
Abstract
Objective:
To conduct a prospective and randomized controlled trial comparing contemporaneous transabdominal rigid ureteroscopy (TRU) with postoperative extracorporeal shockwave lithotripsy (SWL) in the management of migrated or residual stones during laparoscopic pyelolithotomy and ureterolithotomy in kidneys with either intrinsic or extrinsic abnormalities.
Materials and Methods:
From February 2016 to December 2019, 45 patients with migrated or residual stones following laparoscopic pyelolithotomy and ureterolithotomy were accrued and randomly divided into two groups. These patients all had either urinary tract obstruction distal to the stone or concomitant ipsilateral intrinsic or extrinsic pathology requiring laparoscopic intervention. Twenty-three patients underwent contemporaneous TRU, and 22 patients underwent postoperative SWL. Patients' demographics, perioperative variables, and follow-up data were collected. The primary outcome was the final stone-free rate (SFR) at the 2-month follow-up. Secondary outcomes included blood loss, operative time, change in serum creatinine, complications per Clavien-Dindo grading system, renal colic occurrence rate (RCOR), and postoperative hospitalization.
Results:
There was no significant difference in gender, age, body mass index, location, or stone burden between the two groups (p > 0.05). At the 2-month follow-ups, the SFR was higher in the TRU than the SWL group (p = 0.002), and the RCOR was lower in the TRU than the SWL group (p = 0.005). Postoperative hospitalization was also shorter for the TRU group. No significant difference was noted in the operative time, blood loss, change in serum creatinine, or perioperative complications (p > 0.05).
Conclusion:
Contemporaneous TRU is more effective and equally safe compared to postoperative SWL in the management of residual or migrated stones during laparoscopic pyelolithotomy and ureterolithotomy in kidneys with either intrinsic or extrinsic abnormalities.
Introduction
The current recommended treatment options for a ≤20 mm upper urinary stone are extracorporeal shockwave lithotripsy (SWL) and retrograde ureteroscopic lithotripsy (URS). 1 However, when there is obstruction distal to the stone, such as ureteropelvic junction obstruction (UPJO), or a concurrent intrinsic or extrinsic pathology involving the ipsilateral kidney, such as obstructing renal cyst, adrenal tumor requiring surgical intervention, solitary functioning kidney, or infected urinary stone (defined as persistent pyuria with sterile or multiorganism urine culture), then laparoscopic pyelolithotomy or ureterolithotomy can be a reasonable alternative. 2 –6 Stone migration may occur with the laparoscopic approach. 7 –9 Management options for these stones include contemporaneous rigid ureteroscopy through the trocar port or postoperative SWL after the distal stricture or the associated ipsilateral pathology is corrected. We conducted a prospective and randomized controlled trial to compare the safety and efficacy of these two treatment modalities for the residual or migrated stones.
Materials and Methods
This is a prospective randomized controlled trial. This trial was registered with the Chinese Clinical Trial Registry (ChiCTR): ChiCTR2000031520. Stone-free rate (SFR), calculated from the patients' 2-month follow-ups, was selected as the primary outcome for this study. Secondary outcomes included blood loss, operative time, change in serum creatinine, complications as per Clavien-Dindo grading system, renal colic occurrence rate (RCOR), and hospitalization.
SFR for laparoscopic pyelolithotomy combined with nephroscopy was 100% 10 and for SWL monotherapy was 62% 11 from previous reports. Assuming type I statistical error of 5% and type II statistical error of 10%, the sample size was calculated to be, at minimum, 13 patients in each group. To account for patients lost to follow-up and withdrawal, we decided to increase the sample size to either 25 per each arm or to the number of patients accumulated at the closing date of this study (December 31, 2019), but at the least 15% more than the calculated sample size, whichever occurred first.
We used a raffle method for the randomization. Twenty-five tickets, each with either transabdominal rigid ureteroscopy (TRU) or SWL printed on it, were placed in a box. When stone migration or residual stone occurred during laparoscopic pyelolithotomy or ureterolithotomy, the circulating nurse would draw a ticket from the box and inform the surgeon which methodology was to be followed.
