
Abstract
Purpose:
To evaluate the onlay technique using the appendix for ureteral reconstruction and describe the initial experience of nine operations performed by one surgeon.
Methods:
Nine patients with complex ureteral strictures who underwent appendiceal onlay flap ureteroplasty since May 2019 were recruited from our RECUTTER database. There were seven men and two women, with a mean age of 38.9 years; four patients underwent robot-assisted laparoscopic surgery, and five patients underwent traditional laparoscopic surgery. All patients had iatrogenic injuries of the ureter after treatment of stone disease. Seven patients had proximal ureteral strictures, and two had midureteral strictures. The mean stricture length of the nine patients was 3.9 (range 3–4.5) cm. Nephrostomy was performed in seven patients before they presented to our center, and the other two patients had indwelling Double-J ureteral stents.
Results:
All nine operations were effectively completed without open conversion. The mean operation time was 182 (range 135–220) minutes, the mean estimated blood loss was 71 (range 20–100) mL, and the mean length of postoperative hospital stay was 9 (range 6–12) days. No postoperative complications of high grade (Clavien–Dindo III and IV) occurred within 30 days of surgery. All the patients had their Double-J ureteral stents and nephrostomy tubes removed after complete ureteroscopy and upper urinary tract urodynamic examination or CTU, which showed that the anastomosis healed well and that the urinary tract was unobstructed, respectively. The objective success rate was 100% (all the patients had endoscopic and radiographic resolution of their ureteral strictures). The subjective success rate was 88.9% (one patient developed recurrent back discomfort and a 0.5 cm calculus was found in her renal pelvis).
Conclusions:
Appendiceal onlay flap ureteroplasty is a viable and effective technique for treating complex proximal and middle ureteral strictures at the right side.
Introduction
Ureteral strictures can result from congenital anomalies, iatrogenic injury, trauma, and radiation therapy. 1 The endoscopic management options include endoureterotomy and balloon dilatation, which are most suitable for cases with narrow segments measuring <1 cm. 2 For long or complex ureteral strictures, surgical repair is an option. Surgeons select the surgical approach based on the location of the ureteral stricture (upper, middle, or lower ureter) and its length.
Distal ureteral strictures, even when extensive, may be treated by ureteral reimplantation with a bladder psoas hitch or Boari flap to obtain extra length. 3 Besides, transureteroureterostomy was most commonly used to treat an injured or obstructed ureter that makes ureteral reimplantation with or without a psoas hitch and bladder flap impractical. 4 For strictures of the ureteropelvic junction (UPJ), the ureter can be reconnected with the renal pelvis using any type of pyeloplasty. 5 However, proximal and middle ureteral strictures remain a challenge, and ureteral substitution becomes necessary when end-to-end anastomosis becomes difficult.
The alternative substitution tissues for ureter reconstruction include an ileum, buccal, or lingual mucosal graft and the appendix. 6 In 1912, the first ureteral substitute with the appendix was reported by Agrawal et al. 7 Since then, some surgeons have reported cases of this technique, appendix interposition, mainly for pediatric patients, 8 –23 and the longest stricture segment of the ureter was reported to be 8 cm. 23 The first case to be published on the reconstruction of the left ureter with the appendix interposition was described by Die Goyanes et al. in 1983. 10 For cases with appropriate appendix conditions, left ureteral stricture is not a contraindication for repair using the appendix interposition. In addition, appendix interposition for left or right ureteral reconstruction in pediatric renal transplantation patients has been reported in several studies. 24,25
The appendix interposition technique may be a solution to manage ureteral stricture in certain cases, but fistula and anastomosis stenosis are the common complications that have been reported. 20 The onlay concept was first used to treat urethral stricture disease in 1996. 26 In 2009, Reggio and coworkers reported the first case of laparoscopic appendiceal onlay ureteroplasty to repair ureteral strictures. 27 Afterward, a study with six patients with laparoscopic appendiceal onlay ureteroplasty was published in 2015. 28 Onlay flap repair ureteral stricture has been considered more advantageous than interposition. This technique can maintain the blood supply of the ureteral posterior wall and expand the lumen of the ureter. Laparoscopic appendiceal onlay ureteroplasty has not been used widely, while no case of robot-assisted laparoscopic appendiceal onlay ureteroplasty has been reported.
