
Abstract
Introduction and Objectives:
To determine the optimal guidewire for bypassing an impacted ureteral stone.
Materials and Methods:
Three different benchtop models of varying impaction (300, 362, and 444 mm Hg pressure) were used to compare the ability of 13 different guidewires to bypass an impacted ureteral stone. In the first and second models, we recorded the maximum force required to bypass the stone. In the first model (300 mm Hg) 10 new wires for each of the 13 types were advanced past a ureteral stone using a series 5 digital force gauge. In the second model (362 mm Hg), the top 5 performing guidewires were similarly tested. In the third model (444 mm Hg), 5 attending urologists and 5 urology residents (blinded to wire type) compared the 13 guidewires and rated the wire performance using a Likert scale. Statistical analysis was performed with analysis of variance and the chi-square test.
Results:
In the first model, there was a significant difference between wires (p < 0.001) with the lowest mean force to bypass a stone seen in the Glidewire (0.117 ± 0.02 lbs) and HiWire (0.130 ± 0.01 lbs). Of the five wires tested in the second model, the Glidewire (0.24 ± 0.09 lbs) and UltraTrack (0.40 ± 0.35 lbs) both required less force than the other three wires (p = 0.018). In the third model, only two wires (Roadrunner and Glidewire) bypassed the impacted stone in 100% of trials. When comparing standard, hybrid, and hydrophilic wires, the hydrophilic had the highest success rate (standard = 0%, hybrid = 36.67%, and hydrophilic = 70.67%; p = 0.000) and Likert score (standard = 1.03, hybrid = 2.38, and hydrophilic = 3.24; p = 0.000). Hydrophilic wires required the least time to bypass the stone (hybrid = 82.81 seconds vs hydrophilic = 45.37 seconds, p = 0.000).
Conclusions:
In this benchtop study, standard wires performed poorly and hybrid wires were not as effective as hydrophilic wires. The Glidewire required the least force, the shortest insertion time, and had the highest surgeon satisfaction rating.
Introduction
Urolithiasis is a prevalent condition, and urologists are often called upon to place ureteral stents to establish drainage of the collecting system from an impacted and obstructing stone. 1 Recent literature has demonstrated an increase in the prevalence and incidence of kidney stones on a global scale. 2 In the United States alone, urolithiasis has been increasing at a rate of ∼5% to 10% annually. 3 Impacted ureteral stones can pose a great risk to the patient causing acute renal injury and sepsis but also if untreated, are associated with ureteral strictures and irreversible deterioration of renal function. 4 This may result in the need for a nephrostomy tube, a delay in the patients care, and other serious consequences. 5 Impacted ureteral stones are also found to be associated with lower stone-free rates, higher complications, and longer operating times. 6
Guidewires are commonly used in urologic practice for a wide variety of applications, including establishing access beyond an impacted stone. Urologists routinely face the decision of which wire type to use to bypass an impacted ureteral stone. With multiple wires available, surgeons must account for the different characteristics of each wire to maximize efficiency while minimizing the risk of ureteral perforation. However, the effectiveness of these different wires in comparison with each other is not completely understood. In general, hydrophilic guidewires are the preferred choice when it is necessary to bypass an impacted ureteral stone and achieve safe access to the urinary system, because of their floppy tip and low friction coating. The nitinol core standard guidewires are selected for coaxial passage of catheters, stents, and sheaths. 7 However, some urologists prefer to use hybrid guidewires that have the properties of both lubricious and polytetrafluoroethylene (PTFE)-coated wires and can provide both lubricity and stiffness needed for passage of a catheter over the wire.
Each guidewire has variations in core, tip configuration, body, and coating material, which may affect their performance. 8 The optimal wire to bypass a ureteral stone has not been determined. The purpose of this study was to compare the effectiveness of 13 different guidewires to bypass a tightly impacted ureteral stone in a benchtop model.
