
Abstract
Background:
To present a stepwise description and outcomes of bladder neck sparing (BNS) robot-assisted simple prostatectomy (RASP).
Methods:
Between March 2015 and December 2018, 30 consecutive patients with benign prostate hyperplasia underwent BNS RASP. Baseline characteristics, and intraoperative and postoperative variables were retrospectively abstracted. Descriptive statistics were used to report the variables.
Results:
The median age was 66.5 (59.3–72.3) years, and median body mass index was 27.6 (24.5–72.3) kg/m2. The median preoperative International Prostate Symptoms Score was 23 (17.5–27), and median prostate size was 97 (74–148.75) mL. The mean (standard deviation [SD]) operative time was 107.5 (22.2) minutes, and the mean (SD) estimated blood loss was 132.4 (35.4) mL. All cases were completed robotically without any intraoperative complications, and continuous bladder irrigation was not necessary for any patient postoperatively. All patients were able to void after catheter removal except one patient with a preexisting diagnosis of neurogenic bladder who resumed clean intermittent catheterization. All patients were continent as defined as using 0 pads postoperatively. Of the 19 patients who had antegrade ejaculation before the operation, 8 patients (42%) reported of continued antegrade ejaculation after the operation.
Conclusions:
In this report, we demonstrate a simplified approach of BNS RASP that is reproducible with a favorable perioperative complication rates and acceptable postoperative functional outcomes. This technique obviates the need for continuous bladder irrigation and intraperitoneal drain.
Introduction
Benign prostatic hyperplasia (BPH) is the most common cause of lower urinary tract symptoms (LUTS) in elderly men. 1 For patients with medically refractory symptoms, there are variety of surgical approaches including open, laparoscopic, and minimally invasive approaches that may be used in the treatment of BPH. 2,3 The selection of the appropriate surgical approach should be individually tailored based on patient preferences, symptoms severity, prostate volume, the presence of bladder stones, history of previous prostate operation, medical comorbidities, availability of the surgical armamentarium, and surgeon experience. 4 Open simple prostatectomy represents an effective treatment for BPH with demonstrated improvements in mean urinary peak flow, postoperative International Prostate Symptoms Score (IPSS), and a reduction in postvoid residual volume. 5 However, this operation is also associated with significant peri and postoperative complications with an estimated transfusion rate of 7%–14%, transient urinary incontinence in 10% of the patients, and bladder neck contracture and urethral stricture reported in 6% of the patients during 5-year follow-up. 5 –7
In the past decade, there has been increased interest in robot-assisted simple prostatectomy (RASP) as an alternative approach to open simple prostatectomy likely owing to the diffusion of robotic technology and favorable perioperative outcomes. 8 –10 In a recent meta-analysis, minimally invasive approaches including laparoscopic and robotic simple prostatectomy demonstrated significantly less estimated blood loss, reduced transfusion rates, shorter length of stay, and reduced perioperative complication as compared with open simple prostatectomy. 10 Several techniques to perform RASP have been described; however, no head-to-head comparisons have been studied between the approaches. 8,11 The most common complications encountered after RASP were hematuria, urinary tract infection, and acute urine retention. 11 Herein, we describe our technique of bladder neck sparing (BNS)–RASP, which aims to develop a reproducible procedure with a short learning curve, low incidence of short- and long-term complications rate, and offering durably improved functional outcomes.
Methods
All data were prospectively collected into an Institutional Review Board (IRB) approved registry database. Between March 2015 and December 2018, 30 consecutive patients with BPH underwent BNS-RASP by a single high-volume surgeon (D.I.L.). We have no specific exclusion criteria for this operation and have found it appropriate for a wide range of prostate volumes and the presence or absence of a median lobe. Patient age, body mass index (BMI), preoperative prostate-specific antigen (PSA) level, preoperative IPSS, American Society of Anesthesiologists score, prostate size, previous prostate operation, previous prostate biopsy, presence of antegrade ejaculation, and use of clean intermittent catheterization (CIC) were abstracted from the database. Perioperative outcomes including operative time, length of stay, intraoperative blood loss, intraoperative complications, pathological adenoma weight (g), final pathology, need for continuous bladder irrigation, conversion to open technique, 30- and 90-day postoperative complications, patient reported continence, and patient reported antegrade ejaculation after the operation were retrospectively collected. Complication severity was assessed using the Clavien–Dindo scoring system. 12
Statistical analysis
Baseline characteristics, intraoperative and postoperative clinical variables were abstracted from the institutional database. Categorical variables are presented as frequencies and percentages, whereas continuous variables are presented as median with interquartile range (IQR) or mean with standard deviation (SD).
