
Abstract
Introduction:
Ejaculatory dysfunction is a common complication of surgeries for benign prostatic obstruction. It causes a clear deterioration in quality of life. Techniques have been developed to attempt to preserve antegrade ejaculation (AE). Our objective was to analyze results of ejaculatory function using an AE preservation technique during anatomical vaporization with XPS 180-W.
Methods:
Between 2017 and 2019, sexually active patients were treated using this technique by the same surgical team. A questionnaire (MSHQ-EjD Short Form) was mailed, patients who did not answer were contacted by phone or personally during follow-up. Responses were analyzed. Voiding function was evaluated using International Prostatic Symptoms Score (IPSS), Qmax, and postvoid residual volume. t-Test for paired samples was used to compare conformity of patients with and without AE and voiding results. A p < 0.05 was considered statistically significant.
Results:
In total, 77 of 112 patients (68.8%) completed questionnaires and were included. Mean age was 64.1 years (standard deviation [SD] 6.9) and median prostate size was 57.2 g (interquartilic range 30–85). A total of 68 of 77 (88.3%) patients reported AE. Of these, 58 (85.3%) reported AE always or most of the time and 10 (14.7%) reported AE half of the time. In total, 42 (61.7%) patients had preserved strength or slightly less than before the procedure, and 33 (48.5%) reported the same or slightly less volume than before. In terms of satisfaction, the average response values of patients with preserved AE and ejaculatory disfunction were 0.97 (SD 1.12) and 2.7 (SD 1.78), respectively (p = 0.000).
Pre- and postoperative variables were as follows: mean Qmax was 11.6 mL/sec vs 19.6 (p = 0.00), mean IPSS was 13.8 vs 8.9 (p = 0.000), and mean postvoiding residual urine was 125.3 vs 33.1 mL (p = 0.00), respectively.
Conclusion:
It is feasible to perform the AE preservation technique with anatomical vaporization XPS 180-W. In our medium size prostate series, we had a satisfactory patient perception of the ejaculatory function and satisfactory voiding function results.
Introduction
Bladder outlet obstruction (BOO), secondary to benign prostate hyperplasia, is a frequent condition associated with aging men. This condition leads to lower urinary tract symptoms (LUTSs) that are a common complaint and have a major impact upon their quality of life. 1 Clinical practice guidelines recommend various surgical approaches for the treatment of benign prostatic obstruction (BPO). 2
One of the surgical alternatives is laser vaporization using GreenLight XPS 180-W system (XPS 180-W), product of the evolution of the 60 W potassium–titanium–phosphate (KTP) laser presented in 1998. 3 There have been many techniques described as regards the use of green laser: vaporization, incision technique, vapoenucleation, enucleation, and also mixed techniques that respect the principles of enucleation but vaporize the tissue avoiding the use of the morcellator. 4,5 This technique is called “anatomical vaporization.” 6,7
One of the most common complications in the surgical treatment of BPO/LUTSs is ejaculatory disfunction (ED), present in 65% to 80% of cases. 2 It is a frequent reason for refusal to surgery, especially in young adults, and is associated with a clear deterioration in the quality of life. 8 In the 1990's a technique for the preservation (PT) of antegrade ejaculation (AE) during transurethral resection of the prostate (TURP) was presented and has not failed to show astounding results. 9 To our knowledge, there are no studies that analyze the results of ED with a PT using XPS 180-W.
The aim of this study is to analyze the results of ejaculatory function using the ejaculatory preservation technique during anatomical vaporization with XPS 180-W.
Methods
A retrospective observational study was conducted in patients with BPO who were treated with anatomical vaporization and AE preservation technique with XPS 180-W. In our analysis, we have included patients who had been treated between March 2017 and May 2019. In all 117 patients were operated using this technique and 5 patients with no sexual activity were excluded. We included 112 patients treated by the same surgeon. After approval by the hospital's ethics committee (Protocol number 0020-2019), a Spanish translation of the Male Sexual Health Questionnaire on Ejaculatory Dysfunction (MSHQ-EjD Short Form) 10 was extended to them through e-mail. Patients who did not answer were contacted by phone or personally during follow-up.