Materials and Methods
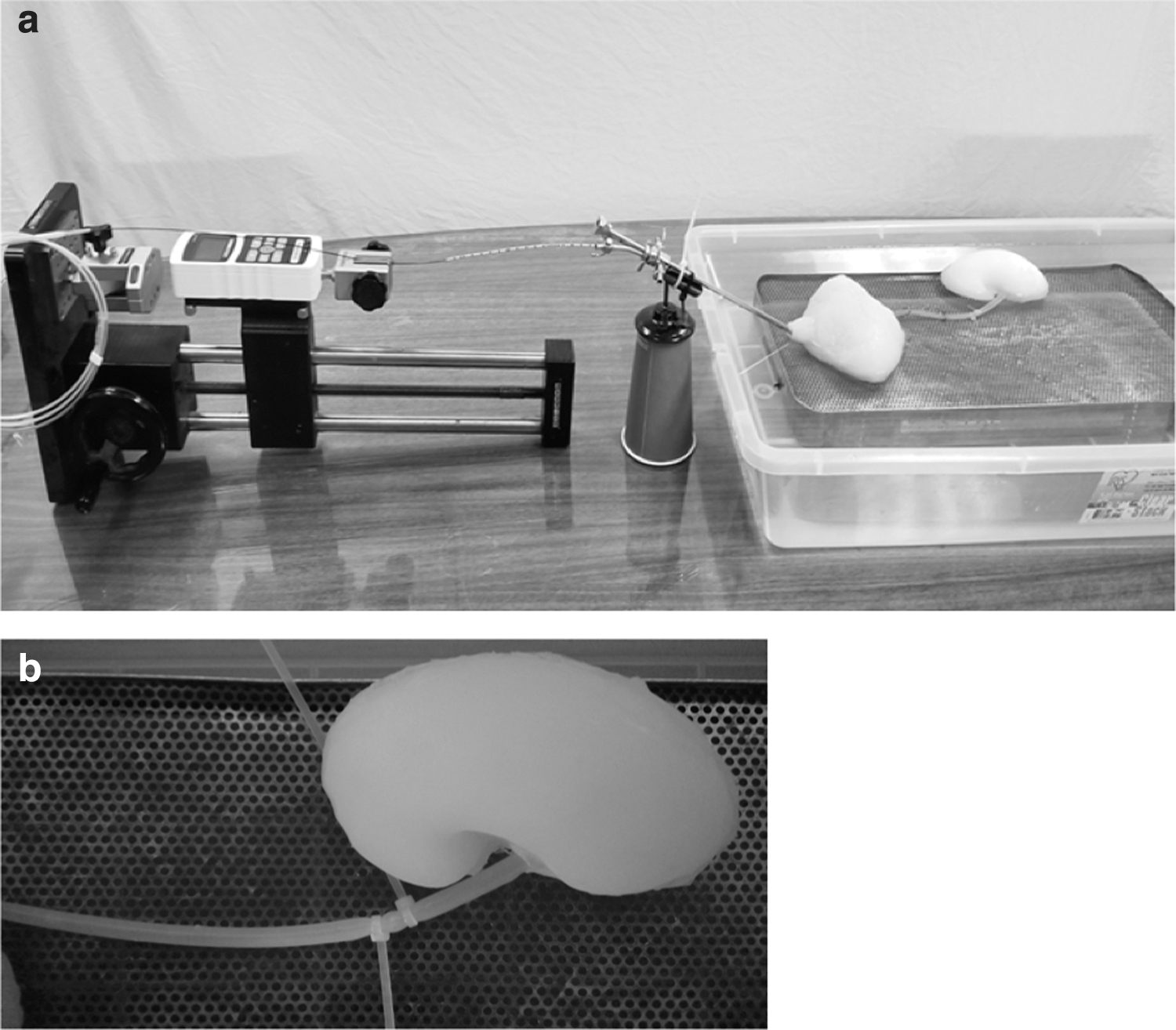
An impacted ureteral stone model was created using silicon ureters (8 mm diameter) configured and mounted on a backboard bathed in saline recreating an actual patient anatomy. Cable ties were placed above and below a 5 mm bego stone and were tightened to create obstruction adequate to resist the passage of saline at 300, 362, and 444 mm Hg (Fig. 1a, b). (A previous study has shown that the lowest amount of pressure to create impaction is 300 mm Hg. 9 ) Degree of impaction was confirmed by measuring the pressure at the proximal end of the ureter with a Uharbour digital pressure gauge. A ureteral catheter was placed in the cystoscope and used to deliver the wire to the impacted stone. The distance from the stone to the tip of the ureteral catheter (2 cm), the length of the ureteral catheter outside the cystoscope (15 cm), and the distance from the end of the cystoscope to the digital force gauge (20 cm) were the same in all trials.
Guidewires from four major manufacturers were compared, including Olympus (PTFE, Glidewire, UltraTrack), Cook (Fixed core, HiWire, Roadrunner, Motion), Bard (Fixed core, Hydroglide, Solo Plus, Solo Hydro), and Boston Scientific (Zipwire, Sensor) (Table 1). The investigator performing phases 1 and 2 was blinded to the wire brand and type. Similarly, the surgeons performing phase 3 were also blinded to wire brand and type.
Types of Guidewires
PTFE = polytetrafluoroethylene.
In the first model (300 mm Hg), 10 different new 0.038 straight-tipped guidewires of 13 different types were advanced past a ureteral stone using a series 5 digital force gauge. The endpoint was to measure the maximum force required to bypass the impacted ureteral stone for each guidewire. This mild degree of impaction was used to compare all 13 wire types.