Between February 2016 and December 2019, 45 patients with stone migration or residual stones following laparoscopic pyelolithotomy or ureterolithotomy were accrued. They were randomly assigned into two groups. Twenty-three patients underwent contemporaneous TRU, and 22 patients underwent postoperative SWL (Fig. 1). The study was approved by our institutional review board. Written informed consent was obtained from each patient.
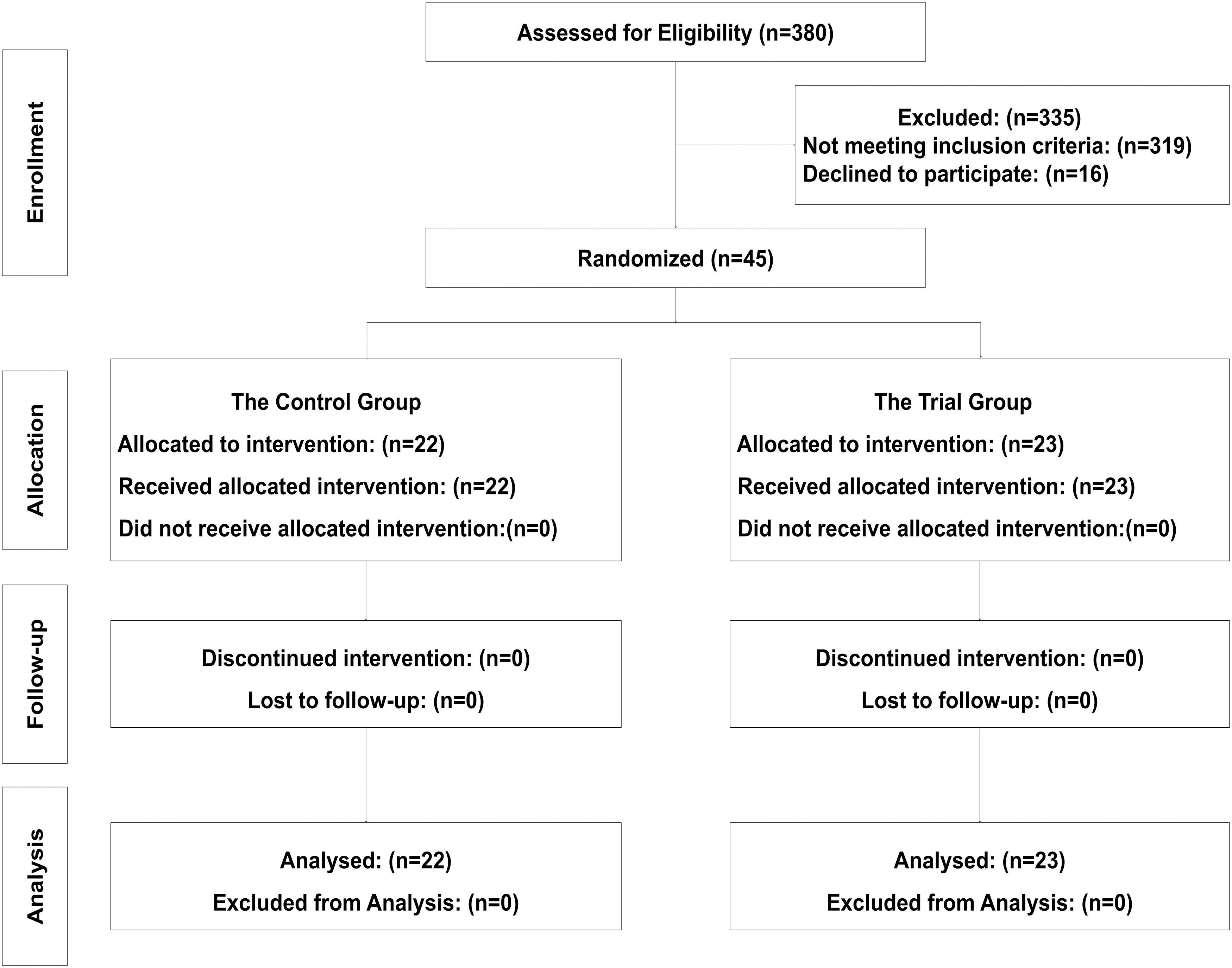
Consolidated Standards of Reporting Trials diagram for patient flow.