In this study, we evaluated the onlay technique using the appendix for ureteral reconstruction and described our initial experience with robot-assisted laparoscopic appendiceal onlay ureteroplasty.
Patients and Methods
Patient selection
This was a prospective study approved by the Ethics Committee of Peking University First Hospital. Patients who had appendiceal onlay ureteroplasty were recruited from our RECUTTER database (
Since May 2019, nine patients underwent right ureteral stricture repair with an appendiceal onlay flap by one surgeon, including four robot-assisted laparoscopic operations and five traditional laparoscopic operations. All patients were most eligible for appendiceal onlay flap ureteroplasty based on the location and length of ureteral stenosis and their appendix conditions. These patients were prospectively followed with regular clinical and radiographic examinations. Outcome evaluations included patients' postoperative complaints, ultrasonography scans, ureteroscopy examinations, upper urinary tract image urodynamic tests, or computed tomography urography (CTU).
The demographic and preoperative characteristics are presented in Table 1. The patients' ages ranged from 28 to 49 years, and the mean age was 38.9 years. There were seven men and two women, and the mean body mass index was 23.6 (range 18.2–26.7) kg/m2. Seven patients had proximal ureteral strictures, and two had midureteral strictures. The mean stricture length was 3.9 (range 3–4.5) cm, which was measured during the operations. All patients had iatrogenic injuries of the ureter after treatment of stone disease, seven strictures were caused by holmium laser lithotripsy, and two were the result of ureterolithotomy. Six patients had undergone previous therapy (balloon dilatation, n = 4; ureteroureterostomy, n = 2; and endoureterotomy, n = 2). The mean time from initial ureteral injury to appendiceal onlay ureteroplasty in our center was 2.2 years (range 1–5 years). Nephrostomy was performed in seven patients before they presented to our center, and the other two patients had indwelling Double-J ureteral stents.
Demographic and Preoperative Characteristics
Surgical techniques