Because the degree of impaction in the first model was low, it could not be used to stratify the best performing wire. Subsequently, a second model was constructed with a moderate degree of impaction (362 mm Hg) to perform a playoff between the top 5 best performing wires in the first model. Ten additional trials were performed for each of the guidewires.
In the third model, designed to simulate a high-degree impaction (444 mm Hg), 5 attending urologists and 5 urology residents (blinded to wire type) were given 3 attempts to pass the impacted stone with each of the 13 guidewire types. The maximum time allowed to complete each trial was 2 minutes. The three measured endpoints included the success rate of wire passage across the impacted ureteral stone, time for wire passage, and subjective surgeon rating of wire performance using a Likert scale (1, least preferred to 5, most preferred).
Statistical analysis was performed with analysis of variance (ANOVA) with p < 0.05 defined as significant. ANOVA post hoc analysis was carried out with Tukey's B method. Success rates were compared using the chi-square test.
Results
In the first model (300 mm Hg), the Glidewire (0.117 lbs) and HiWire (0.130 lbs) passed the impacted stone with the lowest mean force compared with all other wires (p < 0.001) (Fig. 2).
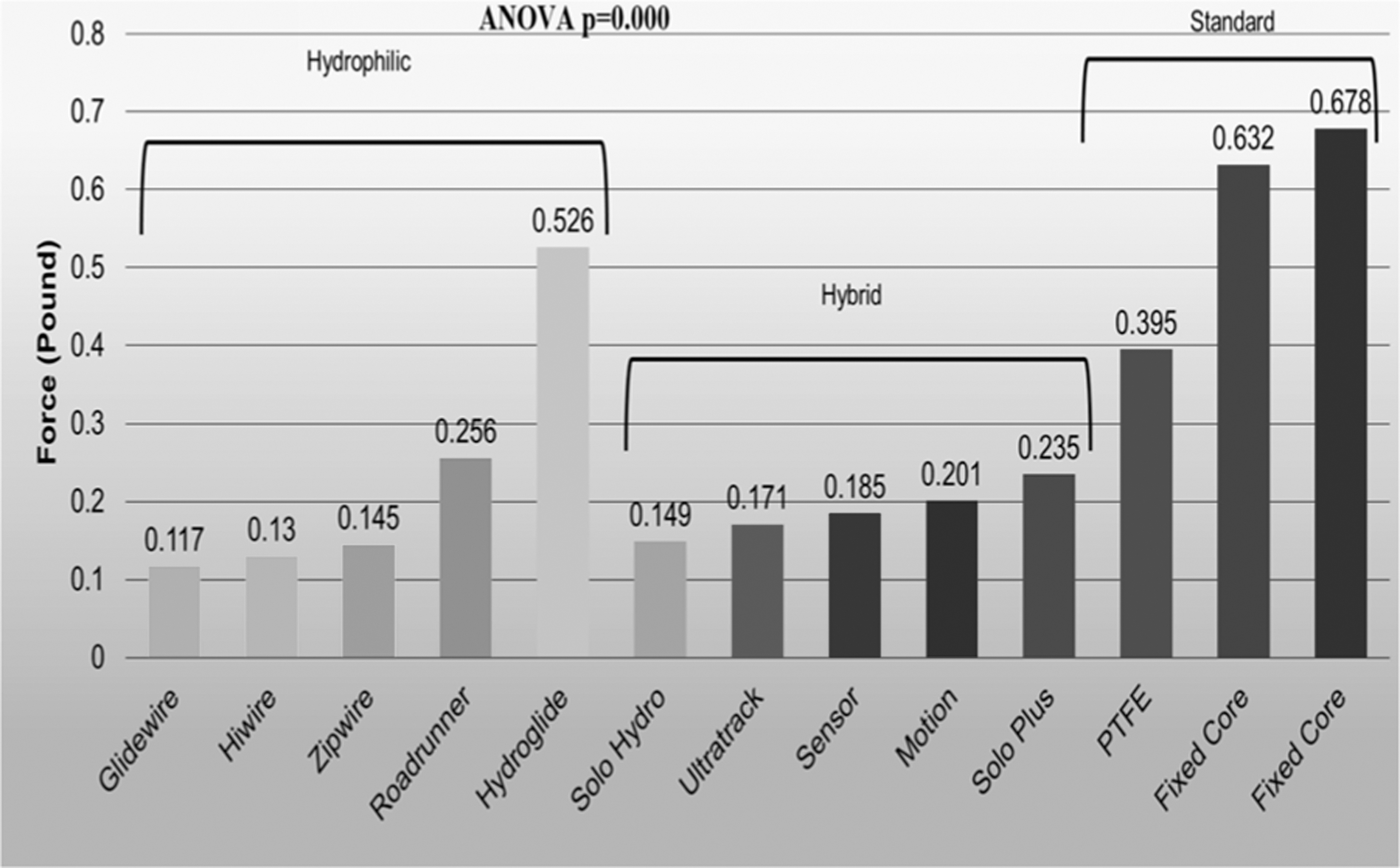
Comparison of 13 different guidewires in the first model (300 mm Hg) to assess the required force to pass the stone. ANOVA = analysis of variance; PTFE = polytetrafluoroethylene.