The questionnaire consists of four questions: three of them concerning the characteristics of ejaculation (frequency, force, and volume) and one concerning satisfaction with the results. To analyze the satisfaction section, the last question includes a scale from 0 to 5, in which 0 represents having “no problem with ejaculation” and 5 represents being “extremely dissatisfied” with the results. We assessed voiding functions 3 months after the surgery with International Prostatic Symptom Score (IPSS), uroflowmetry, and postvoid residual urine by sonography. Variables are described as mean and standard deviation (SD) or median and interquartilic range (IQR) depending on normal distribution or not. We used the t-test for paired samples to compare quality of life in question 4, between patients with and without ED, and for voiding function. A p < 0.05 was considered statistically significant. A logistic regression model was performed to search for association between AE and variables such as total energy used, size of prostate, time of surgery, and patient age.
Description of anatomical vaporization with preservation technique
After the spinal block or general anesthesia (in patients who had contraindicated or did not wish for a spinal block), the patients were placed in lithotomy position. An urethrocystoscopy with a 20F cystoscope and 30° optics is performed to identify the ureteral meatus and its distance from the bladder neck. Endoscopic prostate anatomy and distance to the external urinary sphincter are analyzed. If visible, the ejaculatory ducts are identified (Fig. 1). V-107 four-way irrigation equipment is used.
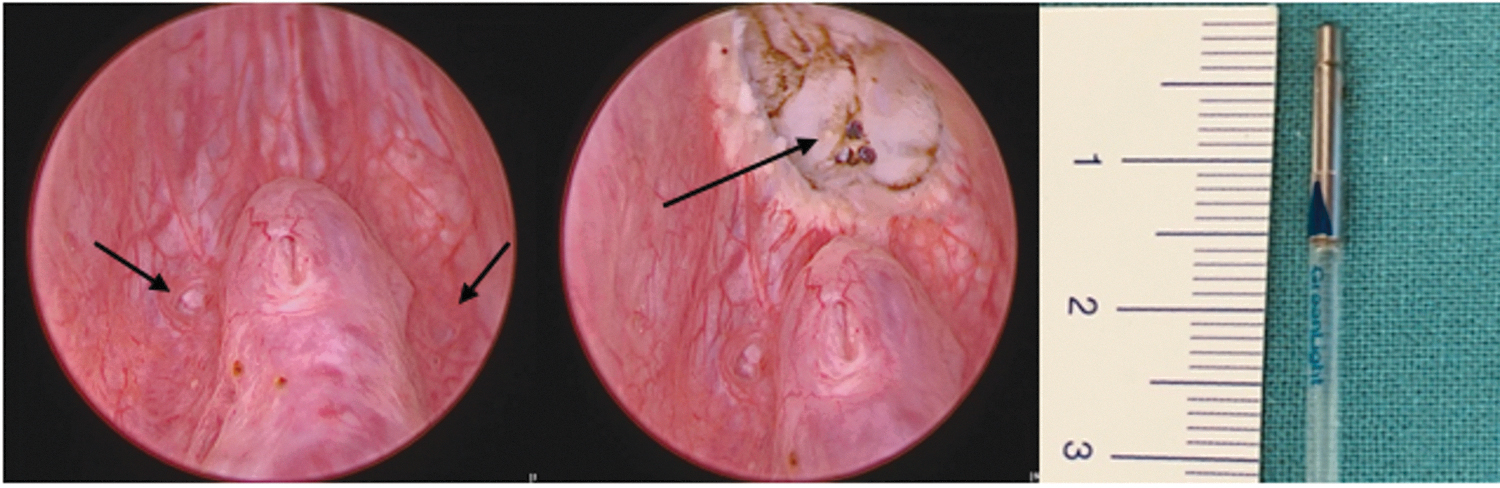
From left: cystoscopic view of verumontanum and meatus of ejaculatory ducts (black arrows); cystoscopic view after demarcation showing plane to be preserved (black arrow); measurement ∼1 cm from distal end of fiber to blue mark.