The patients were placed in a low-flank position with the right side elevated by 70°. First, a Veress needle was inserted 2 cm inferior to the costal margin of the right midclavicular line (point A). Once pneumoperitoneum was established, a 12-mm camera port was placed at the lateral border of the right rectus muscle (point B), a robotic camera positioned at 30° was then passed into the abdomen through this site. Subsequently, a thorough examination of the abdominal cavity was performed. Under direct vision, three mainly operative trocars (all 8 mm) were inserted to point A, 10 cm inferior of the right anterior axillary line (point C) and 10 cm inferior to point B at the lateral border of the right rectus muscle (point D). Two auxiliary trocars (12 and 5 mm, respectively) for assistance were placed at point E (equal distance from point A and point B and both >5 cm) and point F (equal distance from point B and point D and both >5 cm) (Fig. 1). 29 The robot was then docked at a 90° angle to the patient.
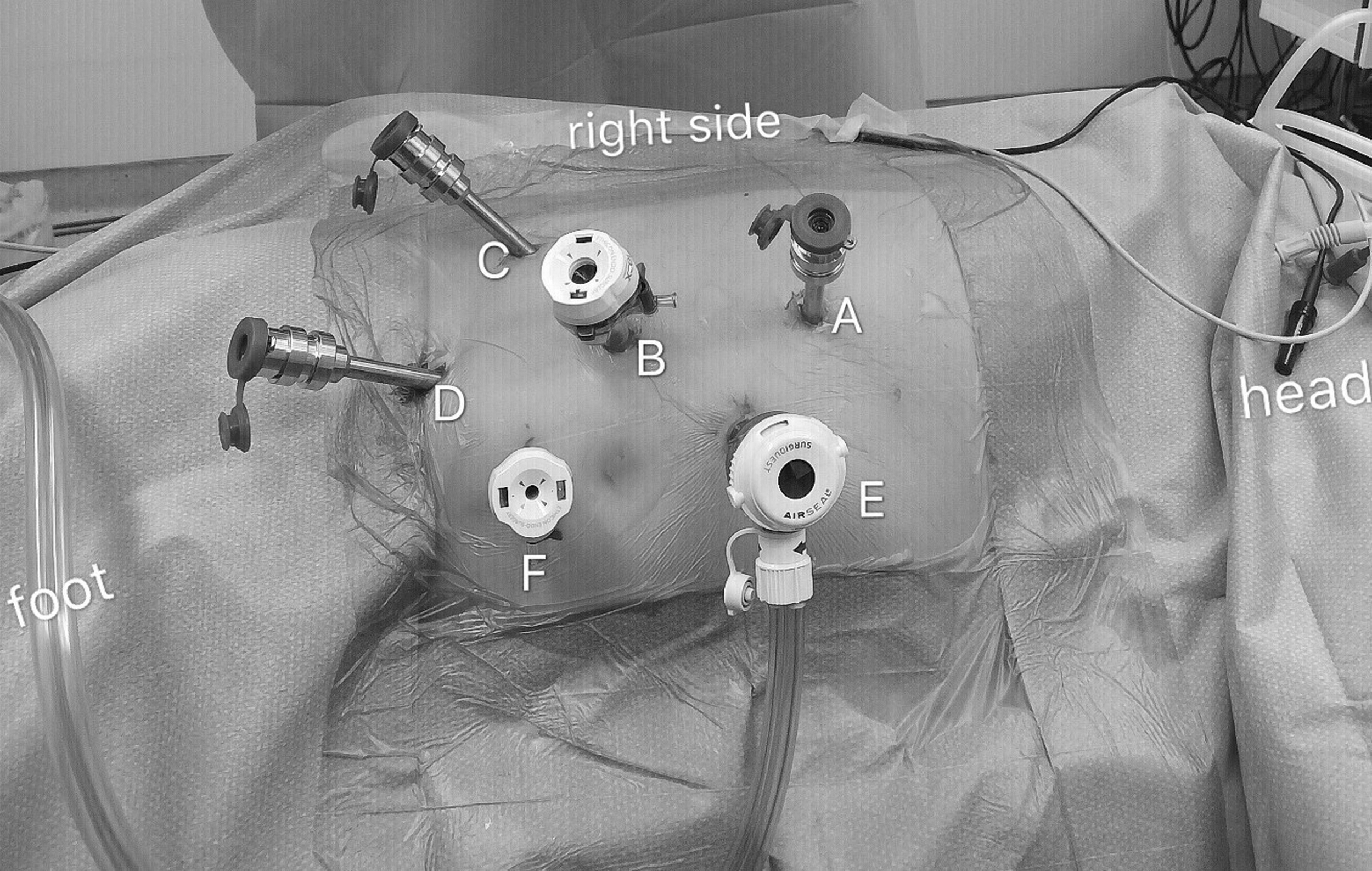
Patient position and port placement for robot-assisted laparoscopic appendiceal onlay flap ureteroplasty. The patients were placed in a low-flank position with the right side elevated by 70°. A Veress needle was inserted 2 cm inferior to the costal margin of the right midclavicular line (point A). Once pneumoperitoneum was established, a 12-mm camera port was placed at the lateral border of the right rectus muscle (point B), a robotic camera positioned at 30° was then passed into the abdomen through this site. Under direct vision, three mainly operative trocars (all 8 mm) were inserted to point A, 10 cm inferior of the right anterior axillary line (point C) and 10 cm inferior to point B at the lateral border of the right rectus muscle (point D). Two auxiliary trocars (12 and 5 mm, respectively) for assistance were placed at point E (equal distance from point A and point B and both >5 cm) and point F (equal distance from point B and point D and both >5 cm).
After the retroperitoneum was entered, an incision was created along the white line of Toldt, and the right colon was mobilized and turned medially. Then, the renal pelvis and ureter were identified and revealed by sharp and blunt dissection at the level of the lower pole of the kidney. The ureteral stricture is usually adherent to the surrounding tissues and difficult to identify. The surgeon determined the ureteral stricture via several methods. First, the length was estimated according to preoperative urography (Fig. 2). Second, for patients with nephrostomy, we injected 20 mL physiologic saline from the tube, and the ureter located above the narrow segment was dilated. Third, we injected indocyanine green intravenously, and normal ureteral perfusion was observed using near-infrared fluorescence imaging to confirm the range of stenosis segment (Fig. 3).