The inclusion criteria for patients were as follows: (1) older than 18 years old, (2) American Standards Association (ASA) ≤2, (3) ≤20 mm stones in the renal pelvis and upper ureter, and (4) a concurrent pathology, such as UPJO, 3,4 solitary functioning kidney, infected urinary stone, 5 obstructing renal cyst, or adrenal disease requiring surgical intervention. 6
The exclusion criteria were as follows: (1) distal ureter stricture, (2) acute urinary infection, (3) coagulopathies, (4) ASA ≥3, or (5) presence of renal or uroepithelial malignancy.
Patients' demographics data included the following: gender, age, body mass index (BMI), previous abdominal surgery, location and laterality of stone, stone burden, and concurrent pathologies. All patients had complete blood count, serum chemistry, urine analysis and culture, and CT before surgery. Positive urine cultures were appropriately treated. All patients received intravenous antibiotics 30 minutes before surgery for prophylaxis.
The laparoscopic procedure was performed under general endotracheal anesthesia in a 45–60° lateral and reversed Trendelenburg position with the affected side facing upward. Four transabdominal laparoscopic trocar ports were positioned on the ipsilateral side of the stone (Fig. 2B). A 10-mm port (B1) was placed 2 cm superior and 4 cm lateral to the umbilicus along the border of rectus muscle for the10 mm Storz laparoscope. A 5-mm port was placed inferior and lateral to the umbilicus along the same line (B2). This port was used for rigid ureteroscopy through the ureterotomy or pyelotomy to reach the renal pelvis and upper calices. It could also be used for accessory instruments. Another 10-mm port was placed in the lower quadrant of the abdomen, 2 cm anterior to the anterosuperior iliac spine (B3). This port was used for accessory instruments. The fourth 5-mL port was placed along the midclavicular line about 2 cm below the costal margin (B4). This port was used for accessing the mid and lower calices with the rigid ureteroscope. If the patient did not undergo contemporaneous ureteroscopy, then three trocar ports would suffice. The port underneath the costal margin (B4) was skipped. The descending or ascending colon (depending