In the second model (362 mm Hg), of the five wires tested, the Glidewire (0.24 ± 0.09 lbs) and UltraTrack (0.40 ± 0.35 lbs) required less force than the other three wires (p = 0.018). Conversely, the Solo Hydro wire required the highest force of 0.65 pounds to bypass the impacted stone (Fig. 3).

Comparison of the top 5 guidewires in the second model (362 mm Hg) to assess the required force to pass the stone.
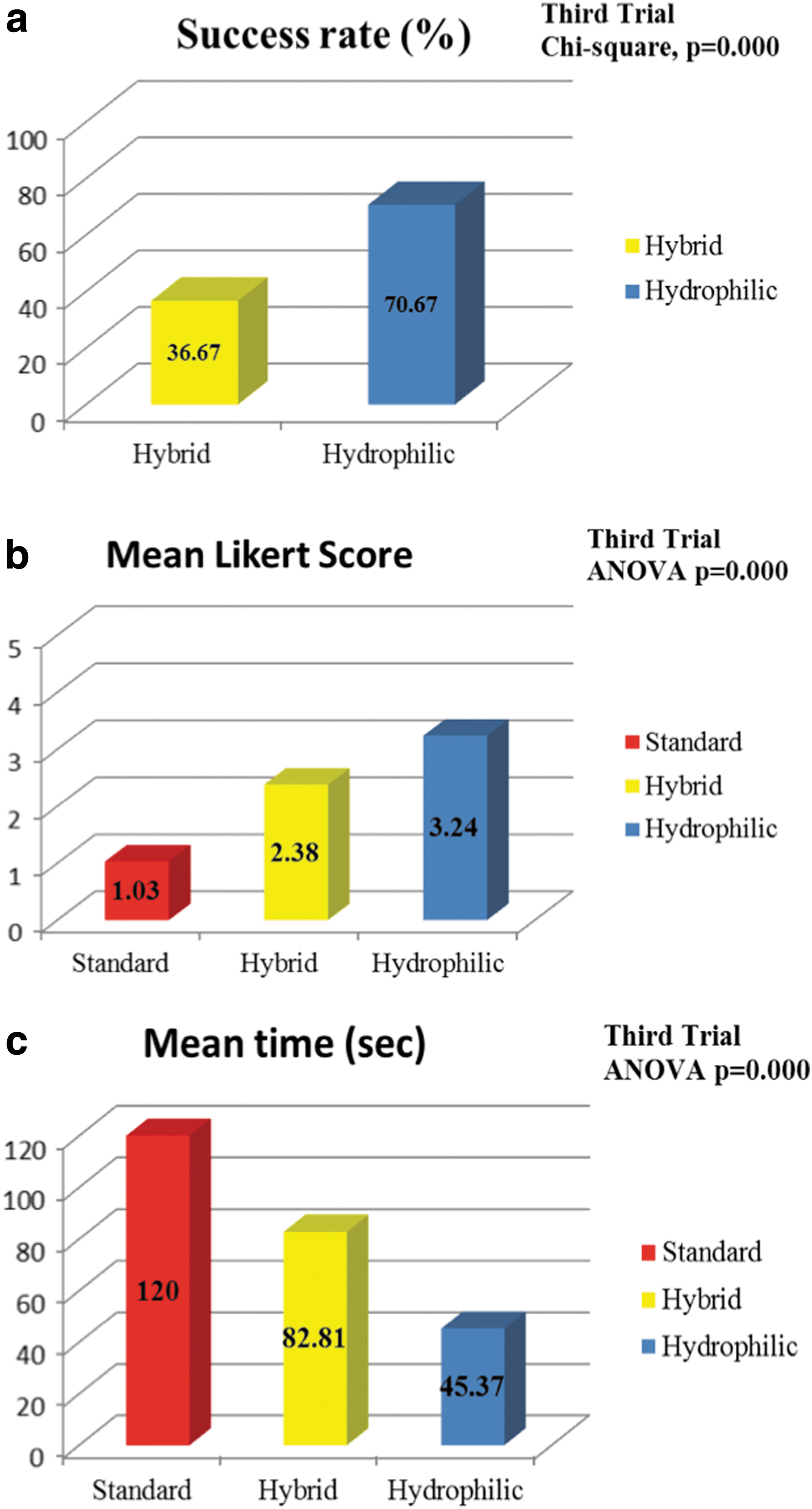
In the highly impacted third model (444 mm Hg) comparison of the different wire types demonstrated that hydrophilic wires had the highest success rate (hydrophilic = 70.67%, hybrid = 36.67%, standard = 0%; p = 0.000). Hydrophilic wires also had the highest Likert scores (hydrophilic = 3.24, hybrid = 2.38, standard = 1.03; p = 0.000) (Fig. 4a, b). Finally, hydrophilic wires were passed more quickly (45.37 seconds) compared with the hybrid wires (82.81 seconds, p = 0.000; Fig. 4c). The standard wires were not able to be passed in the third model.