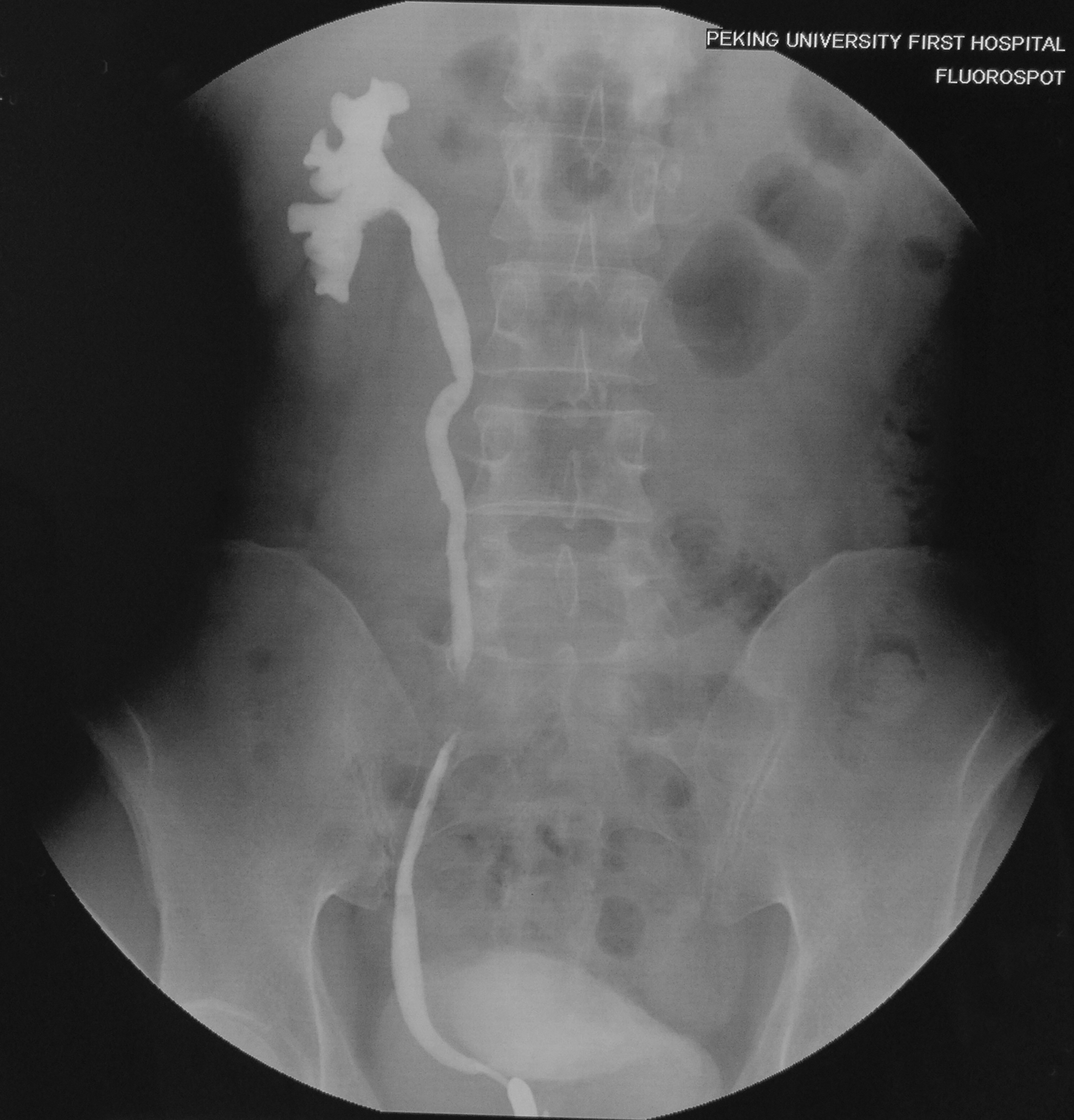
Estimating the stricture location, length, and severity of ureters according to the preoperative antegrade nephrostography and retrograde ureterography.

Estimating the normal ureter ends and the stricture length under near-infrared fluorescence after intravenous injection of indocyanine green during robot-assisted laparoscopic surgery.
Then, the diseased ureter was longitudinally incised and a ureteral catheter with scale was used as a reference to accurately measure the length of the stenosis segment (Fig. 4), guiding the incision of the appendiceal flap of the same length. We transected the appendix from the cecum at its base, but preserved the mesoappendix if its length and conditions were suitable. Then, the distal end of the appendix was transected, and the appendix was detubularized along the antimesenteric border (Fig. 5). In three cases, the region of ureteral stenosis was incised longitudinally along the ventral side and measured accurately, and the appendiceal onlay flap was placed to enlarge the ureteral lumen.
