
Abstract
Background:
T1, high-grade, nonmuscle-invasive bladder cancer (NMIBC) is characterized by a high recurrence rate and progression to muscle-invasive disease concerns a significant number of patients. To overcome limitations of initial transurethral resection of bladder tumor (TURBT), various strategies are proposed in the literature. One of them is performance of restaging TURBT (re-TURBT). In recent years, it has been shown that re-TURBT can provide valuable additional pathologic information. However, its potential effect on survival improvement is debatable and benefits from this procedure have been suggested to be dependent on several clinicopathological factors (e.g., the presence of detrusor muscle in initial TURBT).
Evidence Acquisition:
A systematic search was conducted within the three electronic databases, including Medline, Scopus, and Embase. The following outcomes were retrieved: outcome measurements of recurrence-free survival (RFS), progression-free survival (PFS), cancer-specific survival (CSS), and overall survival (OS), including hazard ratios and 95% confidence intervals. Initially, a main analysis for each outcome (RFS, PFS, CSS, and OS) was performed. Subsequently, we conducted subgroup analyses for the following factors: T1 grade, presence of detrusor muscle in initial TURBT, and type of adjuvant intravesical therapy.
Evidence Synthesis:
Finally, six studies with overall 3257 participants were identified for this meta-analysis. A significant impact of re-TURBT on RFS, PFS, CSS, and OS was not found in the overall analysis that included all patients with T1 bladder tumors. On the other hand, subgroup analyses, including studies reporting cohorts with mixed T1 tumor grading, revealed that re-TURBT was associated with significantly better RFS, PFS, and OS.
Conclusions:
This meta-analysis shows that re-TURBT does not improve survival outcomes in patients with T1 tumors; however, results of some particular subgroup analyses indicate its potential positive impact on the subsequent course of the disease. Furthermore, high-quality, prospective, randomized controlled trials are necessary to make a final statement about the therapeutic role of re-TURBT in T1 NMIBC.
Introduction
Approximately 75
To overcome limitations of the initial TURBT, including risk of residual tumor omission or insufficient depth of resection, various strategies are proposed in the literature. 1,7,8 One of them is performing a restaging TURBT (re-TURBT) within 2 to 6 weeks from the first TURBT. According to EAU guidelines, re-TURBT is strongly recommended in patients with T1 tumors, regardless of whether the muscle layer is present in the initial TURBT specimen. 1,7 –9 In recent years, it has been shown that re-TURBT can provide valuable additional pathologic information. 7 –9 However, its potential effect on survival improvement is debatable and benefits from this procedure have been suggested to be dependent on several clinicopathological factors (e.g., the presence of detrusor muscle in initial TURBT). Therefore, it was decided to conduct a systematic review and meta-analysis of currently available literature.
Evidence Acquisition
Search strategy
A systematic search was conducted independently by two authors (W.K. and L.N.) within the three electronic databases, including Medline, Scopus, and Embase, according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 10 Additionally, resource centers from the biggest urological conferences were searched. The last search was performed on 31st March 2020. The Medical Subject Heading terms and/or key words and/or free words were “bladder cancer,” “transurethral resection,” “TURB*,” “restaging,” “repeat,” “second,” and “second look.” Boolean operators (NOT, AND, and OR) were used in succession to narrow and broaden the search. Only publications in English were considered and evidence was limited to human data.
Inclusion and exclusion criteria
In this meta-analysis, only studies that met the following criteria were included: (1) studies comparing the re-TURBT group with an observation group (no re-TURBT); (2) studies reporting data for patients with T1 tumors; (3) studies reporting at least one survival outcome; and (4) at least 1-year survival data being available in the study. Observational studies, reviews, case reports, letters, and commentaries were excluded, as well as trials on patients with clinical stage other than T1 NMIBC. Moreover, repeated publications from the same authors or institutions, except for publications with updated or new data from the same institution without double counting the patients, were excluded.