Only two wire types were able to be passed in 100% of trials in the third model, the Glidewire and the Roadrunner (Fig. 5). The Glidewire required the least time for wire passage (5.18 ± 5.34 seconds, p < 0.01) and had the highest subjective surgeon rating (Likert scale: 5.0, p < 0.01) compared with all other wire types (Fig. 6). Table 2 provides the outcomes of the third model. Furthermore, we compared the results of the residents and attending urologists. The overall success rates in the third trial between residents and attending urologists were similar (42.6% vs 40%, p = 0.681). Their top 2 preferences were also the same [Glidewire (Likert 5 vs 5) and Roadrunner (Likert 4 vs 3.8)].
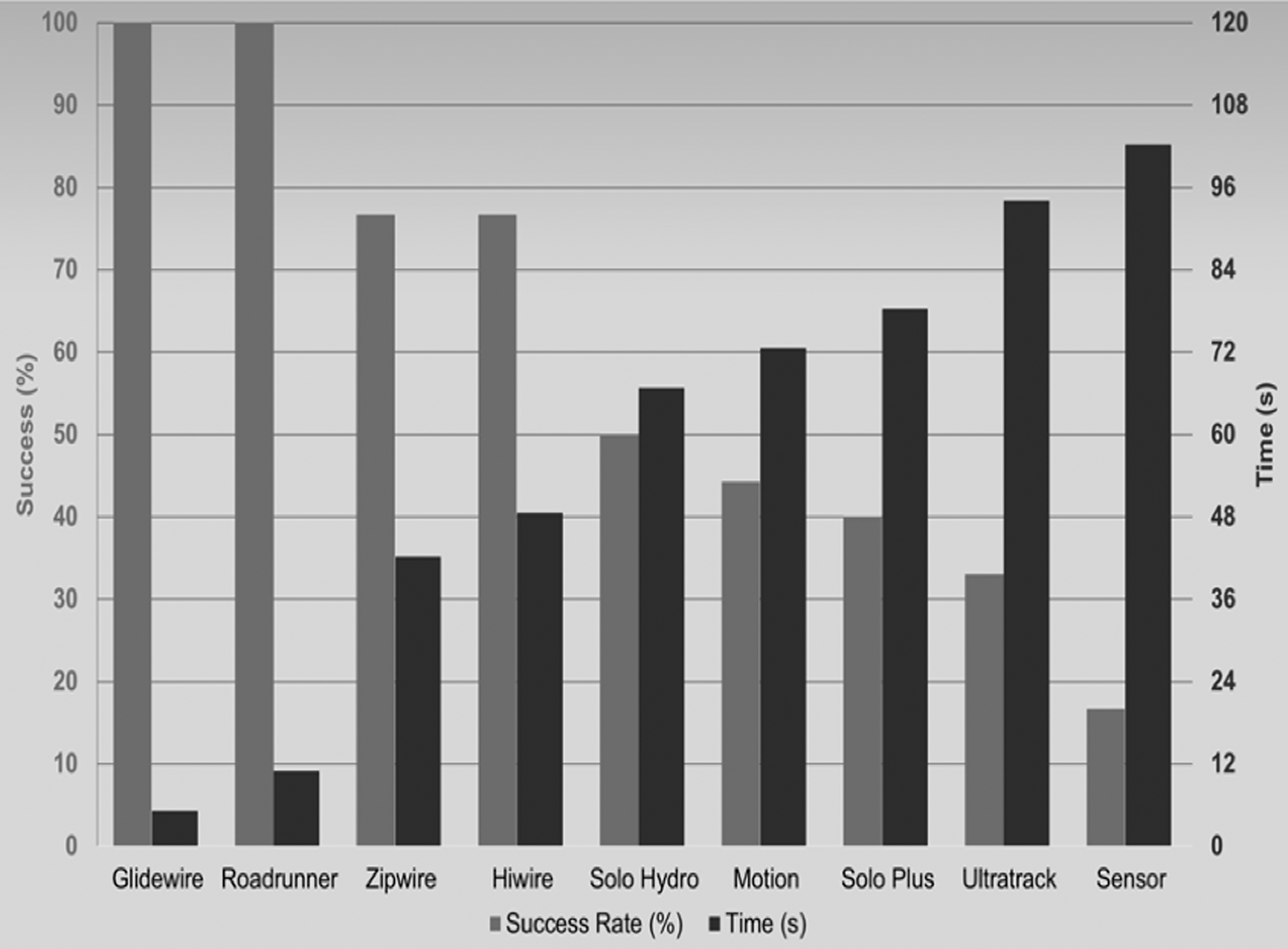
Comparison of guidewires that passed the stone in the third model (444 mm Hg). Average success rate and time required for guidewire passage.