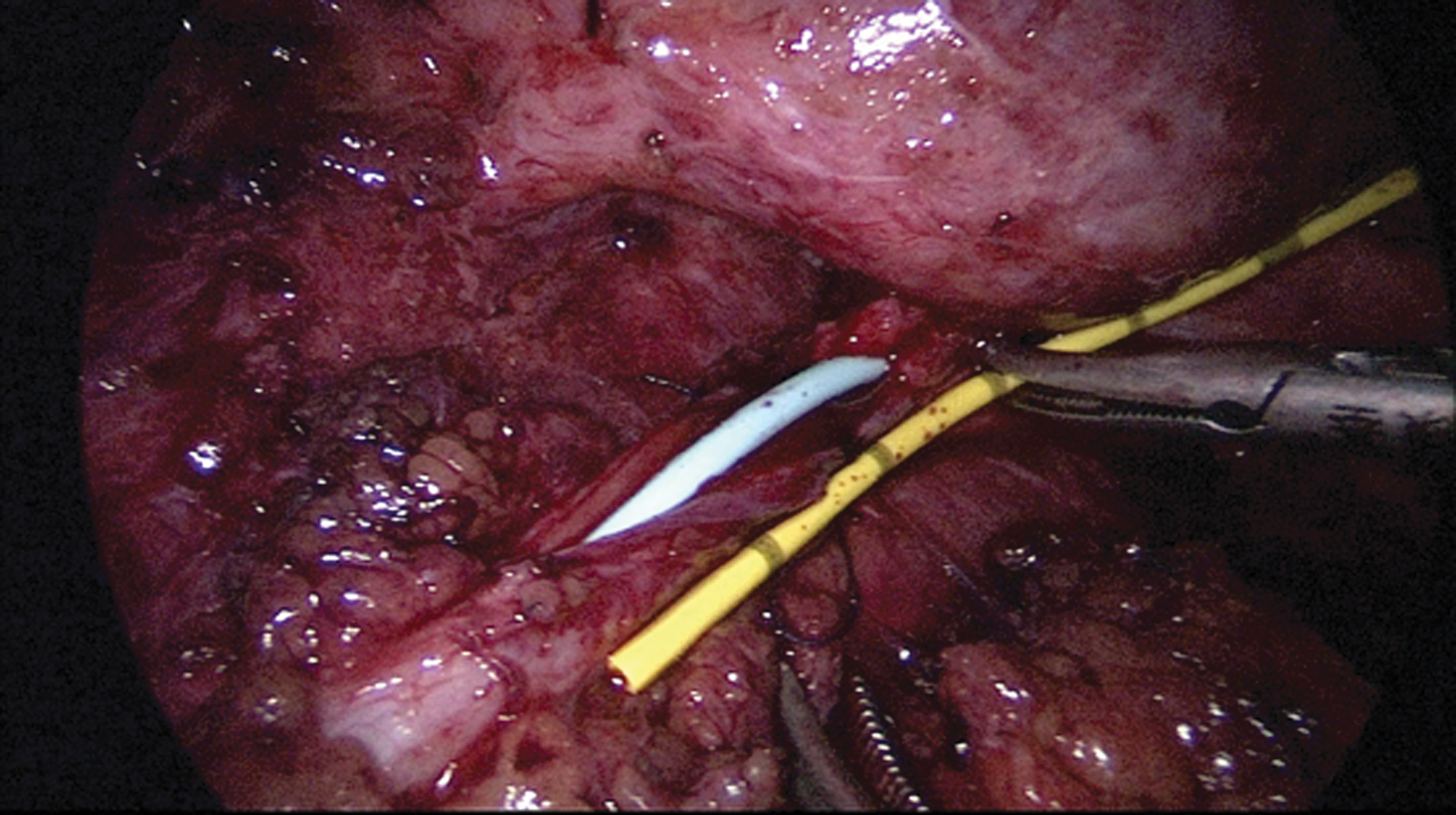
Measuring the length of strictured ureter using a ureteral catheter with scale.

Procedures of detubularizing the appendix along the antimesenteric border.