Data extraction
Two authors (W.K. and S.P.) independently screened titles and abstracts of the retrieved records. All potentially relevant studies were evaluated as full text, if available. In case of multiple reports of the same cohort, the most complete data aggregated with the longest follow-up duration were selected. Disagreements were resolved by consultation with other authors. The following data were initially extracted: first author, year of publication, study design, number of patients who underwent or did not undergo re-TURBT, inclusion and exclusion criteria of particular studies, participant demographics, and baseline tumor characteristics. Furthermore, the following outcomes were retrieved: outcome measurements of recurrence-free survival (RFS), progression-free survival (PFS), cancer-specific survival (CSS), and overall survival (OS), including hazard ratios (HRs) and 95% confidence intervals (95% CIs).
Quality and risk of bias assessment
The methodological quality of included nonrandomized articles was evaluated according to the Newcastle–Ottawa Scale (NOS), whereas for randomized studies, the Jadad Scale (JS) was used. 11,12 Funnel plots were used to assess the publication bias of included publications. Because the visual interpretation of funnel plot asymmetry is inherently subjective, we also performed the Egger test.
Statistical analysis
The statistical analysis was conducted using Review Manager 5.3 (The Nordic Cochrane Center, The Cochrane Collaboration, Copenhagen, Denmark) and Statistica 13.3.0 (TIBCO). If available, already reported HRs and 95% CIs were included into the meta-analysis. We preferred to collect multivariate analysis data, otherwise (if not reported) data from univariate analyses were extracted. In addition, if there were no direct data provided in the publication, HR and 95% CI were estimated using methods presented by Tirney et al. 13 The statistical significance of the pooled HRs was evaluated by the Z test. The heterogeneity I 2 index was calculated to indicate the proportion of inconsistency between studies that could not be attributed to chance. When I 2 < 50%, the evidence showed no significant heterogeneity and the fixed-effect model was used. Otherwise, a random-effect model was applied. For all tests, p < 0.05 was considered a statistically significant difference.