With a power of 120 W, a U-shaped incision is made, prioritizing a 1 cm proximal to the verumontanum (Supplementary Video S1). The end of the fiber is used as a parameter (Fig. 1). Two incisions are made, up to the capsular plane, at hours 5 and 7 at the level of the bladder neck that extend to the U-shaped incision previously described delimiting the medial lobe. The dissection of the medial lobe is continued following the plane between the capsule and the prostatic adenoma on both sides of the capsule, focusing on maintaining a sheet of tissue at 6 o'clock position that prevents the retropulsion of the dissected medial lobe toward the bladder. Once the dissection is completed, the medium lobe is vaporized with a power of 180 W. With 120 W power, a wide opening of the bladder neck is made and the dissection and vaporization of the side lobes proceed. An incision is made in 1 to 2 hours on the left side of the patient, from the bladder neck to the U-shaped incision described previously and is deepened until it reaches the capsular plane. The dissection is continued posteriorly, taking special care to maintain a thin line of tissue near hour 5 that prevents retropulsion of the dissected side lobe into the bladder. Once the dissection is completed, the left lobe is vaporized using a power of 180 W from the medial or lateral edge of the lobe. The same procedure is then performed on the right side.
Once the hemostasis has been checked, a triple-track 20F bladder catheter is placed with continuous washing, which is maintained during the first hours of the postoperative period. Throughout the next morning, the bladder catheter is removed and the patient is discharged from the hospital after spontaneous urination. Postoperative control with urine culture is performed 2 weeks after the procedure.
Results
In total, 77 patients out of 112 (68.75%) patients completed the questionnaire and were taken into consideration for analysis. Patients' mean age was 64.1 years (SD 6.9) and the mean prostate size was 57.2 g (IQR 30–85). Median follow-up was 16 months (IQR 10–26). AE was reported by 68 patients (88.3%). Of these, 58 (85.3%) reported AE “all the time or most of the time” and 10 (14.7%) reported “about half of the time or less than half of the time” (Fig. 1). When analyzing the strength of ejaculation, 42 (61.7%) patients answered “as strong as it was or a little less strong than it used to be” than before the procedure, 21 (30.9%) patients had “somewhat less or much less strong,” and 5 (7.3%) patients referred “very much less strong.” With regard to volume analysis, 33 (48.5%) patients answered “as much as it was or a little less than it used to,” 26 (38.2%) patients answered “somewhat less or much less,” and 9 (13.2%) patients answered “very much less” volume (Fig. 2). In terms of satisfaction, the average response values of patients with preserved AE and ED were 0.97 (SD 1.12) and 2.7 (SD 1.78), respectively (p = 0.000).

Volume, strength, and frequency of patients with preserved antegrade ejaculation.
Pre- and Postoperative variables were as follows: mean Qmax was 11.6 mL/sec (SD ±5.7) vs 19.6 (SD ±10.3) (p = 0.000), mean IPSS was 13.8 (SD ±4.2) vs 8.9 (SD ±5.8) (p = 0.000), and mean postvoiding residual urine was 125.3 mL (SD ±85.4) vs 33.1 (SD ±26.1) (p = 0.00), respectively.
Univariate logistic regression model showed no statistical association between AE and total energy used, size of prostate, time of surgery, and patient age.
Discussion
Sexual health has an important role in the quality of life and ED can have a substantial detrimental effect. The BOO treatment strategy should take into account the patient's expectations about expected sexual outcomes. Kim et al. analyzed 91 sexually active patients who underwent holmium laser enucleation of the prostate 8 ; of the 87 patients who reported reduced ejaculate volume, 52.8% also had decreased orgasmic intensity and ∼10% were “dissatisfied and wanted to return the situation” because of this. In this era of patient-centered and evidence-based medicine and because of new technologies, there are more and more attempts to reduce this complication.