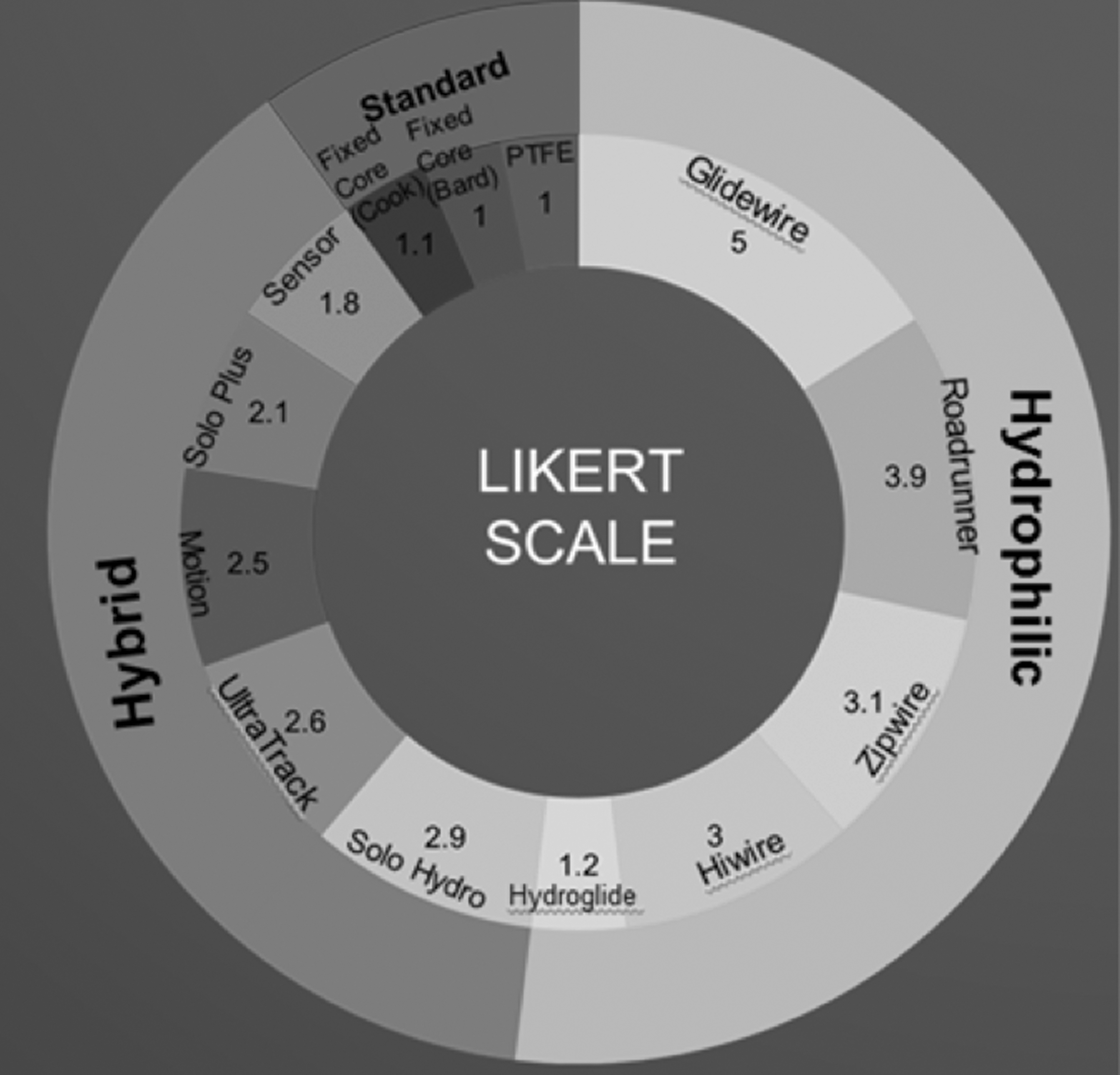
Comparison of all 13 guidewires in the third model (444 mm Hg). Average assigned Likert rating from the surgeons
Outcomes of the Third Model (Surgeon's Hands-On Trial)
NA = not available; SD = standard deviation.
