
Abstract
Introduction:
A detailed understanding of renal tumor anatomy is required to perform partial nephrectomy. We evaluated the utility of a CT-based interactive virtual reality (iVR) display to assist surgeons' understanding of the precise location of the renal tumor.
Methods:
CT scans and iVR models of 11 patients with a mean R.E.N.A.L. nephrometry score of 6.9 were evaluated. Seven faculty urologists and six urology residents reviewed CT scans and positioned each tumor onto a digital three-dimensional model of the same kidney, although without the tumor present. A week later, participants repeated the session using both iVR models and CT scans. For both time points, the overlap between the surgeon-inserted tumor and the actual tumor location was calculated. Participants answered a 1 to 10 Likert scale survey to gauge their understanding of renal and tumor anatomy based on CT alone vs CT+iVR.
Results:
Median tumor overlap for the entire cohort was 28% after CT review and 42% after CT+iVR (p = 0.05); among faculty urologists, for CT+iVR vs CT alone, percentage overlap improved (47% vs 33%, p = 0.033) and the incidence of 0% overlap decreased (19%–4%, p = 0.024), respectively. Among residents, there was no significant difference for either percentage overlap or 0% overlap for CT vs CT+iVR. The percentage overlap for the two tumors with high R.E.N.A.L. nephrometry scores (i.e., 10) increased from 51% to 67% after using CT+iVR (p = 0.039). The combination of CT+iVR was an independent predictor of improved overlap vs CT alone (odds ratio 2.22, 95% confidence interval 1.04–4.78, p = 0.039). Faculty surgeons' survey responses showed an improved understanding of the tumor location and shape with the addition of iVR (p < 0.05).
Conclusions:
The addition of patient-specific iVR models to standard CT imaging improved the ability of faculty urologists to accurately configure the location of a renal tumor, and improved their understanding of tumor anatomy.
Introduction
The treatment of localized renal-cell carcinoma (RCC) is primarily surgical. When amenable, nephron sparing surgery is largely preferred given concerns of cardiovascular events and overall mortality because of decreased renal function. 1,2 Although the use of partial nephrectomy (PN) for the treatment of localized RCC has been expanded, there has been a concomitant shift in the surgical approach from open surgery to laparoscopic and robot-assisted PN. 3,4 As the minimally invasive approach lacks direct visual evaluation and contact with tissues, surgical decisions typically rely on preoperative imaging studies. Surgical planning for PN is based on cross-sectional CT and MRI. Although these imaging modalities can accurately identify renal anatomy, including vasculature, collecting system, and tumor characteristics, a major limitation is their two-dimensional (2D) nature. Accordingly, the surgeon is required to review hundreds of axial, coronal, and sagittal images to obtain a mental three-dimensional (3D) representation of the tumor.
Meticulous preoperative planning with cognitive 3D mental interpretation of the tumor and its spatial relationship with the surrounding anatomy is key before performing PN. The acquisition of a visuospatial ability necessary to convert 2D images to mental 3D images is often challenging, and indeed in a recent study, experienced surgeons failed to accurately perceive the 3D arrangement of the tumor relative to its surrounding anatomy from standard 2D cross-sectional imaging modalities alone. 5 In efforts to bridge these challenges, advanced medical imaging technologies such as virtual reality and 3D printing are being studied with regard to their potential impact on surgical planning as well as surgical education.
3D printing has been employed to provide a more tactile realistic 3D representation of the pertinent anatomy, to improve operative training and patient education. 6 –8 Wake and colleagues 5 recently investigated the utility of 3D-printed kidney models in improving the surgeon's ability to localize the tumor. They found that the use of 3D-printed models enhanced tumor localization; however, the 3D-printed models are expensive and not readily available given the time needed to produce them. 5 Also, the 3D-printed model precludes an immersive experience and is devoid of any of the surrounding anatomy.
In view of the shortcomings of 3D printing, we have explored the use of patient-specific immersive interactive virtual reality (iVR) models for preoperative planning and surgical education. With a virtual input device attached to the head-mounted display, the surgeon not only visualizes the relevant anatomy, but can also interact with, and manipulate the patient's organs and anatomic components of the kidney (pull the tumor from the kidney to inspect the tumor bed, remove the parenchyma from the collecting system, etc.). The utilization of virtual reality technology has been associated with improved clinical outcomes and better understanding of renal surgical anatomy. 9,10 As these models can be rapidly produced from CT scans using open source software, iVR may be a promising tool for preoperative planning and surgical education in minimally invasive renal surgery.