Evidence Synthesis
Study identification and quality assessment
Our search strategy initially identified 4505 articles (4492 from online databases and 13 from additional sources). The flow diagram of study selection with subsequent exclusions (with reasons) is presented in Figure 1. Finally, six studies were identified for quantitative analysis. 14 –19 The main characteristics of studies included in our meta-analysis are presented in Table 1. Included articles recruited overall 3257 patients, of which 1515 had re-TURBT and 1742 had only single initial TURBT. Of the six publications, five were nonrandomized 14,15,17 –19 and one was a RCT. 16 The median follow-up period of the studies ranged from 34 to 119 months. In most articles, adjuvant bacillus Calmette–Guerin (BCG) therapy (at least induction course) was reported, 15,17,18 while other studies included various adjuvant chemotherapeutics, 19 mitomycin C (MMC), 16 and even no application of adjuvant intravesical therapy (until recurrence). 14 Re-TURBT was predominantly performed between 2 and 6 weeks, 14,16 –18 whereas two articles reported other time intervals. 15,19
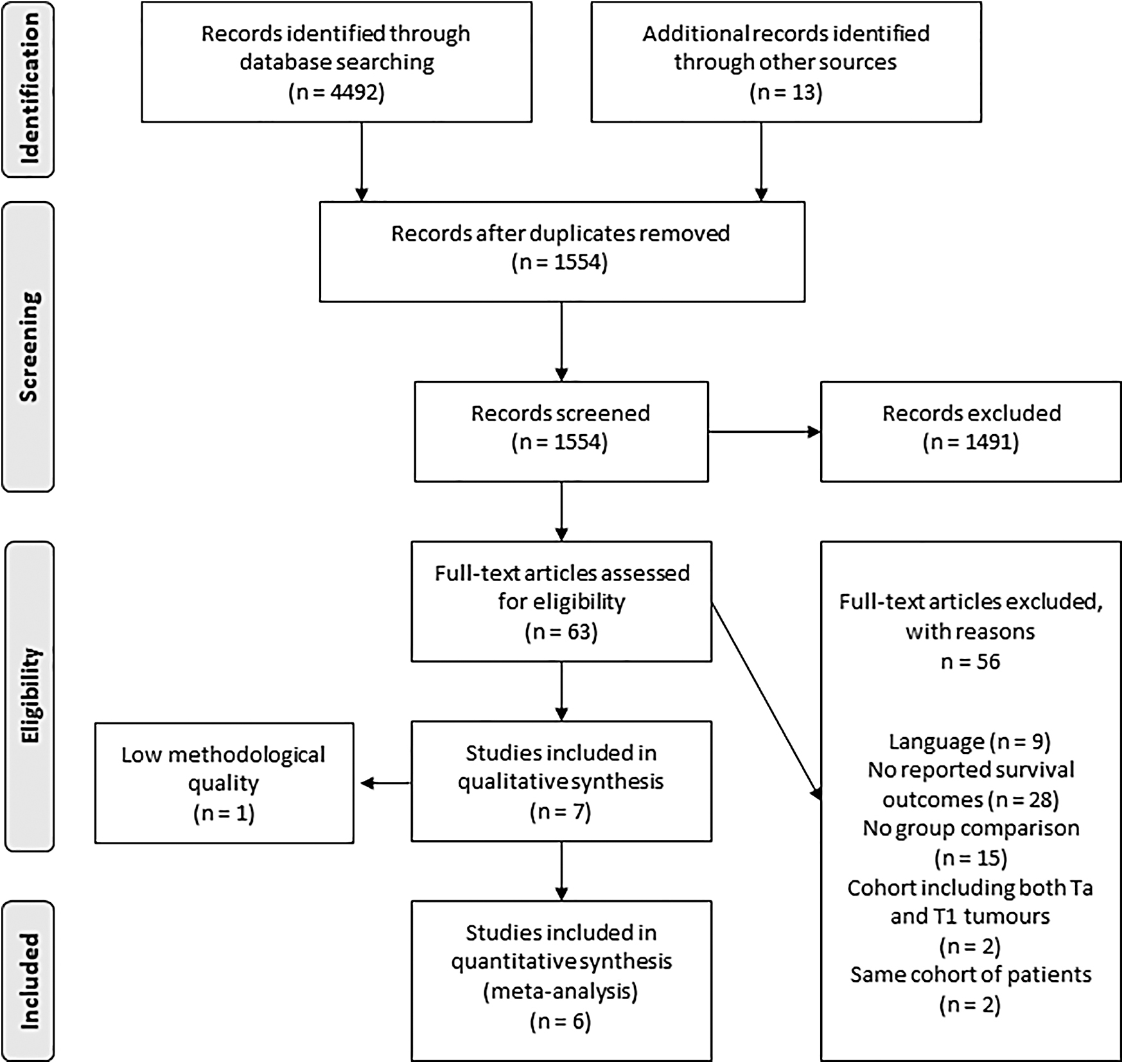
Flow diagram of study selection.
Baseline Characteristics of Included Studies
Newcastle Ottawa Scale score.
Jadad Scale score.
* Extension trial.
Intention-to-treat analysis.
HG T1 tumors.
BCG = bacillus Calmette–Guerin; CSS = cancer-specific survival; ERC = epirubicin; HG = high-grade; MMC = mitomycin C; NOS = Newcastle–Ottawa Scale; OS = overall survival; P = prospective; PFS = progression-free survival; R = retrospective; RCT = randomized controlled trial; re-TURBT = restaging transurethral resection of bladder tumor; RFS = recurrence-free survival; JS = Jadad Scale; TURBT = transurethral resection of bladder tumor.