Patient positioning and trocar placement
The procedure was performed using either the da Vinci Xi or Si surgical system (Intuitive Surgical, Sunnyvale, CA). Our standard robotic instrumentation includes monopolar cautery scissors, Maryland bipolar forceps and Prograsp forceps. For positioning, the patient was placed in low lithotomy position and steep 30° Trendelenburg. Intraperitoneal insufflation was achieved through a Veress needle technique. Once pneumoperitoneum was established, the camera trocar was placed cranial to the umbilicus in the midline. The remaining 8 mm robotic trocars were placed, as previously described, under direct vision with a 0° lens across the lower abdomen in addition to a 5 mm assistant port in the left upper quadrant and 12 mm valve-less insufflation trocar system in the left lower quadrant. 1,13
Extravesical prostate exposure
The procedure started with the development of the space of Retzius by incising the peritoneum just lateral to the median umbilical bilaterally. The incision was carried out caudally, ending just lateral and superior to the internal inguinal rings. Once the bladder was dropped, the periprostatic fat was dissected off the endopelvic fascia, puboprostatic ligament, and the prostate gland. The superficial venous complex was controlled and transected. The periprostatic fat pad was rolled back toward the prostate–vesical junction, and then it was excised.
Then, a limited incision in the endopelvic fascia was made on the lateral aspect of the prostate bilaterally. This limited incision was performed to improve visualization of the prostatic capsule to ensure complete dissection of the adenoma to the level of the capsule. (Fig. 1A). Afterward, a 3-0-V-loc suture was used to ligate the runoff of the deep dorsal vein (Fig. 1B) to prevent venous bleeding during the incision of the prostatovesical junction.
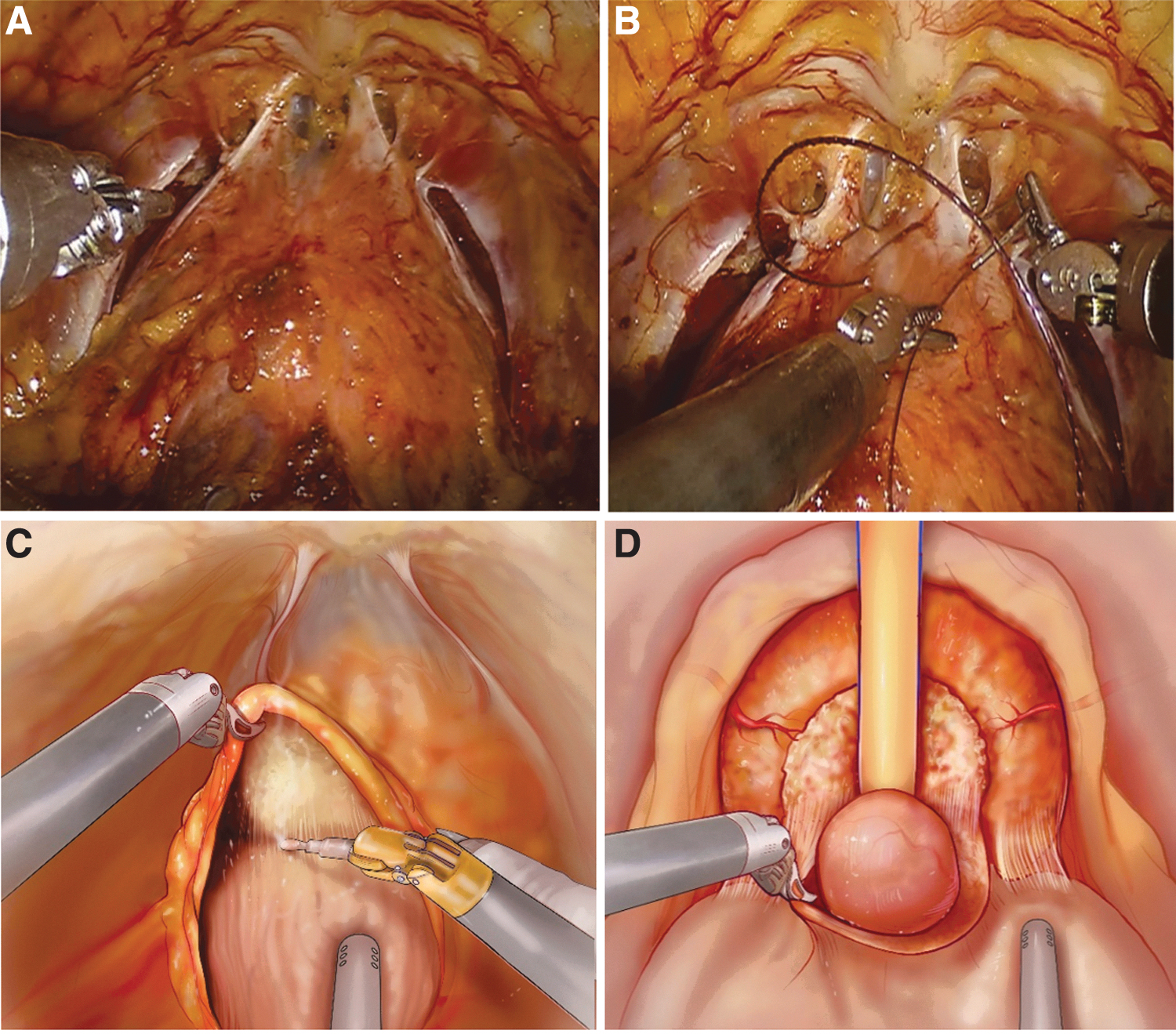