Herein we report our evaluation of the impact of iVR technology as an adjunctive tool to CT in aiding a surgeon's ability to accurately localize renal tumors.
Materials and Methods
CT acquisition
IRB approval is included, 11 patients with renal tumors who had PN and had preoperative iVR models were included in our study. All patients had available CT scans with precontrast and postcontrast phases. Six patients had right-sided tumors and five had left-sided tumors. The mean tumor diameter was 3.6 cm and the mean tumor volume was 35.6 cm3. The mean R.E.N.A.L. nephrometry score was 6.9 (4–10) with a mean endophytic component of 32%.
iVR and 3D model creation
Contrast-enhanced CT images in Digital Imaging and Communications in Medicine (DICOM) format were manually segmented using 3D Slicer (National Institute of Health, Bethesda, MA); slice-by-slice delineation of specific anatomic structures (renal parenchyma, tumor, vasculature, and collecting system) was performed to construct a 3D model. The 3D models were then uploaded into an iVR model cloud website, Bosc (Pyrus Medical, Seattle, WA). Oculus Rift and Touch controllers (Facebook, Inc., Menlo Park, CA) for head-mounted display, paired with Leap Motion (Leap Motion, Inc., San Francisco, CA), were utilized for iVR model display and manipulation.
Tumor placement
Thirteen physicians were recruited from our institution: seven fellowship-trained urology attendings experienced in PN and six urology residents with a mean of 3 years of training. The participants viewed the CT scans on RadiAnt DICOM Viewer (Medixant, Poznan, Poland) and the corresponding radiology reports. All phases of the CT scan including axial, coronal, and sagittal views were provided. The 3D kidney models were viewed in computer-aided design (CAD) software (3-matic; Materialise, Leuven, Belgium) for participants to mark their perceived location of the tumor. Using 3-matic, the tumor was duplicated and moved to a random location off of the renal surface, whereas the tumor in its original location was “erased.”
Each participant was then asked to move the duplicated tumor in the X (medial/lateral), Y (anterior/posterior), and Z (superior/inferior) planes and to place the virtual tumor on the “erased” renal model (Fig. 1). This process was repeated for a 30-minute period, allowing each participant to complete as many CT viewing and tumor placement exercises as possible during the 0.5-hour period. A total of 11 cases were prepared for review by the participants. At the end of each exercise, participants were administered a Likert-style questionnaire to assess their understanding of tumor, hilar, and vascular anatomy using CT alone (0 = not at all to 10 = very well).

After a washout period of at least 1 week, the participants completed an additional session using iVR in conjunction with CT imaging they had previously viewed, and were asked to again place the virtual tumor on the “erased” kidney using the 3-matic system. The same Likert-style questionnaire was administered to assess the participants' understanding of the anatomy, now with the aid of iVR plus CT viewing. During both sessions, time spent reviewing each imaging modality and time spent placing the tumor were recorded. Each virtual tumor placed on the “erased” kidney was analyzed to measure the degree of overlap between the placed tumor and the true tumor location. Deviations from the coordinates of the actual tumor location were recorded in each dimension. Percentage overlap was calculated by the following equation:
Statistical analysis
Time spent reviewing scans and placing the “virtual” tumor on the “erased” kidney, degree of overlap, number of zero overlaps, and magnitude and direction of error in the X, Y, and Z planes were compared between sessions. Paired continuous nonparametric variables were analyzed using Wilcoxon signed rank test and Welch's t-test. Categorical variables were compared using a chi-squared test. Unpaired continuous variables were analyzed using Kruskal–Wallis analysis of variance and Dunn's test with Bonferroni correction if greater than two groups, otherwise Wilcoxon rank sum test was used. Questionnaire data provided by the participants were compared between sessions using Wilcoxon signed rank test.
Multiple logistic regression was applied to determine the independent relationship between imaging modality (CT or CT with iVR) and percentage overlap while controlling for significant covariates. Since the percentage overlap values were not normally distributed, they were converted to a binary variable above or below the median percentage overlap (38%). For all statistical tests, a p-value <0.05 was deemed statistically significant. Statistical analysis was performed using RStudio® version 1.1.456 (RStudio, Boston, MA).