Tumor characteristics at initial TURBT as well as reported residual disease and upstaging rates at re-TURBT are presented in Table 2. Of the six publications, four involved only patients with T1 HG tumors 14,15,17,18 and two included both patients with low-grade (LG) and HG cancers. 16,19 In the majority of studies, the detrusor muscle was present in all initial TURBT specimens. 14 –16,19 One study included both patients with and without detrusor muscle at first TURBT. 18 Furthermore, one article provided data for all patients regardless of detrusor muscle presence (which was used in our main analysis) as well as data for two separate subgroups (muscle at initial TURBT and no muscle at initial TURBT), which were used in our following subgroup analysis. 17 Reported presence of residual tumor and progression to MIBC at re-TURBT in included articles ranged from 18% to 71.3% 14 –19 and 1% to 7.6%, respectively. 14 –16,19
Tumor Characteristics at First Transurethral Resection of Bladder Tumor, Reported Residual Disease, and Upstaging Rates at Restaging Transurethral Resection of Bladder Tumor
LG = low grade; MIBC = muscle-invasive bladder cancer; NR = not reported.
Assessment of quality scores by the NOS showed that the scores of selected nonrandomized studies ranged from 7 to 9, while the JS score for the included RCT was 4, which was considered appropriate for the following meta-analysis.
Data analysis
For each outcome of interest (RFS, PFS, CSS, and OS), the main analysis, including data from all available publications, was performed (Fig. 2). Subsequently, we conducted subgroup analyses for the following clinicopathological factors: T1 grade (T1 HG only vs both T1 LG and HG tumors), presence of detrusor muscle in initial TURBT specimens (yes vs no), and adjuvant intravesical therapy (BCG vs other). Summary of all subgroup analyses is presented in Table 3.
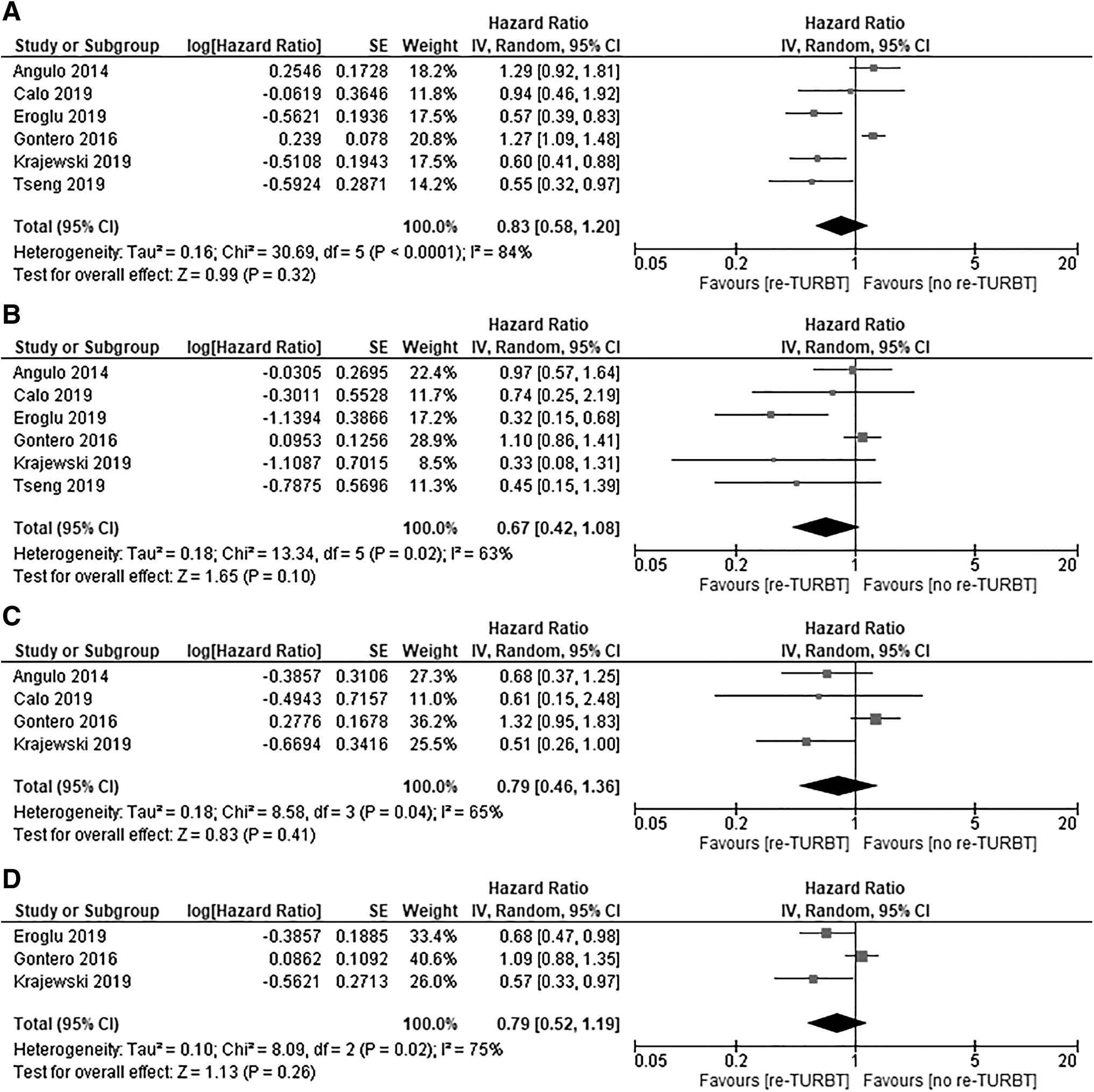
Forest plot of hazard ratio for
Subgroup Analysis for Recurrence-Free Survival, Progression-Free Survival, Cancer-Specific Survival, and Overall Survival
Statistically significant p-values are in bold.
In this analysis, from the study by Gontero et al., HRs and 95% CIs were obtained from two subgroups: muscle and no muscle.