Bladder neck dissection and adenoma enucleation
The lens was switched to a 30° down lens, and the monopolar scissors was exchanged for the permanent spatula cautery. Bladder neck dissection is similar to previously described graded bladder neck preservation for robot-assisted radical prostatectomy (RARP). 14 In brief, the prostate–vesical junction was marked in the midline, then the superficial bladder fat located 2 cm cranial and lateral to the mark was grasped. The plane between the detrusor muscles and the superficial fat was developed using blunt and sharp dissection with pinpoint hemostasis and the dissection continues to reach the lateral borders of the prostatovesical veins. The same dissection was reproduced on the contralateral side (Fig. 1C). Then, the prostatovesical junction was opened, and the Foley catheter was placed on the external tension to aid in retraction. Further dissection of the lateral aspects of bladder attachment to the prostate is essential to ensure that the bladder is dropped away from the prostate. The mucosa and detrusor muscle covering the median lobe was transected, and the bladder was further mobilized away from the prostate using blunt and sharp dissection (Fig. 1D).
The posterior subcapsular plane between the adenoma and the prostate capsule was developed and carried distally toward the apex with pinpoint hemostasis (Fig. 2A). Then, further lateral dissection of the posterior plane was carried out to detach the adenoma from the prostate capsule and allowed to establish a circumferential plane around the adenoma until the anterior commissure of the prostate was exposed (Fig. 2B). The anterior commissure was incised to visualize the verumontanum, which represented the most distal point of dissection (Fig. 2C, D). The adenoma was thoroughly dissected off the verumontanum, cautiously, to preserve the verumontanum that may aid in preserving antegrade ejaculation. 15 The specimen was then retrieved in an EndoCatch™ (Medtronic Plc, Dublin, Ireland) bag.