Results
Comparison of CT and CT+iVR sessions
Participants reviewed a cumulative total of 85 CT scans and their corresponding iVR models; the mean number of CT scans and iVR models viewed was 6.5 (range 4–11). Faculty and residents reviewed 47 (mean 6.7) and 38 (mean 6.3) pairs of CT scans and iVR models, respectively (p = 0.75). Compared with CT alone, the combination of CT and iVR was associated with 32% reduction in the time spent placing the tumor on the 3D CAD kidney model among faculty and 34% reduction among residents (1.14 vs 0.77 minutes, p = 0.013 and 0.85 vs 0.56 minutes, p < 0.001, respectively). Tumor volume percentage overlap was higher with the aid of iVR models compared with CT alone (42% vs 28%, p = 0.05); this difference was significant among faculty (33% vs 47%, p = 0.033). When comparing faculty and residents, percentage overlap was not significantly different for both the CT session (faculty: 33% vs residents: 26%, p = 0.84) and the CT+iVR session (faculty: 47% vs residents: 42%, p = 0.11).
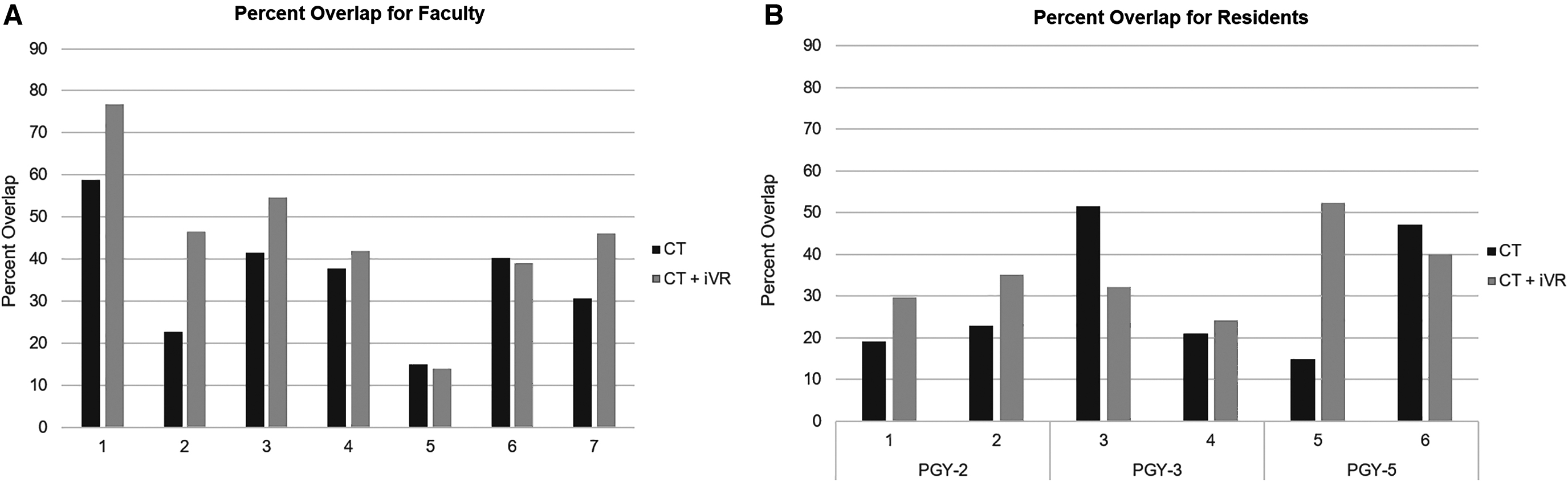
To assess the impact of level of training on the degree of tumor overlap, participants were further stratified based on their clinical experience (post graduate year status for residents and <10 vs 10–20 vs >20 years for faculty); there were no significant differences in percentage overlap with CT only vs CT+iVR among the residents nor among the faculty subgroups. In addition, the number of models with zero tumor overlap sessions among faculty was significantly lower in the CT+iVR sessions (19% vs 4.3%, p = 0.021). There was no difference when comparing errors made in the X, Y, and Z planes (Table 1). The mean percentage overlap for each participant is shown in Figure 2; of the 13 participants, 9 demonstrated overall improvement in tumor placement with the addition of iVR.
Mean percentage overlap of placed and actual tumor using CT alone vs CT+iVR for
Comparison Between CT only and CT+Interactive Virtual Reality Sessions Among Faculty and Residents
Bold indicates statistical significance.
Continuous nonparametric data displayed in median and interquartile range.
iVR = interactive virtual reality.
Univariate analysis of tumor characteristics
The correlation between tumor characteristics, based on the respective components of the R.E.N.A.L. nephrometry score, and accuracy of tumor localization was analyzed (Table 2). In both sessions (i.e., after viewing CT only and after viewing CT+iVR), participants were more accurate in locating tumors >4 cm in maximal diameter, having <50% exophytic component, ≤4 mm from the collecting system, and tumors that had >50% of their mass extending beyond the polar lines based on the R.E.N.A.L. nephrometry criteria.