95% CI = 95% confidence interval; HR = hazard ratio; I2 = heterogeneity index; NA = not applicable.
Comparison of RFS of re-TURBT vs observation
Data for RFS were reported in six studies. The pooled HR was 0.83 (95% CI = 0.58–1.20; p = 0.32), indicating that re-TURBT was not associated with significantly better RFS, compared with the observation (no re-TURBT) group (Fig. 2A). A significant heterogeneity was found between the trials (I 2 = 84%), thus a random-effect model was applied.
Subgroup analysis demonstrated that performing re-TURBT in patients with T1 HG tumors did not significantly improve RFS (HR = 1.01; 95% CI = 0.70–1.45; p = 0.96; I 2 = 78%). When two studies presenting patients with both LG and HG cancers were analyzed, re-TURBT was associated with significantly better RFS (HR = 0.56; 95% CI = 0.41–0.77; p < 0.001; I 2 = 0%). Other subgroup analyses did not confirm any significant differences for RFS (Table 3).
Comparison of PFS of re-TURBT vs observation
Data for PFS were extractable from six studies and a significant difference in study heterogeneity was observed (I 2 = 63%). Therefore, a random-effect model was used. The pooled HR was 0.67 (95% CI = 0.42–1.08; p = 0.10), indicating that re-TURBT was not associated with significantly better PFS, compared with the observation (no re-TURBT) group (Fig. 2B).
Once more, the subgroup analysis revealed that performing re-TURBT in T1 HG tumors did not significantly improve PFS (HR = 1.03; 95% CI = 0.83–1.28; p = 0.79; I 2 = 9%). Oppositely, analysis of two studies presenting mixed T1 grades (both LG and HG) showed that re-TURBT was associated with significantly better PFS (HR = 0.36; 95% CI = 0.19–0.67; p = 0.001; I 2 = 0%). Other subgroup analyses did not confirm any significant differences for PFS (Table 3).
Comparison of CSS of re-TURBT vs observation
Data for CSS were reported in four articles, with significant heterogeneity (I 2 = 65%), thus a random-effect model was applied. The pooled HR for CSS was 0.79 (95% CI = 0.46–1.36; p = 0.41), indicating that there was no significant difference between re-TURBT and observation (no re-TURBT) groups (Fig. 2C).