on the affected side) was medially mobilized to expose the psoas muscle and the ureter. Using preoperative images for guide and tactile feedback from forceps, the location of the stone could usually be determined. A longitudinal pyelotomy or ureterotomy was made for stone extraction or lithotripsy. In some cases, stone migration occurred, and the stones generally moved proximally into the renal pelvis or even the calix. In some other cases, there were additional stones elsewhere in the pyelocaliceal system.
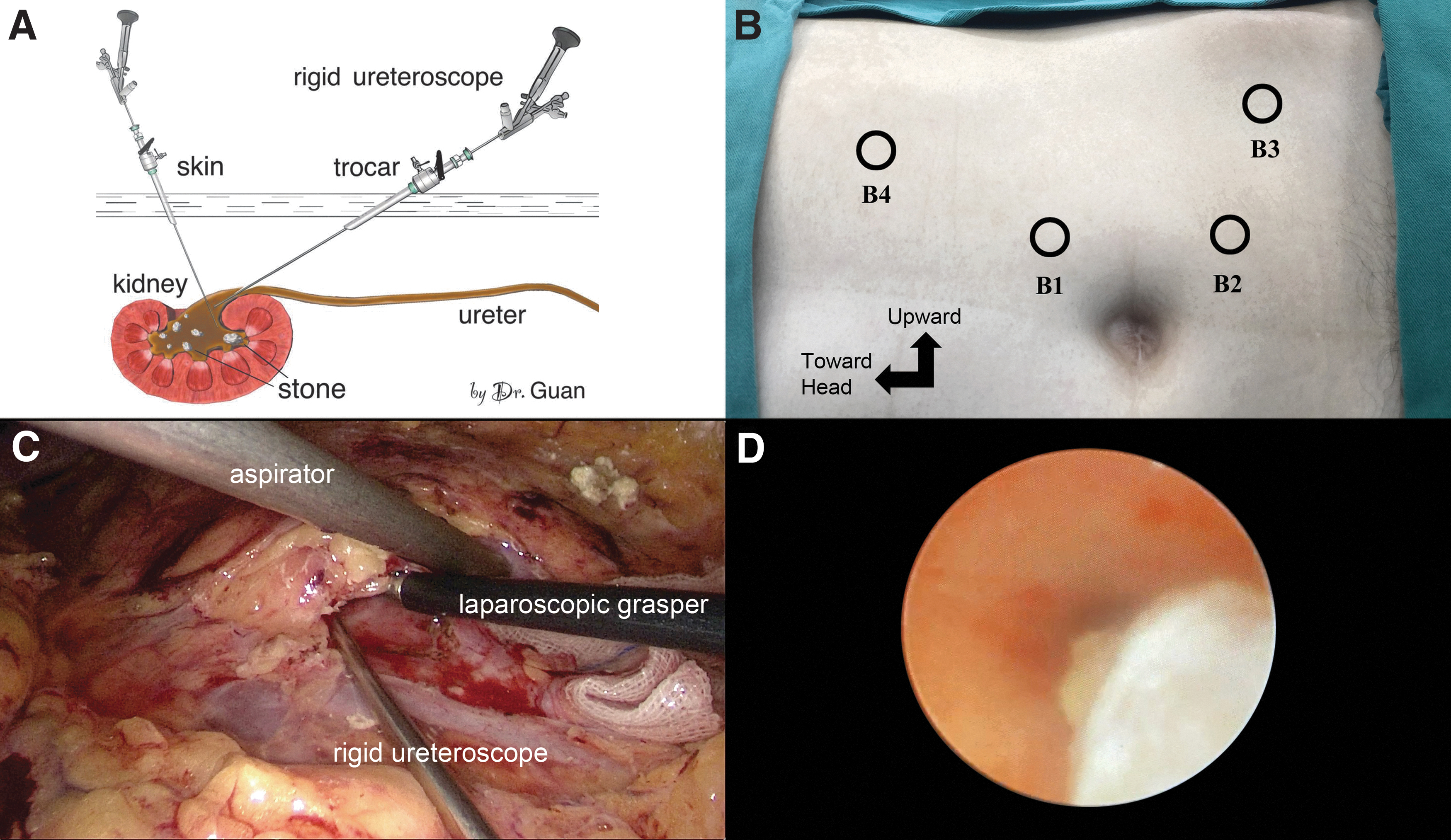
In the TRU group, an 8.0/9.8F in size and 430 mm in length Wolf rigid ureteroscope was introduced through the trocar. It was then inserted into the renal pelvis or ureter directly through the respective incision using a separate set of camera and video monitor. Gravity irrigation was used for the ureteroscopy. We generally raised the irrigation bag to about 50 cm above patient's heart. This height usually offered sufficient flow and pressure. The stones were extracted using a rigid grasper or stone basket. Pneumatic lithotripter was used to fragment the stone if it was too big to remove through the incision; alternatively, a laparoscopic grasper was used for extraction if the stone was too large for the ureteroscopic grasper. Generally, removing the migrated or residual stones in the upper and interpolar calices was quite straightforward. Occasionally, the migrated or additional stone was located in the lower pole calix. The lower pole of the kidney often had to be mobilized and tilted one way or other to facilitate visualization and extraction of the stones. Once the stone was removed, a Double-J stent was inserted into the ureter in an antegrade manner. The incision was closed with absorbable running suture. Next, pyeloplasty, ureteroplasty, excision or marsupialization of the renal cysts, or treatment for adrenal diseases was performed.
In the SWL group, after insertion of the Double-J stent and closing of the pyelotomy or ureterotomy incision, the concurrent pathology was similarly remedied. SWL was performed 1 week after the laparoscopic procedure. The voltage used for SWL ranged from 13 to 20 kV. The number of shock waves ranged from 1000 to 3000.