Discussion
Impacted ureteral stones represent a difficult challenge and have a higher risk of complications including pain, urinary tract infections, bleeding, sepsis, ureteral stricture, and kidney failure. 6,10,11 Patients with impacted ureteral stones have a higher rate of ureteral perforation and avulsion compared with patients with nonimpacted stones. 11 Failure to provide surgical decompression in a timely manner increases the risk of both morbidity and mortality in patients with infected obstructing ureteral calculi. 12 The first and often most difficult step of retrograde ureteral access is passage of the wire beyond the stone. This highlights the importance of establishing secure guidewire access beyond the stone without perforation. Subsequently, the impetus of this study was to determine the optimal guidewire to bypass an obstructed impacted ureteral stone.
Our study demonstrated that lubricious wires when compared with hybrid wires required less force, less time, and had a higher success rate in bypassing an obstructing impacted stone. In addition, our results showed that conventional Teflon-coated wires required significantly more force, required more time, and had lower success rates compared with both lubricious and hybrid wires. Of the lubricious wires, the Glidewire and Roadrunner wires required the least insertion time, the least force, and had the highest success rate.
Guidewires used in urologic cases vary by their mechanical properties and safety profiles. Because no standard classification system exists for guidewires, we divided the wires into three subcategories: hydrophilic, hybrid, and standard wires. Hydrophilic wires have a solid nitinol or metal alloy core, with a durable hydrophilic coating that decreases the frictional coefficient when wet. 13 Monga and colleagues 13 showed that guidewires (both stiff and regular shaft) have the lowest potential for perforation in their benchtop model. However, because the entire hydrophilic wire is slippery, they may be more difficult to use as a working or safety wire and more prone to dislodgement. 13
In comparison with hydrophilic guidewires, hybrid guidewires combine an atraumatic hydrophilic tip with a stiffer PTFE Teflon-coated nitinol shaft. 14 This wire design subsequently requires a junction point between the lubricious-coated tip and the Teflon-coated shaft. The effect of this transition upon the ability to bypass an impacted stone has not been previously determined. A previous benchtop study demonstrated that hybrid wires (U-Nite and Sensor) had less stiff shafts than the Amplatz super stiff. They were also more prone to perforation necessitating less force to puncture aluminum foil compared with a purely hydrophilic guidewire (RadiFocus). 15 However, no previous model has determined whether these wires are as effective at bypassing an impacted stone. Our model demonstrates that the hybrid wires do not bypass an impacted stone as effectively as the purely lubricious wires. In some trials, we observed that even if the tip of the hybrid wire was advanced past the impacted stone, the junction of the flexible tip and Teflon-coated shaft created a friction point that would not allow this transition point to slip above the stone.
The third wire type in common use is the standard Teflon-coated guidewire. These wires have a flexible tip and stiffer stainless steel shaft. The primary advantage of these standard wires is that they provide a relatively stable working and safety platform at a relatively low cost. A previous benchtop study showed that standard Teflon-coated guidewires required less puncture force through aluminum foil, indicating the higher ureteral perforation risk compared with hydrophilic and hybrid wires. 7 These wires may function well as a safety wire, but given our findings, they are not the most effective wire to bypass a tightly obstructing stone. In fact, use of these wires could substantially increase the risk of perforation.
Recently, Chandhoke and colleagues found that peri-calculus ureteral thickness on CT is predictive of ureteral stone impaction and useful for surgical planning. 16 In another recent study, a formula was developed to predict stone impaction by combining the grade of hydronephrosis, ureteral wall density in HU, and ureteral wall thickness. Using this formula, authors predicted the impacted stone cases with a sensitivity and specificity of 91% and 97.7%, respectively. 17 Subsequently, it is possible to preoperatively predict whether the stone is impacted using CT criteria. When impacted stones are demonstrated on CT imaging, our study demonstrates that lubricious wires should be the wire of choice to facilitate passage of the impacted stone.