Correlation Between Tumor Characteristics and Accuracy of Tumor Placement
Bold indicates statistical significance.
Continuous nonparametric data displayed in median and interquartile range.
NA = not applicable.
Overall, the tumor volume percentage overlap was highest in high complexity tumors (i.e., nephrometry score 10–12) compared with medium (7–9) and low complexity tumors (4–6) for both the CT only session (51% vs 24% vs 1.9%, p < 0.001) and the CT+iVR session (67% vs 41% vs 12%, p < 0.001). When comparing the accuracy of tumor placement between the two sessions, the degree of overlap of anterior tumors (28% vs 55%, p = 0.015) and tumors with high nephrometry score (51% vs 67%, p = 0.039) significantly increased when iVR models were viewed.
Multivariate analysis
Regression analysis was utilized to determine the independent relationship of the imaging modality with the accuracy of localizing the renal tumors. The addition of iVR to CT imaging was a positive predictor of a percentage overlap greater than the median overlap of 38%, when controlling for level of experience and tumor properties (odds ratio 2.22, 95% confidence interval 1.04–4.78, p = 0.039).
Questionnaire responses
Analysis of the participant questionnaire is illustrated in Table 3. All participants had in general a better understanding of the tumor location and shape, renal vasculature, and collecting system anatomy after viewing CT+iVR. Subanalysis of the questionnaire data among attendings and residents demonstrated that the significant benefit of iVR was maintained among attendings in understanding the tumor location and shape. Overall, 9 of 13 (69%) of participants strongly agreed that the use of CT with iVR improved their ability to locate the tumor with greater certainty.
Questionnaire Data
Bold indicates statistical significance.
Discussion
We hypothesized that exposure to an iVR model would enhance the surgeon's comprehension of the precise location of a renal tumor. Attendings and residents had an initial percentage volume overlap between the perceived tumor location and the actual tumor location of 33% and 26%, respectively, when viewing only the CT images. These relatively low scores suggest that, at various levels of experience, there is significant lack of understanding the tumor's location when viewing 2D images alone.
Overall, tumor localization was improved after viewing the iVR models, with percentage volume overlap between imaging and actual tumor location increasing from 28% to 42%. The added value of iVR was most pronounced among faculty surgeons; the percentage volume overlap among attendings significantly increased (from 33% to 47%) whereas the incidence of cases with zero overlap significantly decreased (from 19% to 4%); of interest, the faculty invariably spent more time than the residents in positioning the virtual tumor on the kidney. Consistent with these findings was that only attendings reported a significantly improved understanding of the tumor location and shape after viewing the iVR model.
Somewhat to our surprise, when tumor parameters were stratified by their individual R.E.N.A.L. nephrometry score components, participants performed better for tumors with a higher nephrometry score. During both sessions and regardless of the imaging modality (CT only or CT+iVR), the accuracy of tumor placement was better for larger as well as for more endophytic tumors. Similarly, tumor volume overlap was also greater, independent of the imaging modality used, for tumors that were closer to the collecting system and for tumors that extended across a polar line. The degree of tumor overlap increased for all tumors with the addition of iVR, but this difference only reached statistical significance for tumors with the highest nephrometry scores (10–12). These findings suggest that when the tumor's nephrometry score is high, the surgeon may pay more attention to its position with regard to its vascular supply and proximity to the collecting system.
Wake and colleagues, using seven 3D-printed renal tumor models, have recently shown that among three experienced surgeons, there was marked difficulty in accurately localizing renal tumors, especially if they were small and endophytic. 5 Our study concurs with the former but differs with regard to the endophytic complex nature of a tumor; in their study there was only one high complexity tumor. In their study, the mean overlap of 20 CT/MRI viewed tumors by three experienced surgeons was 24%. This was similar to our findings in which the degree of overlap after CT alone was only 26% and 33% for residents and faculty, respectively. When CT was combined with iVR, the overlap, despite high complexity tumors, increased to 47% for experienced urologists, but failed to change for the resident participants. Also, in their study, the degree of overlap was not significantly affected by the nephrometry scores or the relative endophytic component, whereas in our study, with a larger number of tumors analyzed, both the complexity of the tumor and the endophytic nature of the tumor augured for a greater degree of overlap.
Other groups have similarly demonstrated the benefits of preoperative modeling of a renal tumor using non-VR technology in preoperative planning, surgical training, and patient counseling. 8,11,12 Consequently, the implementation of 3D printing technology in urologic surgery could possibly translate into improved surgical outcomes; however, this remains an untested hypothesis. 13,14 Of note, 3D printing technology is time consuming, not immediately available as it invariably is done off-site, and is expensive ($460–$1000/model). 14 In addition, 3D-printed models only offer surgeons an isolated surface level representation of anatomical structures that cannot be deconstructed; they also are “out of context” in that the surrounding anatomy is not present.