Postoperative treatment and follow-up
Low-dose CT was performed 3 days after laparoscopic surgery to assess the locations of stones in the SWL group and to confirm the clearance of stones in the TRU group. The Double-J stent was removed 1 month after the surgery. SFR was reassessed 1 month after the removal of the Double-J stent using low dose CT. SFR is defined as no visible residual stone on the CT scan. Patients' demographics, perioperative variables, and follow-up data were prospectively collected. The demographics included patients' gender, age, BMI, previous abdominal surgery, location and laterality of the stones, stone burden, and concurrent pathologies. The perioperative variables included blood loss, calculated by measuring the amount of blood in the suction container; operative time; change in serum creatinine; complications as per Clavien-Dindo grading system; and postoperative hospitalization. Follow-up data comprised SFR and RCOR. RCOR was defined as the presence of colicky pain after the removal of the Double-J stent that required outpatient analgesics and/or antispasmodic treatment or hospitalization. Stone burden was assessed by stone size and number. The stone size was expressed by the largest diameter measured on the preoperative CT scan. In the case of multiple stones, the summation of the largest diameter of each individual stone was used. The operative time was delineated as laparoscopic pyelolithotomy or ureterolithotomy time plus TRU in the TRU group; it covered laparoscopic pyelolithotomy or ureterolithotomy time plus time for SWL in the SWL group. Treatment time for the concurrent conditions was excluded. Postoperative hospitalization ranged from the day of laparoscopic surgery to discharge.
Independent t-tests or rank sum tests were used for numerical variables. Chi-square tests or Fisher's definite probability methods were used for categorical variables. The difference was analyzed using SPSS 23.0 software. p ≤ 0.05 was set to be statistically significant.
Results
Comparison of patients' demographics is presented in Table 1. These included gender, age, BMI, previous abdominal surgery, location of stone, laterality, stone burden, and concurrent pathologies. There was no difference in any of the demographics between two groups.
Comparison of Patient Demographics
BMI = body mass index; SD = standard deviation; SWL = extracorporeal shockwave lithotripsy; TRU = transabdominal rigid ureteroscopy; UPJO = ureteropelvic junction obstruction.
Table 2 shows perioperative variables and follow-up data. SFR, the primary outcome of this study, was much higher in the TRU group (100%) than the SWL group (59.1%, p = 0.002). RCOR 1 month after the removal of the Double-J stent was lower in the TRU group (0%) than the SWL group (22.7%, p = 0.05). Hospitalization was also shorter in TRU vs SWL group (mean 5.2 ± 1.5 vs 8.8 ± 1.1, p < 0.05). There were two cases of fever in the TRU group and three in the SWL group. All resolved with antipyretic treatment (Clavien I) and p = 0.96. No urinary leakage, laparoscopic port infection, or intestinal obstruction occurred. No significant difference was noted in the operative time, blood loss, or change in serum creatinine (all p > 0.05).
Comparison of Perioperative and Follow-Up Variables
Discussion
Treatment options for upper ureteral and pelvic stones include SWL, URS, percutaneous nephrolithotomy (PNL), and laparoscopic and open surgery. 1 URS and SWL are the first-line treatments for most ureteral and renal stones ≤20 mm in size. However, if there is urinary tract stricture distal to the stone, such as UPJO, or concurrent intrinsic or extrinsic pathology affecting the ipsilateral kidney, such as obstructing renal cyst, solitary functioning kidney, infected stone, or adrenal disease that requires surgical intervention, then laparoscopic or open surgery can be valid alternatives. 2 –6 Stone migration can occur with any type of surgical intervention. 7 –9 Generally, stones migrate in antegrade manner, from the pelvis to the calix or from the ureter to the pelvis or calix. Many factors can affect stone migration. These include the stone diameter, severity of impaction, degree of hydronephrosis, and others. 7 Due to the limitations of the laparoscopic instruments, stone migration can be a problem for laparoscopic urolithotomy.