In six cases, the ureteral lumen was completely obliterated. We excised the obliterated segment and then anastomosed the normal ureteral tissue from the posterior wall, to create a new ureteral plate for the anastomosis of appendiceal onlay flap in the anterior aspect (Fig. 6). It is important to sew a stitch along one side of the ureter before completely removing the obliterated segments.

Intraoperative image of posterior wall reconstruction via running suture between two healthy ureteral ends.
The proximal end (opposite the cecal end) of the appendix was anastomosed to the proximal ureter, and the distal end (cecal end) of the appendix was anastomosed to the distal ureter. A 6F Double-J ureteral stent was placed through the ureteral defect before anastomosis of the ureteral defect and appendix onlay. The edges were anastomosed in a running manner using 5-0 Vicryl sutures (Fig. 7). Finally, a drain was placed adjacent to the anastomosis once omental coverage was completed. The traditional laparoscopic procedure steps that we used have been described previously. 27,28
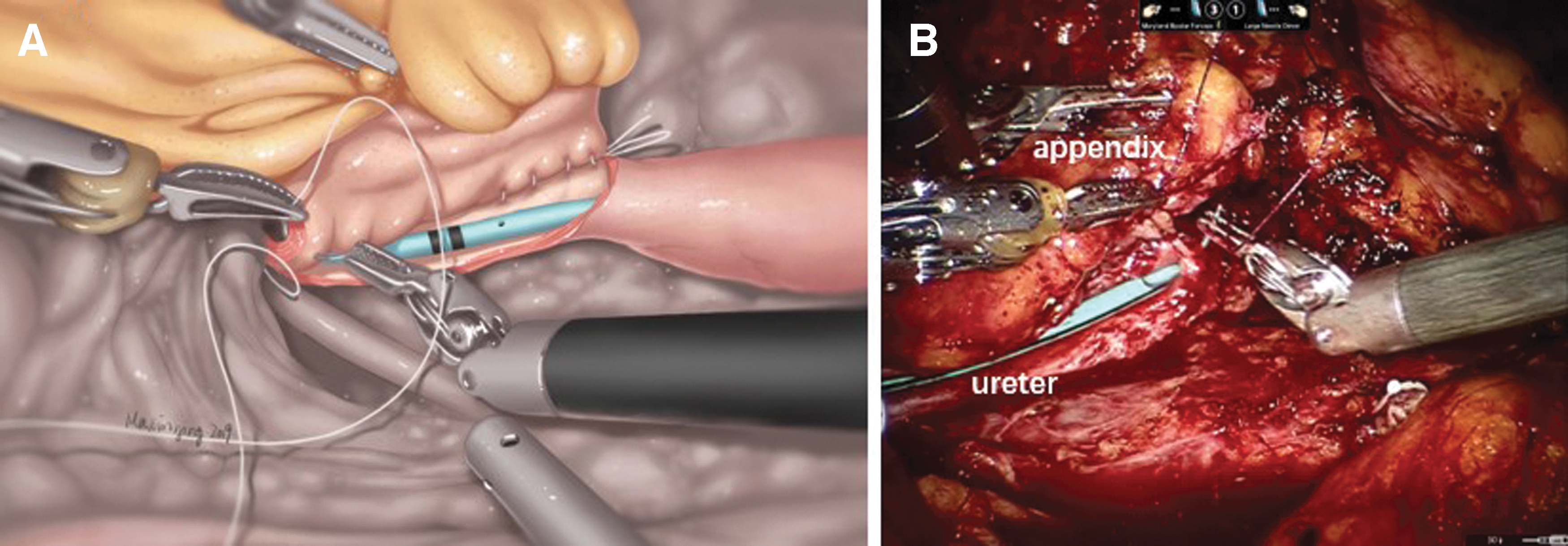
Procedures of the anastomosis between the partially excised ureteral segment (ureteral plate) and appendiceal onlay.
Postoperative management and follow-up
After the operation, patients received an indwelling Foley catheter, a drain near the anastomosis and a Double-J ureteral stent. The catheters remained in the seven patients who underwent ipsilateral nephrostomy preoperatively. The Foley catheters were usually removed for 1 week. The drain was usually removed when the output was <50 mL 4–6 days after the operation. Creatinine in the drain fluid was evaluated if the drain volume was high. Kidney, ureter, and bladder radiograph was performed routinely before discharge to confirm that the Double-J ureteral stent stayed in the appropriate position. Patients with a Double-J ureteral stent and ipsilateral nephrostomy were discharged. Two weeks after surgery, the nephrostomy tube was clamped but not removed. The patients were asked to return to the hospital for a ureteroscopic examination 2 months after surgery if there was no discomfort, such as fever or low back pain, during this period.