Current viewing software has the ability to create a volume-rendered 3D reconstruction from CT images that can be displayed on a standard screen; this technology has been shown to be of value for preoperative planning in minimally invasive kidney surgery. 15 –17 However, what remains a limitation of this function is that the 3D-rendered image can only be displayed on a 2D screen and is neither immersive nor interactive. Another modeling approach, holographic reconstruction (HR), is a relatively new technology that, similar to iVR technology, generates digital 3D models using manual segmentation of DICOM files. Similar to iVR, HR offers an interactive experience; the digital 3D model is viewed on a headset or stereoscopic screen coupled with tracking eyewear. Compared with standard 2D CT images, HR was found to enhance surgeons' understanding of the renal tumor's position within the kidney and of the overall renal anatomy; however, this technology is yet to be tested clinically during renal surgery. 18
Virtual reality technology is readily available and relatively inexpensive, as the software and headset can be used countless times. Moreover, iVR displayed on a headset offers both an interactive and immersive experience during which the surgeon can view the kidney and its surrounding anatomy, and can then proceed to focus on the tumor itself and literally deconstruct the kidney such that the base of the tumor can be viewed. Indeed, other studies of virtual reality and PN have documented enhanced tumor localization and improved operative parameters: shorter operative time, less ischemia time, reduced blood loss, and decreased hospital stay. 9,10,19
In our prior study with patient-specific iVR models for preoperative PN planning, viewing the iVR models altered the surgical plan in upward of 50% of cases. 20 Examples of changes to the operative plan included wider tumor resection at a specific location to ensure a negative margin and better understanding of vascular anatomy, leading to modifying the approach for the hilar dissection. Also of note in our study was that the degree of overlap increased despite a reduction in the time to position the “virtual” tumor on the “erased” kidney, indicating perhaps a more rapid grasp of the anatomy given the immersive and interactive nature of the iVR model. Similarly for living donor nephrectomy, surgeons reported that the preoperative viewing of an iVR rendering of the patient's kidney improved their understanding of the surgical anatomy, frequently resulting in alteration of their original surgical plan, particularly with regard to dissection of the renal vessels. 21 Furthermore, viewing iVR models before percutaneous nephrolithotomy improved surgeons' understanding of the relevant anatomy and also altered the surgical approach in 40% of cases specifically with regard to selection of the optimal calix of entry and the sequence of stone removal. 22
It is our contention that the potential benefits of iVR extend beyond preoperative planning. As VR technology becomes widely available and more affordable, its implementation as an intraoperative tool may aid in decision making during surgery in which a renal tumor is endophytic or during a donor nephrectomy in which there are multiple renal arteries. VR would be an outstanding addition to current robotic technology and one that may not be too great a leap given that the surgeon is already using what amounts to a headset.
Presently, the creation of iVR models is dependent upon the experience of the individual who is charged with reading the CT and segmenting the various renal structures (veins, arteries, collecting system, renal parenchyma, renal tumor, etc.). This study is both time consuming and tedious. Developments in artificial intelligence have led to automated methods capable of accurate segmentation of the renal contour with an overall performance that is similar to human-to-human interobserver agreement. 23,24 As machine learning algorithms improve, they will be better able to differentiate normal kidney parenchyma, renal tumors, collecting system, and renal vasculature. When this level of sophistication is reached, the segmentation process can be automated. We anticipate this segmentation of the CT scan could then be integrated into the CT viewing panels such that one could select an iVR panel and proceed to use a VR headset for an immersive interactive experience using one's laptop or desktop computer.
There are two major limitations to our study. First, surgeons participating in the study had different levels of training and expertise, which likely contributed to the wide variation in the accuracy of tumor placement. This was certainly most notable when comparing the resident scores with the scores of the urology faculty. Second, iVR model creation involves manually tracing the desired anatomy on each slice of the CT scan, this requires 2 to 3 hours per rendering and is much dependent upon the ability of the person creating the model. In this study two individuals created the models and thus there may have been some variability in the VR rendering.
Conclusions
The addition of patient-specific iVR models to standard CT imaging improved the ability of postgraduate faculty urologists to accurately configure the location of a renal tumor. This improvement was most significant for the most complex renal tumors.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
This study was funded by Curiosity and Innovation Laboratory at UC Irvine.