All studies included in the main analysis reported only HG T1 cancers, so a subgroup analysis regarding the mixed T1 grade was not feasible. Other subgroup analyses did not confirm any significant differences for CSS (Table 3).
Comparison of OS of re-TURBT vs observation
Data for OS were extractable from three studies. A significant heterogeneity was found between the trials (I 2 = 75%), therefore a random-effect model was applied. The pooled HR was 0.79 (95% CI = 0.52–1.19; p = 0.26), indicating that re-TURBT was not associated with significantly better OS, compared with the observation (no re-TURBT) group (Fig. 2D).
In the subgroup analysis, with only one study presenting mixed T1 grades (both LG and HG), re-TURBT significantly improved OS (p = 0.044). Other subgroup analyses did not confirm any significant differences for OS (Table 3).
Publication bias assessment
Funnel plots are presented in Figure 3. The results of Egger tests revealed no evidence for publication bias for RFS (p = 0.11), CSS (p = 0.20), and OS (p = 0.16). Potential publication bias for PFS (p = 0.047) was found. However, mixed grade cohorts and different sample sizes of particular studies might contribute to its occurrence.
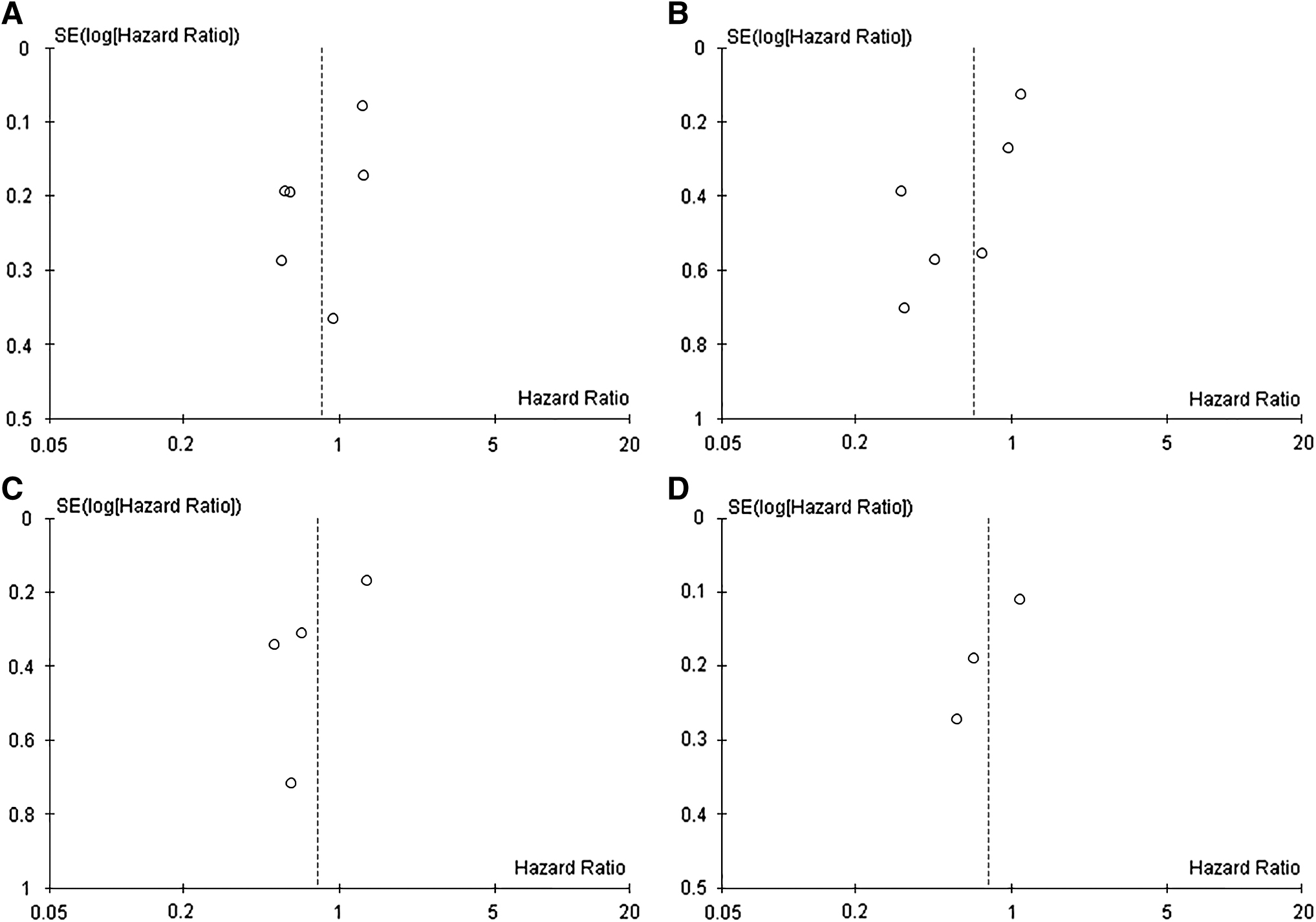
Funnel plot for the evaluation of potential publication bias:
Discussion
This meta-analysis included patients with T1 tumors and it was extended by subgroup analyses according to several important clinicopathological factors. To our best knowledge, this is the first meta-analysis comparing survival outcomes in patients with single vs re-TURBT in T1 tumors. A statistically significant association between performing re-TURBT and improvement in any survival parameter (RFS, PFS, CSS, and OS) was not found in the overall analysis, including all patients with T1 BCs. Despite this, some statistical trend (yet not significant) was noted for PFS (p = 0.1)