The Double-J stent was removed or replaced according to the healing state of the anastomosis. Patients with preoperative percutaneous nephrostomy are followed with imaging urodynamic examination (IUE) 3–4 months after surgery. The upper urinary tract IUE was performed according to the Whitaker test. 30 In the prone position, a 7F three-lumen catheter was placed into the renal pelvis from the nephrostomy tube. Iopromide was injected into the renal pelvis at 10 mL/min for upper urography and pressure measurements. Other patients are followed by CTU. Since no ureteral narrowing or contrast extravasation was confirmed, the nephrostomy could be removed. Finally, the patients were instructed to undergo an ultrasound examination annually. If the patients felt discomfort such as back pain or fever, they were instructed to visit the hospital at any time. Subjective and objective success was defined as relief of symptoms and improvement in the imaging results (ultrasonography, CTU, or IUE) during the follow-up period, respectively.
Results
All nine operations were effectively completed without open conversion. Perioperative and postoperative data on the four robot-assisted laparoscopic operations and five traditional laparoscopic operations are shown in Table 2. In three cases, the diseased ureter was incised to open the narrowed segment, and an appendiceal onlay was placed to expand the lumen. In six cases, ureteral stenosis was transected, two ends of the healthy ureter underwent posterior wall anastomosis, and an appendiceal onlay was placed to cover the anterior defect. The effect of the posterior wall reconstruction technique on patient recovery needs to be observed further. The mean (range) operation time was 182 (135–220) minutes, and the mean (range) estimated blood loss was 71 (20–100) mL.
Intraoperative and Postoperative Parameters
No patient needed blood transfusion. No intraoperative complications occurred, and no postoperative complications of high grade (Clavien–Dindo III and IV) occurred within 30 days of surgery. Only two patients developed fever, and they both responded well to antibiotics. The mean (range) indwelling drain time was 4.2 (2–6) days, and the mean (range) length of postoperative hospital stay was 9.1 (6–12) days. There was no significant difference in the above parameters between the robot-assisted laparoscopic surgery and traditional laparoscopic surgery.
Thus far, the median follow-up duration was 6.8 months (range 4–10 months). None of the patients reported noticeable discomfort during follow-up. All the patients completed ureteroscopy and had their Double-J ureteral stents removed 2–3 months after surgery. The nephrostomy tubes of two patients were accidentally dislodged within 4 months of follow-up. Therefore, five and four patients were followed with upper urinary tract IUE and CTU, respectively, 4 months after surgery. The ureteroscopic and radiologic results showed well-healed anastomosis and the patent upper urinary tract was unobstructed (Fig. 8). The objective success rate was 100% (all the patients had endoscopic and radiographic resolution of their ureteral strictures). The subjective success rate was 88.9% (one patient developed recurrent back discomfort and a 0.5 cm calculus was found in her renal pelvis).

Discussion
Surgical repair is an option for complex ureteral strictures that are not eligible for endoureterotomy or balloon dilatation. For distal ureteral strictures, even when extensive, may be treated by ureteral reimplantation, and additional length can be obtained with a psoas hitch or Boari flap, as required. 3 For UPJ obstruction, the ureter can be reconnected with the renal pelvis using any type of pyeloplasty. 5 However, for long proximal and middle ureteral strictures, the treatment options include downward nephropexy, renal autotransplantation, nephrectomy, and ureteral substitution, which are rarely required for complex ureteral strictures and should be used only when the previously discussed repairs are not possible or are contraindicated. 31
The alternative tissues that can be used for ureter reconstruction include ileum, buccal, or lingual mucosal grafts and the appendix. 7 Surgeons select the surgical approach based on the length of the ureteral stricture. To date, the longest ureteral stenosis repaired with an appendix onlay laparoscopically is 6 cm, as reported by Duty and associates. 28 We think an appendiceal onlay flap can be used to repair 2–6 cm proximal and middle ureteral stenoses, the mean stricture length of this study was 3.9 (range 3–4.5) cm. Laparoscopic appendiceal onlay ureteroplasty has not been used widely, and all reported procedures have not been performed with robotic platforms (as shown in Table 3).
