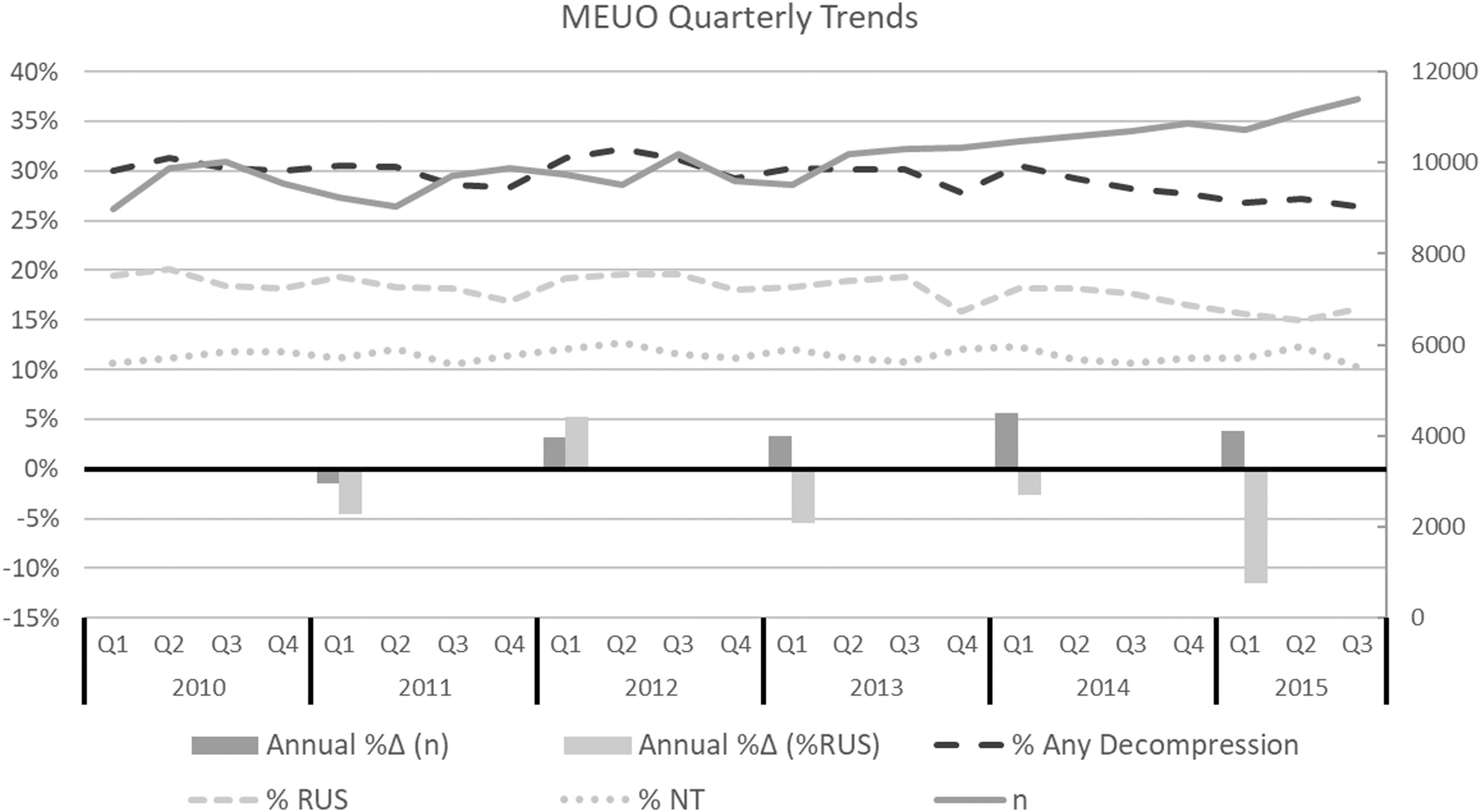
Quarterly trends in decompression of MEUO. MEUO = malignant extrinsic ureteral obstruction.
Discussion
This study represents the largest assembled MEUO cohort to date by orders of magnitude with significant power to detect a wide range of variation in practice patterns. Interestingly, most cases (70.6%) received no decompression of hydronephrosis during inpatient hospitalization. This high rate of observation can be accounted for in several scenarios: those with milder cases of MEUO with decompression deferred to the outpatient setting, sicker patients with more pressing clinical issues or with palliative care intent, or prior decompression with chronic dilation. Furthermore, it was also not possible to elucidate the likely small proportion of patients who presented with hydronephrosis despite prior placement of RUS or NT and may have received either an exchange or a conversion of diversion type.