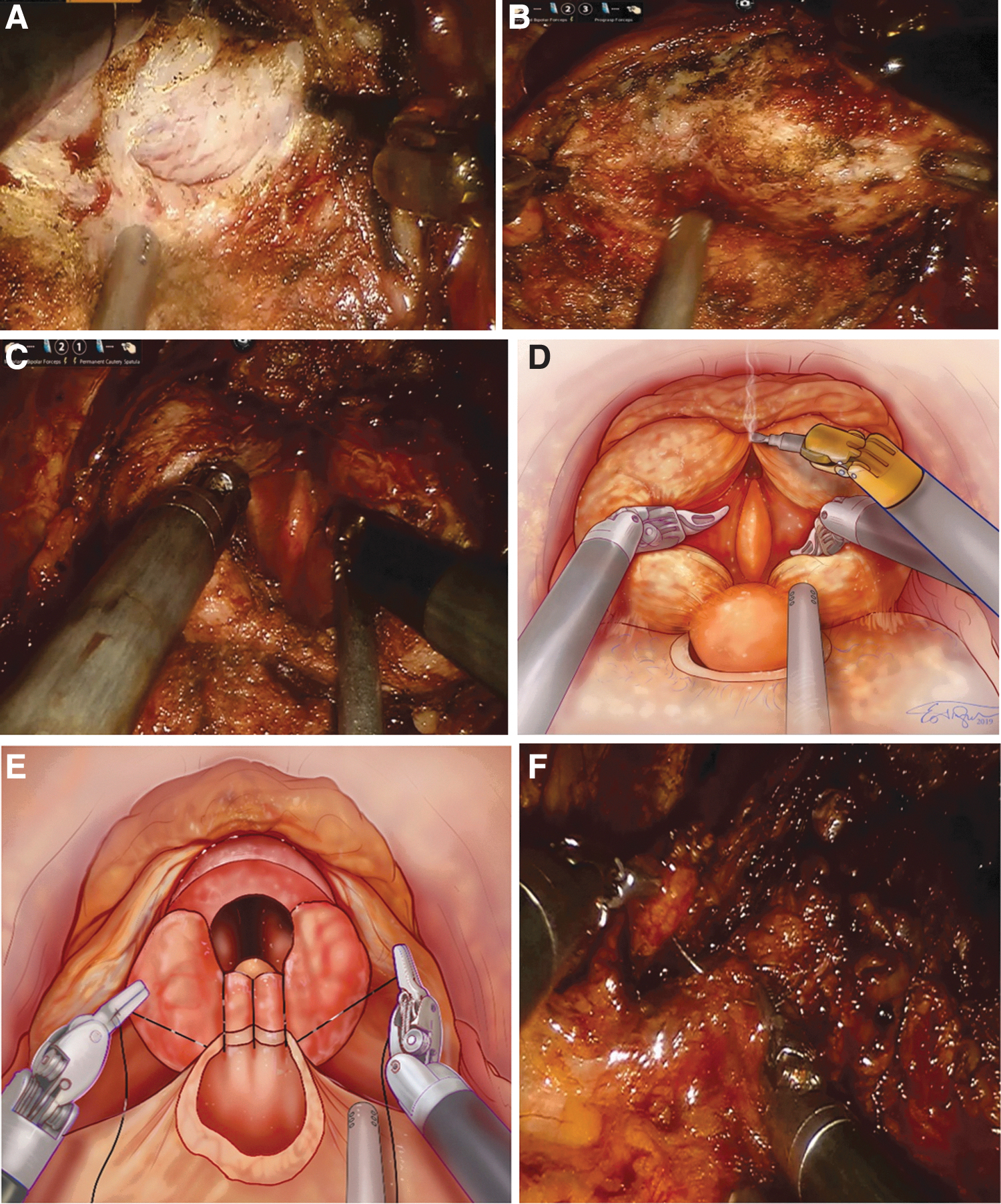
Two-layer reconstruction
A circumferential 360° anastomosis closure as described by Van Velthoven, using a running, double-armed 3-0 bidirectional absorbable barbed Quill™ (Angiotech Pharmaceutics, Vancouver, BC, Canada) suture was performed (Fig. 2E). 16 A new 18F two-way catheter was placed, and the anastomosis was tested to ensure a watertight closure. Finally, the anterior fat overlying the prostate–vesicle junction was reapproximated to the anterior bladder with a running 3-0-V-Loc™ (Medtronic Plc) suture (Fig. 2F).
Finally, a robot-assisted transperitoneal transversus abdominus plane block was performed as previously described. 17 The specimen was retrieved through the camera port, and port sites were closed in the usual manner. We did not place any intraperitoneal drain postoperatively. Patients usually were discharged the same day or postoperative day 1. The patient presented in clinic for Foley catheter removal 1 week after the operation.
Results
Table 1 summarizes baseline characteristics of the cohort. The median age was 66.5 (59.3–72.3) years, and median BMI was 27.6 (24.5–72.3) kg/m2. Most patients had LUTS classified as “severe” before their operation with a median preoperative IPSS of 23 (17.5–27), and a median prostate volume on magnetic resonance imaging of 97 (74–148.75) mL. Eighteen patients had previous prostate biopsies and four patients were performing CIC, two of whom had neurogenic bladder secondary to bladder outlet obstruction.
Demographic and Clinical Characteristics in Men Who Underwent Bladder Sparing Robot-Assisted Simple Prostatectomy
ASA = American Society of Anesthesiology; IPSS = International Prostate Symptoms Score; IQR = interquartile range; PSA = prostate-specific antigen; RASP = robot-assisted simple prostatectomy.