It ought to be emphasized that T1 LG, especially T1G1, is rather a rare clinical entity. It is proven that well-differentiated urothelial carcinoma has no propensity to infiltrate the bladder mucosa, and, in fact, T1 LG tumors are either upstaged or undegraded. 20 In our meta-analysis, vast majority of patients had T1 HG tumors, yet some studies used in this article included both patients with LG and HG cancers. Similar to the total study population, there were no statistically significant findings regarding any of the survival outcomes when articles presenting only patients with T1 HG cancers were analyzed. Interestingly, when studies including mixed tumor grading (both LG and HG), were analyzed, re-TURBT was associated with significantly better RFS, PFS and OS. That indicates a potential positive impact of re-TURBT on the subsequent course of the disease. However, it has to be mentioned that besides strong results, articles reporting on both LG and HG were not free from flaws other than heterogeneous grades. 21
Initially, comparative studies showed improvement in survival outcomes when re-TURBT was performed. Sfakianos and colleagues, in their retrospective article, compared RFS and PFS of patients treated with intravesical BCG for high-risk NMIBC. The median time to recurrence was significantly shorter for patients who received a single TURBT compared with those who also received re-TURBT. In addition, re-TURBT resulted in a significantly better 5-year PFS rate. 22 Oppositely, Kim et al. showed no difference in PFS rates between both groups; however, patients having re-TURBT had a significantly higher 2-year RFS rate (77.0% vs 45.8%). 23 Although abovementioned studies presented some evidences that re-TURBT could result in better survival outcomes, both of them analyzed tumors of mixed stages together (Ta and T1). The results might be severely biased and therefore could not be used in this meta-analysis. Subsequently, several comparative studies limited to patients with T1 tumors were published, which allowed performing this meta-analysis. Once more, the positive impact of re-TURBT on any survival parameter (RFS, PFS, CSS, and OS) was found neither in the overall analysis (including all patients with T1 BC) nor in the T1 HG subanalysis.