Toward the end of the 1990s, the first attempts to preserve ejaculation during TURP were made. Ronzoni and De Vecchis achieved 80% preservation by treating 45 patients, although they do not mention how the analysis was performed in the postoperative period. 9 In one of the largest samples, Alloussi et al. carried out preservation in 89 patients, achieving 91% AE for the 10th question of the IIEF-15 questionnaire. 11 Abdel-Basir Sayed in 2003 performed a nonrandomized comparison between 20 patients treated with preservation technique vs 20 patients treated with conventional TURP. 12 We highlight his study since he performed postoperative sperm analysis, reporting 85% preservation in the PT group vs 20% AE in the group that did not undergo preservation.
In terms of ejaculation satisfacion after Green-Light procedures, the evidence is scarce and there are only a few abstracts presented at congresses or symposiums. Talab and colleagues, in a series of 160 patients with mean prostate volume of 64 mL treated with GreenLight and PT, recorded 136 patients with AE (85%) with IPSS of 20.3 preoperatively vs 5.3 postoperatively. 13 Miyauchi et al. analyzed 24 patients of whom 22 (92%) referred AE by answering a direct question at 1 month postoperatively and report significantly improved mean IPSS, QoL score, and Qmax postoperatively at 6 months. 14 Both studies analyzed the results with nonvalidated questionnaires. Using the MSHQ-EjD Short Form in our series, patients report an 88% AE with efficient treatment of voiding obstruction, showing significant differences between pre- and postoperative IPSS, Qmax, and postvoiding residual urine.
In 1974 Marberger described as a crucial step for AE the closure of the bladder neck and the dilation of the posterior urethra for the formation of a pressure chamber where semen is accumulated during emission, with subsequent expulsion by the perineal floor muscles (mainly bulbocavernosus). 15,16 This concept, associated with the idea that retrograde ejaculation occurs as a consequence of the opening of the bladder neck during surgery, has since been transmitted among urologists. 17 However, there are authors who differ. In 1994, Gil-Vernet and colleagues performed ultrasound studies in adults during ejaculation. 18 They described the displacement of verumontanum toward caudal and anterior with the dilation of the inframontanal urethra, and the superposition of the emission and expulsion phases when a continuous flow was observed. This denotes the importance of the perimontanal tissue. In contrast, the preservation of ejaculation observed during the transurethral incision of the prostate has called the impact of the bladder neck closure on the ejaculation mechanism into question. 19,20 This was interpreted as a consequence of the preservation of the “preprostatic sphincter,” which prevents the return of seminal fluid to the bladder during ejaculation. These findings indicate the importance of preserving part of the supramontanal prostatic tissue to maintain AE and not bladder neck integrity. 21
Our study has limitations. We used a validated questionnaire that we proceeded to translate to Spanish. This is associated with a possible memory bias or subjectivity on the part of the patient as it is a self-administered questionnaire. 22 Furthermore, there were no objective studies of ejaculatory function before the procedure, beyond the reference of active sexual life on the part of the patients.
To summarize, in our medium size prostate series, 88.3% of patients answered concerning the preservation of AE. Out of these, >60% reported ejaculation with the same or slightly less force and ∼50% reported ejaculation with the same or almost the same volume.
Conclusion
We have found that it is feasible to perform the ejaculation preservation technique during anatomical vaporization with XPS 180-W. In our medium size prostate series, we had a satisfactory patient perception of the ejaculatory function results and a satisfactory voiding function.
Footnotes
Authors' Contributions
Writing and editing of the article and references search were carried out by L.B. and N.B. Supervision and references search were carried out by L.B., N.B., P.C., C.A.A.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.
Supplementary Material
Supplementary Video S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.