Perioperative outcomes are given in Table 2. The mean (SD) operative time was 107.5 (22.2) minutes, and the mean (SD) estimated blood loss was 132.4 (35.4) mL. All cases were completed robotically without intraoperative complications or conversion to an open technique. Continuous bladder irrigation was not required for any patient postoperatively and all patients were discharged within 24 hours of the procedure. All patients were able to void after catheter removal except one patient with a preexisting diagnosis of neurogenic bladder who resumed CIC. All patients were continent after catheter removal as defined as using 0 pads. Of the 19 patients who had antegrade ejaculation before the operation, 8 patients (42%) reported experiencing antegrade ejaculation after the operation. Two patients developed postoperative urinary tract infection within the 30-day postoperative period and were treated with oral antibiotics (Clavien grade II). Prostate cancer was incidentally discovered in 10% (n = 3) of the patients; all patients had International Society of Urological Pathologists (ISUP) grade group 1 prostate cancer and are currently being managed with an active surveillance protocol. The mean (SD) weight of the enucleated adenoma was 62.6 (39.6) g. No patient required additional surgical or medical treatment during the follow-up, and no bladder neck contractures or urethral strictures occurred. The median follow-up of the cohort was 16.5 (IQR 9.5–24.8) months.
Perioperative Outcomes in Men Who Underwent Bladder Sparing Robot-Assisted Simple Prostatectomy
SD = standard deviation.
Discussion
In this report, we demonstrate a simplified approach to BNS RASP that is reproducible with a short learning curve, favorable perioperative and intermediate functional outcomes. This technique obviates the need for continuous bladder irrigation and an intraperitoneal drain.
Most published transperitoneal techniques used a transvesical approach to the adenoma. 8,18 –20 Although this provides excellent access to the adenoma and allows identification of the ureteral orifices, it offers a limited working space that may prevent effective use of the fourth arm and strait access for the assistant's instruments. Finally, the cystostomy incision and bladder stretching during the operation is not without consequence, as it may potentiate bladder remodeling by inflammation, hypoxia, and mechanical stretching, which may contribute to postoperative urine retention. 21 –23 Therefore, we prefer to use an extravesical approach owing to the similarity with RARP technique that provides a capacious working space and avoids inflicting potential damage to the bladder during the operation.
Our technique is considerably different from other extravesical techniques described thus far. 24,25 First, we completely preserved the puboprostatic ligament and dorsal venous complex (DVC), and selectively ligated the dorsal vein run off at the base of puboprostatic ligaments to decrease intraoperative blood loss and preserve the fibrovascular support to the urethra that has been shown to have improved continence rate in RARP. 26 Second, in our technique, we emphasized the BNS that play a major role in early continence and antegrade ejaculation. 27,28 Finally, the complete circumferential anastomosis decreased postoperative hematuria and obviated the need for continuous bladder irrigation. Therefore, urinary continence was not affected by our technique; as all patients were continent immediately after catheter removal, and 42% of the patients were able to have antegrade ejaculation.
In a recent meta-analysis of 27 observational studies of minimally invasive simple prostatectomy, including 764 patients, the mean operative time was 141 minutes (95% confidence interval [CI] = 124–159), the mean intraoperative blood loss was 284 mL (95% CI = 243–325), and 104 patients (13.6%) developed surgical complication. 11 However, the mean operative time in this series was 107.5 (22.2) minutes, which is shorter than other series and can be explained by the efficiency of using the fourth arm during the procedure and surgeon experience. The mean estimated blood loss was 132.4 (35.4) mL, and minor postoperative complications developed in two patients (6%); these figures demonstrate safety. There were no major complications encountered, and no patient required blood transfusion.
The incidence of identifying occult prostate cancer after transurethral resection of the prostate or simple prostatectomy has sharply declined after the introduction of PSA screening from 23% to 7%. 29 Despite 18 patients (60%) having had at least one prostate biopsy before the procedure, prostate cancer was discovered in 10% of the patients; all of them had ISUP grade group 1, and have been managed with an active surveillance protocol without requiring active treatment or additional intervention. This finding underlines the poor prostate cancer detection rates using systematic prostate biopsies in prostates >40 cm3. 30
This study was intended to focus on our surgical technique for RASP and to report our early outcomes. A formal comparative assessment with other available techniques and analysis of predictive factors of the surgical outcomes was not performed and can be regarded as a limitation of this study.
Conclusions
BNS-RASP represents a reproducible surgical approach for the treatment of BPH with favorable perioperative complication rates and acceptable postoperative functional outcomes. Standardization of each surgical step has allowed for optimization of the procedure and, ultimately, an improvement of its outcomes. Additional multicenter studies are necessary to validate these initial findings.
Research Involving Human Participants and/or Animals
The study was approved by IRB under PRIME protocol.
Informed Consent
Waved.
Footnotes
Authors' Contributions
M.S.: Project development and concept, article writing. K.P.: Data collection. S.N.: Data collection. J.K.: Project development. A.E.-F.: Data collection. R.W.D.: Manuscript editing. D.I.L.: Project development and concept, article proofreading.
Acknowledgment
The authors thank Eu Trueblood for assistance with the surgical illustrations.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.