SWL is recommended for stones ≤20 mm in the renal pelvis and upper or middle calices. 1 However, in general, SWL is associated with a lower SFR and a higher retreatment and auxiliary procedure rate, especially as the stone size increases. 12 Moreover, SWL results in a lower SFR in patients with renal cysts or with polycystic kidney disease. Renal cysts seem to interfere with stone passage. 13,14 SWL was also reported to be less effective in patients who had previous pyeloplasty. 4
Rigid ureteroscopes are generally smaller than 12F in size. They can be easily inserted through the laparoscopic ports, as well as into the pyelotomy and ureterotomy. They can be ideal adjunctive instruments for laparoscopic stone surgery. Flexible endoscopes can also be used with the laparoscopic procedure. The combined use of laparoscope with flexible endoscopes has been reported. 15,16 However, operation with flexible endoscope is more technically demanding; may result in lower SFR 17 ; and incurs a higher cost. 18
Stone migration and residual stones during laparoscopic urolithotomy is a challenging problem. There is no consensus on the best treatment options. We generally use either contemporaneous TRU or postoperative SWL to manage these patients. There is no literature showing which treatment modality is superior; hence, we embarked on the present trial.
In this study, the SFR was 100% for the TRU group, and there were no cases of renal colic 1 month after ureteral stents were removed. In contrast, SFR was only 59% for the SWL group, and there were five cases of renal colic. Patients who received postoperative SWL still had to pass the stone fragments, thus the higher RCOR.
There was no significant difference in the safety parameters between the two groups. The operative time and blood loss were comparable, and there was no significant difference in perioperative complications or serum creatinine changes. Postoperative hospitalization was longer in the SWL group than the TRU group, (p < 0.05).
Combining laparoscopy with rigid ureteroscopy can be a useful tool for urolithiasis. Under laparoscopy, a ureteroscope can be introduced into the renal pelvis or calix. The stones are visualized and then extracted using a stone basket or forceps. The larger stones can be fragmented with lithotripter or teased out of the pyelocaliceal system and then removed with laparoscopic forceps.
We found a few caveats to this technique. It is important that the axis of the rigid ureteroscope is close in line with the axis of the ureter, renal pelvis, or calix that contains the stone, to facilitate its exploration and extraction and to decrease the risk of excessive torque that can potentially tear the wall of the renal pelvis or ureter. The ipsilateral port located below the umbilicus and along the rectus muscle border is the best rigid ureteroscopic route for stones in the renal pelvis and upper calix. The middle and lower calix, on the other hand, is a blind area for this approach. For stones in these calices, we usually introduced the rigid ureteroscope through the ipsilateral port that is below the costal margin. Furthermore, it is often helpful to mobilize the lower pole of the kidney and to tilt it upward and outward to better expose the stones.
If the stone migrated into renal pelvis during ureterolithotomy and the ureterotomy is too distal to the pelvis, we recommend a separate pyelotomy for the insertion of the rigid ureteroscope. Using pressurized irrigation through the ureteroscope can be beneficial. It dilates the renal pelvis to allow better visualization and sometimes even flushes out the stones. Finally, it is more important to prevent stone migration than to treat migrated stones. We generally take advantage of gravity by placing the patients with their affected sides facing upward and in a 25° reverse Trendelenburg position.
Our hospitalizations tend to be much longer than those of western nations. China has a universal health insurance through the government. It only covers the in-hospital expenses. The hospital cost is set by the government and is extremely low. Consequently, patients tend to stay in the hospital until they feel that they are pain free and fully recovered from the surgery.
The major limitation of this study is that it is a single center trial. A multicenter study would be beneficial to further validate our findings.
Conclusions
Contemporaneous TRU is equally safe but more effective than postoperative SWL for the treatment of migrated or residual stones during laparoscopic pyelolithotomy and ureterolithotomy in kidneys with either intrinsic or extrinsic abnormalities.
Footnotes
Acknowledgment
The authors thank Professor Shaw P. Wan, MD, for his contribution in advising and editing this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.