Review of the Literatures Regarding Ureteroplasty with the Use of Appendiceal Onlay Flap
Objective success was defined as improvement in the imaging results during the follow-up period.
Subjective success was defined as relief of symptoms during the follow-up period.
N.D. = not determined.
The present study describes nine patients who underwent right ureteral stricture repair with an appendiceal onlay flap performed by one surgeon, including four robot-assisted laparoscopic operations and five traditional laparoscopic operations. To the best of our knowledge, we report the first case of a robot-assisted laparoscopic approach for appendiceal onlay ureteroplasty. It would be premature to identify the differences between robot-assisted laparoscopic surgery and traditional laparoscopic surgery groups according to the intraoperative and postoperative parameters of our nine patients (Table 2). However, robotic platforms are advantageous for delicate operations, such as suturing, while traditional laparoscopic surgery is advantageous for rapid dissection and the exposure of lesions.
Ileal ureter replacement is the ultimate method for the reconstruction of long ureteral defects or bilateral ureteral substitution. 31 There are several potential advantages to using the appendiceal onlay rather than the ileum for ureteral stricture repair. The appendiceal onlay flap ureteroplasty can minimize the trauma associated with resecting an ileum segment compared with the ileal ureter replacement. The function of absorption and secretion of the mucosa in the appendix is lower than those in the ileum, which greatly reduces the risk of systemic acidosis and mucus stasis after surgery; therefore, it is a suitable reconstruction method for patients with renal insufficiency. Of course, the length of the appendix in the human body is limited, and the extent to which ureteral stenosis can be repaired is limited, but the risk of failure of this technique should not prevent patients from undergoing ileal interposition or autotransplantation.
There are many cases reported in the literature that use oral mucosal grafts, especially buccal mucosal grafts, to repair ureteral strictures. Zhao and colleagues reported that an 8 cm ureteral defect was repaired with a buccal mucosal graft. 32 The surgeon in our center has performed 15 ureteral stricture repair procedures with lingual mucosal grafts, and all patients are currently undergoing detailed follow-ups. However, fewer cases of ureteral stricture repair using the appendiceal onlay have been reported, and so, there are insufficient data for a comparative analysis of these two techniques. At present, the lengths of the narrow segments that can be repaired by the techniques are equivalent. Because of its anatomical position, the appendix is mostly used to repair the right ureteral stricture, and the oral mucosa can be used on both sides. The appendix, mesoappendix, is preserved, and its blood supply is better than that of the oral mucosa. The authors suggest that more studies comparing these two techniques be conducted.
To measure the length of ureteral stenosis during the operation, Zhao and coworkers used ureteroscopy in robot-assisted ureteral reconstructions using buccal mucosal grafts and observed the quality of the anastomosis after completion. 32 Based on our intraoperative experience, it is not difficult to determine the length of ureteral stenosis using the three methods described above. The authors think that ureteroscopy is not necessary. According to the severity of ureteral stenosis, the narrowed segment can be incised longitudinally along the ventral side or transected for posterior wall reconstruction. To the best of knowledge, the present study is the first report of ureteral stricture repair using ureteral posterior wall reconstruction combined with the appendiceal onlay technique. The effect of posterior wall reconstruction methods on patient recovery needs to be assessed further.
Appendiceal onlay ureteroplasty provides a solution for urologists to repair complex ureteral strictures. For 2–6 cm ureteral stenoses that are not eligible for direct anastomosis, especially in the proximal and middle ureters, an appendiceal onlay can be used as an alternative to the ileal ureter. Of course, no cases of left ureteral stenosis repair using the appendiceal onlay have been reported, and this procedure deserves continued exploration.
Although the data on the patients were collected prospectively, our study was limited by the small sample size and short follow-up period. We will continue to follow up on these nine patients carefully and collect longer term recovery data. At the same time, more cases will be accumulated. We will summarize our more comprehensive experience on robot-assisted laparoscopic and ureteral posterior wall reconstruction techniques in the future.
Conclusions
Appendiceal onlay flap ureteroplasty is a feasible and effective technique for treating complex proximal and middle ureteral strictures at the right side.
Footnotes
Acknowledgment
We acknowledge the excellent work of the medical illustrator, Madam Xinying Ma, who drew figures for us.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Video S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.