A wide degree of variation in the management of MEUO was observed at the hospital and regional levels. Unsurprisingly, teaching (academic) and large hospitals utilized more NT, both because of the greater availability of interventional radiology and also perhaps because of traditional academic teaching that favors MEUO decompression with NT over RUS. Surprisingly, there was significant regional variation as the Midwest and South preferred RUS over NT, while the West and East coasts had similar rates of NT and RUS.
Among all malignancy types, prostate and bladder cancer had the highest rates of initial decompression choice of NT over RUS. Reflecting a component of internal obstruction in some cases of metastatic bladder and prostate cancer, urologists may prefer decompression with NT for its greater reliability for initial and long-term success. Despite attempts to remove patients with internal obstruction by excluding cases with ICD-9 procedure codes indicating internal resection, there likely remained a small portion of patients with internal obstruction that could not be accounted for based on ICD-9 coding. The third-most common cancer type in which NT was performed was metastatic cervical cancer, which in locally advanced cases can obstruct the ureteral orifices via direct invasion. Although cervical cancer was preferentially decompressed with RUS on univariate analysis with an RUS/NT ratio of 1.24, it had the second highest cancer-related OR on multivariable analysis of 1.56. In contrast, malignancies with low likelihood of internal obstruction—such as GI cancers, ovarian cancer, and lymphoma—had the higher rates of RUS compared with NT on univariate and multivariate analysis.
Decompression of malignant hydronephrosis is often a semielective procedure rather than an urgent matter such as decompression of obstructive pyelonephritis. This is reflected in the finding of weekend admission decreasing odds of decompression with both RUS (OR 0.82) and NT (0.85). However, there are scenarios of MEUO with severe AKI, pyelonephritis, and/or urosepsis that warrant prompt decompression in the inpatient setting, and this is reflected in our analysis. Our analysis also shows that NT is clearly preferred to RUS in patients with more of these acute disease measures present.
In looking at the national trends, the prevalence of MEUO in the United States has undoubtedly been rising in tandem with the aging baby boomer generation at an estimated average annual rate of 2.9%. Perhaps with increasing awareness of the futility/unnecessary morbidity of decompression in certain scenarios or continued evidence emerging for significant rates of RUS failure, 4,16 the rate of decompression with RUS has been decreasing at an annual average of 3.8%, while the rate of decompression with NT has held nearly constant.
Although this study excels in providing benchmarks and trends from its large sample size, it is limited by the inherent design of the NIS and administrative data sets more generally. Particular to the NIS in which each discharge record is a unique deidentified data point, it is impossible to track longitudinal patient outcomes of readmission rates and survival rates. Moreover, data granularity is restricted by coding for ICD-9 codes, which do not give important details such as severity of AKI and decompression's impact on its resolution, radiographic findings of hydronephrosis laterality and severity, and laterality/bilaterally of RUS or NT insertion.
The decision to decompress MEUO with either RUS or NT or observe is complex—the urologist should incorporate shared decision-making involving the patient's overall prognosis and wishes, acuity of the clinical scenario, and likelihood of success to provide meaningful additional quantity and/or quality of life to the patient. As such, our study cannot comment on the optimal approach for each patient scenario. This study shows that NT vs stent is preferred in different clinical scenarios (i.e., in malignancies where concomitant internal obstruction may be present and in more acute settings of AKI and sepsis) and this may give guidance to providers unfamiliar with this area; however, comparative effectiveness of modality is outside the scope of this study. To make comparisons of outcomes such as the mortality rate between RUS vs NT would be misleading because of the high degree of selection bias between modalities that cannot adequately be controlled for in such a data set.
Conclusions
There is substantial variation in decompression approaches for MEUO among patient, hospital, and disease types. A preference for NT was observed in larger academic institutions for nonwhite and Medicaid patients with bladder, prostate, or cervical cancer, while RUS was preferred in female patients, and those with lymphoma, ovarian, or colon cancer. While the prevalence of MEUO has increased from 2010 to 2015, the overall proportion of decompression for MEUO has been driven by a decreased use of RUS. Further investigation into best approaches for certain patient characteristics and disease types will help to standardize care and reduce disparities.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.