One of the major limitations of initial TURBT is the possibility of residual tumor omission and depth of tumor invasion underestimation. 24 To date, a few systematic reviews and meta-analyses provided data about residual tumor and upstaging rates at re-TURBT. In a systematic review presented by Cumberbatch and colleagues, residual tumors at re-TURBT in T1 cancers ranged from 20% to 71% and upstaging to muscle-invasive disease occurred in 0% to 32% of cases. 25 The most recent meta-analysis by Naselli et al., including also patients with T1 tumors, found a high pooled prevalence of 56% for residual tumors and 10% for upstaging to muscle-invasive disease at re-TURBT. Even if the detrusor muscle was present at initial TURBT, the corresponding rates were 47% and 10%. 26 The presence of residual tumors at re-TURBT in studies included in our meta-analysis ranged from 18% to 71.3%, which was similar to that reported by Cumberbatch and colleagues, while the reported upstaging rates were slightly lower, ranging from 1% to 7.6%. Consequently, re-TURBT should be indicated and performed to improve staging accuracy and achieve completeness of the surgical resection, as well as to implement appropriate sequence therapy. 27 However, because of issues such as health care costs, potential morbidity or patient discomfort, and no clear influence on survival, in general, re-TURBT is probably not associated with strong oncological benefit.
Some recent studies, also included in this meta-analysis, questioned the role of re-TURBT in T1 tumors when initial TURBT provided a histopathological specimen containing a reliable amount of detrusor muscle. It was suggested that performing re-TURBT in such cases might not result in a better oncological outcome, thus, as a potentially morbid procedure, it should be avoided. Results of our meta-analysis seem to confirm this approach because significant improvement in any survival outcome was not found when patients with detrusor muscle in the initial TURBT specimen were analyzed. On the other hand, based on the study by Gontero and colleagues, 17 which also provided data of patients without muscle at the initial TURBT, performing re-TURBT is reasonable in case the detrusor muscle is absent in the histopathological specimen at the first TURBT.
We have also tried to investigate the influence of adjuvant treatment on oncological survival, yet we have not found any significant associations. Data regarding intravesical treatment were substantially heterogenic regarding the type of drug, schedule, and dosage and therefore probably incomparable.
This meta-analysis has potential limitations, which need to be mentioned for interpretation of the results. First, it should be remembered that results of the included studies originate from referral centers with vast expertise in urological oncology and probably high quality of primary resections. Therefore, conclusions of this meta-analysis may not be true for less experienced centers. Second, the strength of the conclusions that can be drawn from this meta-analysis is limited by the fact that most of the included studies were retrospective. Third, majority of the studies analyzed a long period of observation (median over 4 years). This fact raises some doubts about whether a cohort effect may occur with present-day high-risk patients being dissimilar from those in the early part of the study. Fourth, no influence of the quality of TURBT/re-TURBT, novel prognostic factors (e.g., lymphovascular invasion and histological variants) was analyzed, yet such data were not reported in articles in a homogeneous way. Finally, there were some differences in study population homogeneity between the articles.
Conclusions
This meta-analysis shows that re-TURBT does not improve survival outcomes in patients with T1 tumors. We found that re-TURBT provided significant survival benefit only when both T1 LG and HG tumors were included in the analysis. Furthermore, high-quality, prospective, randomized controlled trials are necessary to make the final statement about the therapeutic role of re-TURBT in T1 NMIBC.
Footnotes
Authors' Contributions
The authors listed have made substantial contributions to the intellectual content of the article in the various sections described below: (a) conception and design: W.K., M.M., and E.X.; (b) acquisition of data: W.K., Ł.N., P.K., and M.W.; (c) analysis and interpretation of data: W.K., Ł.N., and S.P.; (d) drafting of the manuscript: W.K., Ł.N., M.M., and S.P.; (e) critical revision of the manuscript for important intellectual content: M.M., E.X., R.Z., A.M., and E.D.T.; (f) statistical analysis: A.T. and Ł.N.; and (g) administrative, technical, or material support: A.M. and E.D.T.
Author Disclosure Statement
None of the contributing authors have any conflicts of interest, including specific financial interests and relationships and affiliations relevant to the subject matter or materials discussed in the article.
Funding Information
No funding was received for this article.