Inappropriate selection of guidewires can unnecessarily contribute to the morbidity of ureteroscopy or ureteral stenting in patients with impacted stones, necessitating higher level of care secondary to ureteral perforation or avulsion. The reported rates of perforation during ureteroscopy have ranged from 1.5% to 13%, whereas the avulsion rate is <1%. 18 In the setting of an impacted stone with infection, timely decompression can be a life-saving therapeutic measure. Use of a suboptimal guidewire could delay decompression. For example, if a surgeon was unsuccessful in bypassing an impacted stone using a hybrid wire, they might incorrectly conclude that a nephrostomy tube and a secondary procedure were required for decompression. In contrast, use of a lubricious wire like the Glidewire, could avoid a secondary procedure.
Efficiency in the operating room (OR) is another important factor, as the mean cost of OR time is $37 per minute. 19 The perceived vs actual cost of devices is also often overlooked. Elsamra and colleagues recently demonstrated that neither attending nor resident urologists are able to accurately estimate the cost of commonly used disposable devices. 20 Selecting the optimal guidewire for bypassing an impacted ureteral stone has the potential to improve patient outcomes while shortening procedure time and lowering cost. In contrast, selecting the wrong wire could increase the risk of perforation and substantially increase the operative time and cost. Failure to bypass an impacted stone with a guidewire could add several thousand dollars of cost and additional time for the placement of a nephrostomy tube. Therefore, selecting the optimal wire initially will reduce disposables and operative time, resulting in a lower cost to the patient and hospital.
When evaluating the cost in our institution, the Sensor wire with a cost of $76.38 per wire, required an average of >100 seconds for wire passage in the 17% of times that it passed successfully. In contrast, the Glidewire and Roadrunner with a cost of $63 and $37.13 per wire, respectively, each had a wire passage success rate of 100%, with mean passing times of 5.18 and 10.94 seconds, respectively. Because the Sensor wire required six attempts (2 minutes per failed attempt and 1.7 minutes for successful attempt) to bypass an impacted stone, necessitating more OR time that will result in higher cost [$76.38 + ($37/minute OR time × 11.7 minute) = $509.28/renal unit]. However, the Glidewire and Roadrunner will require less OR time and cost to bypass an impacted stone [Glidewire: $63 + ($37/minute OR time × 0.086 minute) = $66.19/renal unit and Roadrunner: $37.13 + ($37/minute OR time × 0.18 minute) = $43.87/renal unit].
Although to our knowledge, this study includes the largest selection of urologic guidewires tested in a benchtop model, one of the limitations of our study is not including every type of urologic wire available globally. We tested 13 commonly used guidewires; however, there may be wires that are used by other urologists that were not included in our study. In addition, this is a benchtop model with all the limitations arising from use of a model. Although we ensured the ureter size, orientation (bathed in saline), and material (silicon) to resemble the human ureter as closely as possible, it may not perfectly replicate all the factors encountered in an actual patient. In the third model, a surgeons' experience may have also played a role in the time and force required to bypass the impacted stone; however, this was minimized by use of multiple surgeons with varying experience level, resident physicians, and multiple attempts. Although we attempted to perform all trials in a blinded and objective manner, there are some unique characteristics of certain wires (i.e., Roadrunner), which reduce the effectiveness of the blinding process. Despite this fact, many of the wires physically appear similar to other wire types. For example, the Glidewire, Zipwire, and HiWire would be difficult to differentiate even for an experienced endourologist. Furthermore, the residents who had no previous exposure to the majority of the wire types tested in this study had similar results compared with the attending physicians. This supports the objectivity of our results.
Finally, our cost analysis includes only the costs of the wire used to bypass the impacted stone. Although stents may be placed over all types of wires including lubricous wires, surgeons may prefer to convert the lubricious wire to a working wire before proceeding with stone treatment, which would increase overall cost.
It is also important to understand and consider the availability of these products in the hospital and outpatient setting before applying these results clinically. Varied geographical preferences, cost, access to representatives for troubleshooting, and surgeon familiarity all play a role in the current climate of guidewire selection. In light of these considerations, our study highlights the importance of using the optimal guidewire when managing patients with impacted ureteral stones. The selection of the optimal wire will serve to improve patient outcomes, reduce health care costs, minimize complications, and maximize efficiency.
Conclusion
The selection of the appropriate guidewire for treatment of an impacted ureteral stone is critical. Failure to select the optimal guidewire for an impacted stone may increase the risk of ureteral perforation, complications, and cost. We found that hydrophilic wires had the highest success rates, shorter mean times for passage, and higher surgeon satisfaction. Of the lubricious guidewires, we demonstrated that the Glidewire required the least force, had the shortest insertion time, and had the highest surgeon satisfaction rating.
Footnotes
Author Disclosure Statement
This study was sponsored by Olympus Corporation of the Americas. Equipment and financial resources were provided by Olympus Corporation of the Americas.
Funding Information
No funding was received for this article.